
Abstract
BACKGROUND:
It is hypothesized that inherent differences in movement strategies exist between control subjects and those with a history of lower back pain (LBP). Previous motion analysis studies focus primarily on tracking spinal movements, neglecting the connection between the lower limbs and spinal function. Lack of knowledge surrounding the functional implications of LBP may explain the diversity in success from general treatments currently offered to LBP patients.
OBJECTIVE:
This pilot study evaluated the response of healthy controls and individuals with a history of LBP (hLBP) to a postural disturbance.
METHODS:
Volunteers (
RESULTS:
The healthy cohort utilized an upper body-focused strategy for balance control, with substantial activation of the external oblique muscles. The hLBP cohort implemented a lower limb-focused strategy, relying on activation of the semitendinosus and soleus muscles. No significant differences in joint range of motion were identified.
CONCLUSIONS:
These findings suggest that particular reactive movement patterns may indicate muscular deficits in subjects with hLBP. Identification of these deficits may aid in developing specific rehabilitation programs to prevent future LBP recurrence.
Introduction
Previous researchers have utilized in vitro studies, computational models, and human movement analysis to understand the function of the spine [1, 2, 3, 4]. However, the causes and optimal treatments for nonspecific lower back pain (LBP) remain unclear. Movement analysis, often performed using stereophotogrammetric systems, has allowed researchers and clinicians alike to quantify human movement during everyday activities [5, 6, 7]. However, previous spinal motion analysis studies focus primarily on tracking spinal movements, neglecting the connection between the lower limbs and spinal function [4, 8].
The causes of nonspecific back pain are not usually the result of an isolated injury within the spine, but instead are postulated to be the result of dysfunctional movement strategies within the spine and its base of support (the lower limb complex) [9]. For example, a patient standing with knee hyperextension and anterior pelvic rotation will influence the spine’s posture and resultant movement patterns. As such, for subsets of patients, lower back pain may be secondary to problems in the knees or pelvis, altering their spinal function and movement patterns. A study by Giles and Taylor into the impact of leg length inequality and function supports this concept [10]. Patients are often given generalized regimens to treat back pain, with variable outcomes between patients, which may relate to the range of underpinning causes [11, 12].
It has been shown that individuals with a history of lower back pain (hLBP) exhibit altered movement patterns that are caused by changes in both voluntary and reactive neuromuscular control [13, 14]. Therefore, an effective method for creating differentiable movement patterns is to subject a volunteer to a perturbation (postural disturbance). If delivered appropriately, perturbations create automatic movement patterns rather than movements that are consciously controlled by the volunteer [13]. Previous studies examining the response of the trunk to postural perturbations demonstrate that subjects with hLBP exhibit different EMG responses when compared to a healthy cohort [13, 15], including trunk stiffening and a delay in EMG activity by the trunk muscles. However, these responses may result from pain experienced by symptomatic hLBP subjects and perhaps do not reflect underlying changes in musculoskeletal control of both the spine and lower limb.
Therefore, the major aim of this exploratory study was to investigate the kinematics (i.e. body movements) of the spine, pelvis, and lower limbs following a postural disturbance in both healthy and hLBP subjects that are not currently in pain. A secondary aim of the project was to create a computational model of the kinematics of the spine-pelvis-lower limbs complex during a perturbation response to calculate the hip joint angles as well as facilitate interpretation of the response. The overlying hypothesis is that distinct differences in movement strategy will be observed between healthy controls and hLBP subjects in response to a balance disturbance.
Materials and methods
Subjects
This study was approved by the Imperial College Research Ethics Committee and written informed consent was obtained from all subjects. A convenience sample of 26 volunteers (Table 1) were recruited, of which 16 were healthy volunteers (12 females; 4 males) and 10 volunteers (6 females; 4 males) with hLBP. Volunteers were excluded from the study if they had a medical history of neurological disease or balance disorders, current acute lower back problems such as a herniated disc, uncorrected vision problems, presence of spinal deformities such as scoliosis, systemic infection, cardiovascular disorders, severe musculoskeletal deformity, were currently pregnant, had an injury to the lower extremity, or had surgery within three months prior to testing. Volunteers in the healthy group had no history of LBP and volunteers in the hLBP group had recurrent episodes of LBP at least once per year, with no specific diagnosis but were in remission with no pain at time of testing. Although 26 subjects were tested, full datasets were recorded for 24 subjects and therefore future analyses include only complete datasets.
Subject characteristics. The compiled characteristics of the subjects in the healthy and hLBP cohorts. There was not a significant difference found between the subjects in the two cohorts, although generally the hLBP subjects were heavier and older than the healthy cohort
Subject characteristics. The compiled characteristics of the subjects in the healthy and hLBP cohorts. There was not a significant difference found between the subjects in the two cohorts, although generally the hLBP subjects were heavier and older than the healthy cohort
Twenty-four individual reflective Vicon markers were used along with flat 3-marker clusters, placed on the calf and thigh to track the orientation of the segment in the capture volume. Foot and hip orientations were tracked using individual marker locations. Although both left and right limbs were captured during balance trials, only the right limb is considered in the following analyses. On the spine, a cluster method was used to track the lumbar, lower thoracic, and upper thoracic segments. The clusters placed on the spine consisted of three orthogonal reflective markers. Recent work demonstrated the validity of this particular cluster-based lower limb model [7]. Although skin movement is a concern in marker-based studies, with the small amount of movement observed during a perturbation, the skin-to-marker movement is minimal. Previous work has also investigated spine tracking with bone pins and fluoroscopy; however, these techniques are far more invasive for participants and the results are not significantly different than marker-based tracking in studies of gait and lateral bending [16, 17].
The markers allowed for body movements to be tracked and recorded by 10 Vicon T160s, 16-megapixel motion-capture cameras (Oxford, UK). Specifically, the single markers defined the subject’s anatomical frame and marker triads tracked the orientation of each segment in space [7].
The spine was separated into three regions: lumbar (L1–L5), lower thoracic (T7–T12), and upper thoracic (T1–T6). The thoracic region was split into two segments in order to observe different manifestations in the upper and lower portions. One marker was placed at either side of the spinous process of each vertebra of interest, including T1, T6, T7, T12, L1, and L5. These anatomical landmarks were tracked during the static portion of the trial. A 3-marker cluster was also placed at the center of each spinal segment, which was tracked during the dynamic portion of the trial. Marker data were sampled at 100 Hz. To remove spurious high-frequency marker motion, all marker data were filtered using a 4
In addition to kinematic measurements, electromyography (EMG) signals (sampling frequency,
In post-processing, DC offset was removed and EMG data was bandpass filtered using a 4th order filter between 10 and 400 Hz. Finally, the signal was rectified and a linear envelope was constructed using a 4th order low-pass filter of 6 Hz. Subsequently, processed EMG signals were normalized to muscle activation during quiet standing, and therefore all data presented is the fold-change in EMG activation in reference to quiet standing. It is known that subjects with hLBP are often unable to reach full maximal voluntary contraction, which may introduce variability into the study [18]. Thus, normalization to quiet standing was chosen to minimize error that could occur due to normalization from maximal voluntary contraction. Despite bilateral EMG collection, responses from the right muscles are considered in this analysis.
Testing procedure
The volunteer stood on the translating platform with safety bars on either side of the platform edge and was instructed to maintain his/her balance through a series of 31 anterior-posterior platform movements (0.7 second duration; distance of 7 cm). Subjects moved with an average peak velocity of 0.33
Computational modeling
A custom seven-segment unilateral joint kinematics model was developed using BodyBuilder (Vicon) based on the lower limb model developed by Cleather et al. [19]. Three segments, representing the lumbar, lower thoracic, and upper thoracic portions of the spine, were added to the existing model. Ankle, knee, hip, lumbar, lower thoracic, and upper thoracic joints connected the rigid body segments (Fig. 1). Each joint has the ability to move in three degrees of rotational freedom. In this study, we chose to model the skeletal motion of the spine and the right lower limb, and therefore acknowledge the limitations associated with neglecting the left lower limb.
Seven-segment joint kinematics model. (left) Simplified representation of the segments within the 3D kinematics model and the adjacent joints and (right) schematic of the full marker set, viewed from both the anterior and posterior perspectives.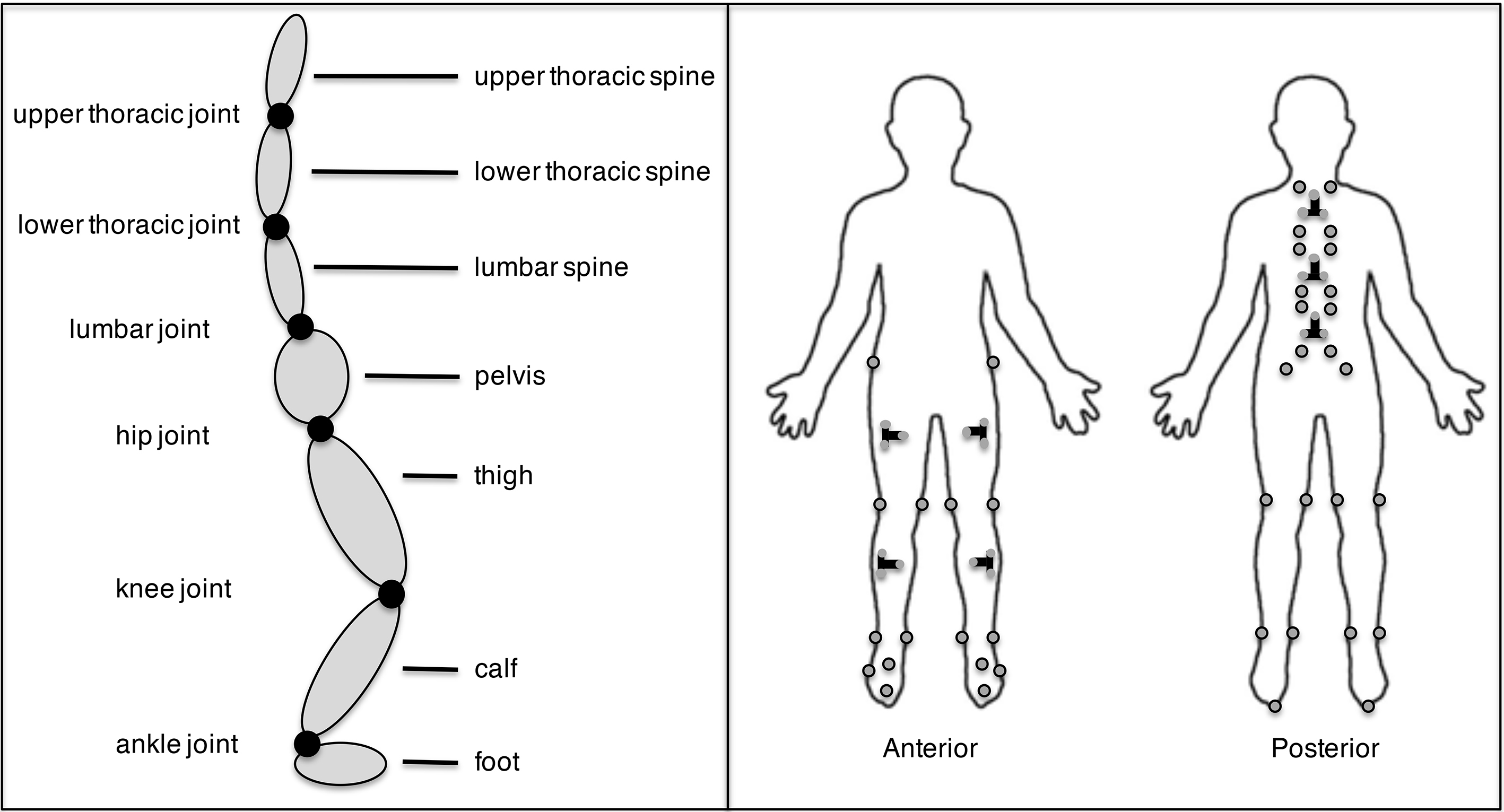
To solve for joint angles, the model relies on input from both individual markers, placed at bony landmarks, and tri-marker clusters that are centrally placed on body segments. Using the individual markers placed at bony landmarks, local landmark frames were calculated for each body segment during a static capture. The orientation of these frames follows the lower limb model developed by Cleather and Bull [19]. Additionally, the tri-marker clusters were used to track segment orientation using a local cluster frame. Utilizing transformation matrices, the cluster coordinate system was transformed into the anatomical frame for each segment. Subsequently, transformation matrices were used to relate the anatomical frame of each adjacent body segment to one another, thus placing both segments in the same coordinate frame. Euler angle decomposition was executed to calculate the flexion/ extension, abduction/adduction, and axial rotation angles at each joint.
Of particular importance to the accuracy of skeletal movement modeling is identification of the hip joint center (HJC) [20]. Unlike the knee or ankle, the HJC is impossible to directly track with reflective markers and therefore it must be estimated based on other pelvic measurements. Utilizing markers situated at the anterior superior iliac spine (ASIS) and posterior superior iliac spine (PSIS), the HJC was located using linear scaling compared to the Klein Horsmann dataset [21].
In order to capture the entirety of joint movement during each perturbation, kinematic data were partitioned into 2-second windows, one second prior to the peak velocity of platform movement and one second following the peak of platform movement. The mean of all 2-second windows was found for each subject (the mean kinematic perturbation curve) to evaluate timing and shape of joint kinematics. The range of motion (ROM) for each joint in response to every perturbation was calculated for each subject and the mean ROM for each joint was subsequently averaged across subjects in the healthy and hLBP cohorts. EMG data were also partitioned into 2-second windows, in the same manner as the kinematic data. The mean EMG perturbation curve was calculated for each subject. Peak EMG signal was measured for each perturbation for each subject at all joints studied and averaged across subjects.
Ternplots, three-sided plots on which three variables can be represented, were used to understand relationships between joint combinations in response to an unexpected perturbation. Ternplots are commonly used in the field of genetics [22], but to our knowledge have not been used to characterize the musculoskeletal system. These graphical depictions illustrate the relative contributions of each joint to movement across body segments. The ratio of joint movement contributions for each healthy control and subject with hLBP were plotted and an elliptical fit was applied to each plotted data set to identify group-level movement tendencies (Ternplot package, developed by Carl Sandrock and available via Matlab File Exchange). Elliptical fits were calculated in Matlab through an algebraic least-squares method of estimation using all points plotted for each cohort to obtain the sub-axis lengths of the ellipse and the tilt of the ellipse. The area enclosed by the ellipse gives an indication of the variability across the cohort.
Joint kinematics. Range of flexion/extension in the sagittal plane in response to a balance perturbation at six joints of the lower limb and trunk.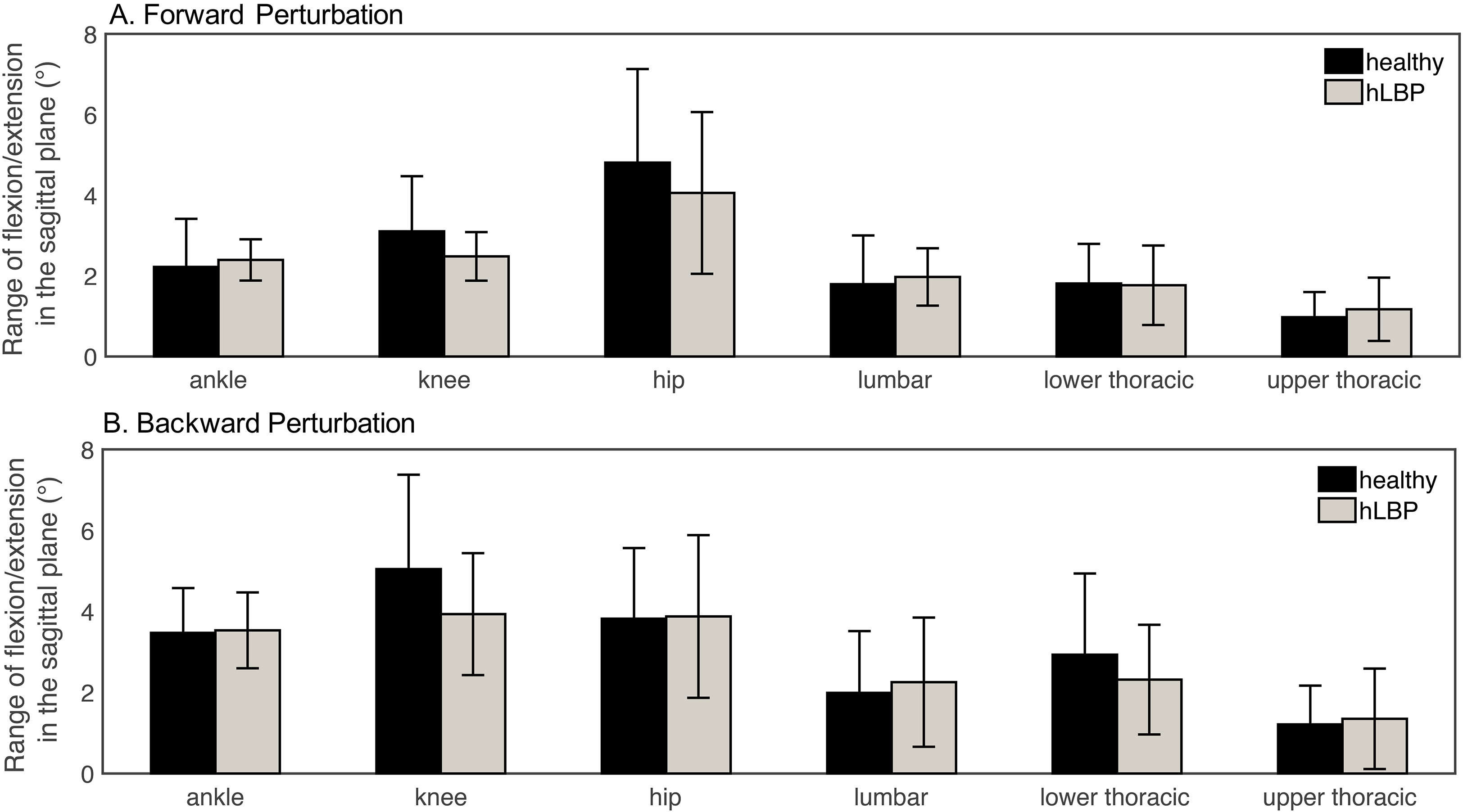
All data analyses were carried out using Matlab (Mathworks, Natick, MA, USA) and found to have a normal distribution using the Kolmogorov-Smirnov test at a 5% significance level. Group differences were assessed using the two-sample t-test and two-way ANOVAs.
Joint kinematics
Subjects were instructed to stand perpendicular to the axis of platform movement and thus, the majority of motion was seen in the sagittal plane. The average range of motion at each joint, derived from joint kinematics, is plotted for each joint in Fig. 2. The averaged kinematic curve between the healthy and hLBP cohorts is visibly similar in shape and timing. However, at several joints, including the knee and hip, the two cohorts exhibit apparent, though not statistically significant, differences, with the healthy cohort appearing to exhibit a larger ROM. Throughout the spinal segments, there is a high degree of variability in both the healthy and hLBP cohorts, possibility indicative of a range of spinal movement strategies. The ROM is consistent between the forward and backward perturbations (Fig. 2A and B), except at the knee joint, for which the ROM increased in the backwards direction of movement relative to forward in both the healthy and hLBP cohorts. There are no statistically significant differences in kinematic ROM of the spinal segments between the healthy and hLBP cohorts during forward or backwards movement.
In addition, to determine if there was any potential learning effect between perturbations, the consistency of the response over time was investigated. The mean kinematic responses from the perturbations, calculated individually for each subject in both cohorts, indicate no significant differences in movement patterns throughout the trial (
Kinematic ternplots
Ternplots were used to illustrate the relative movement of joint combinations across the lower limb and trunk. The hLBP group is contained to a more centralized region within the ternplot (Fig. 3A), whereas the healthy control group is scattered over a much wider region. There is a more consistent distribution of movement between the ankle, knee, and hip for hLBP subjects, whereas healthy subjects appear to use a more diverse range of balance maintenance techniques.
Relative movement of joints. Ternplots showing the relative movement at three adjacent joints, with axes shown as a percent of total movement between the three joints: (A) Lower limb, including the ankle, knee, and hip, (B) Interaction between upper and lower limb, including knee, hip, and lumbar spine, (C) Spine, including lumbar, lower thoracic, and upper thoracic spinal segments.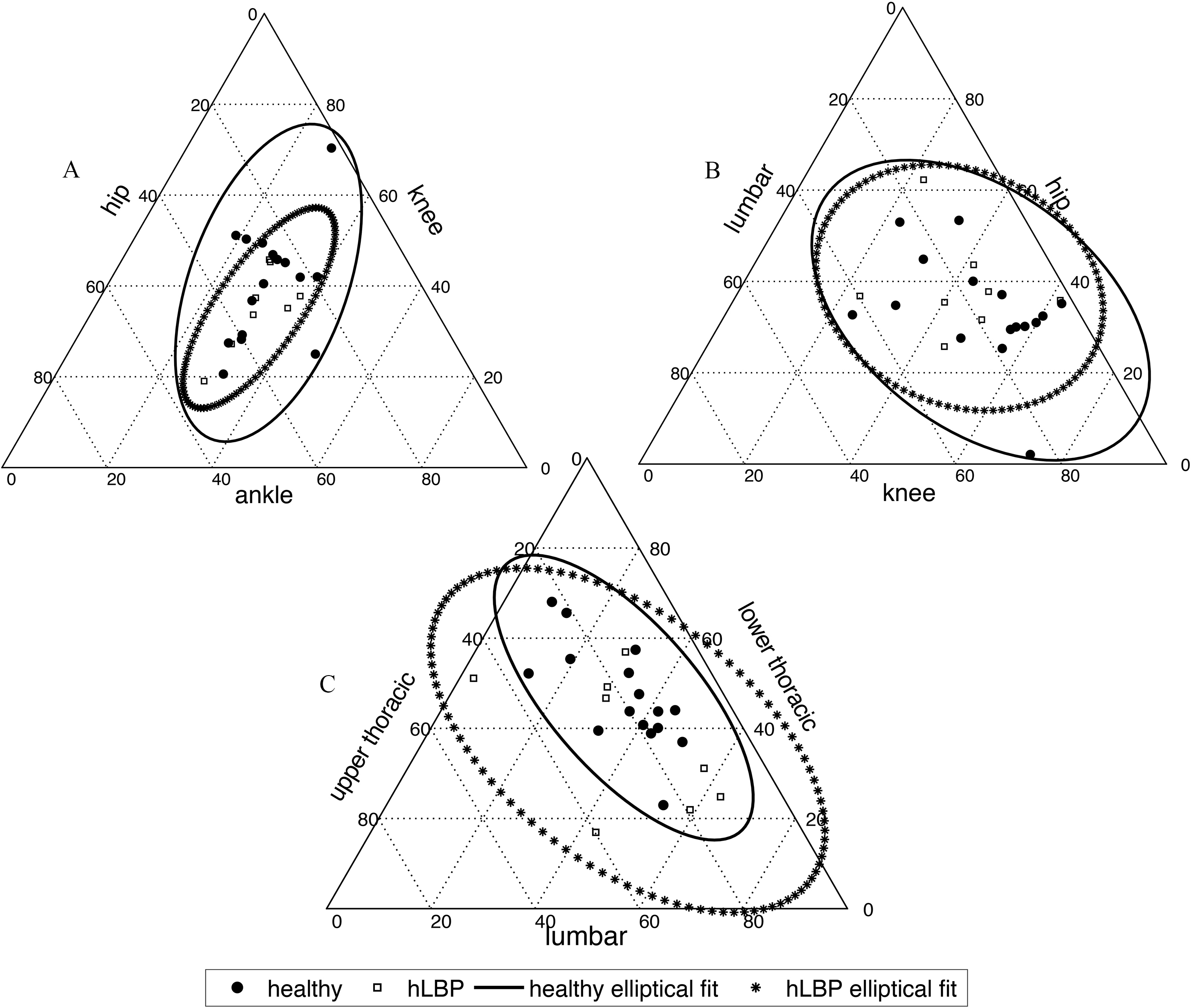
However, when creating the same plot for comparison of the spinal segments (Fig. 3C), the difference in ratios between the three segments (lumbar, lower thoracic, and upper thoracic) appears to be greater for the hLBP cohort, suggesting a wider variety of spinal movement strategies.
Similarly, a ternplot of the knee, hip, and lumbar joints identifies the relative ranges of motion between three joints situated through the epicenter of LBP (Fig. 3B). This ternplot demonstrates that some healthy subjects use knee-hip-lumbar balance strategies similar to hLBP subjects. However, healthy subjects tend to use a greater knee-based strategy than the hLBP subjects, as evidenced by the cluster of dots further along the knee ROM axis.
Muscle activation. Peak muscle activation for healthy and hLBP subjects during (A) forward and (B) backwards perturbations with error bars denoting standard deviation from the mean. Muscle activation during the perturbation is normalized to quiet standing.
The average EMG signal during quiet standing was calculated for the healthy and hLBP subjects and found to not be significantly different at any muscle between the two cohorts (Table 2). In the hLBP group, the resting soleus muscle demonstrated a nonsignificant trend (
Resting muscle activation. Average EMG signal for healthy and hLBP subjects during quiet standing
Resting muscle activation. Average EMG signal for healthy and hLBP subjects during quiet standing
The spine is a complex structure that is part of an intricate whole-body system that uses many strategies to maintain functional dynamic stability. Due to these aspects of spinal control, it is challenging to identify the precise problems that contribute to LBP, as many strategies can be used to compensate for system deficiencies. It is hypothesized that through exploration of these compensation strategies, treatment can be targeted to need rather than the current global approach, which assumes one treatment method works for all patients.
In this exploratory study, the greater activation of the SL and ST muscles by the hLBP cohort suggests that hLBP subjects employed a lower limb strategy to maintain balance on the moving platform. Despite changes in muscle activation of the lower limb, there is no significant difference in range of motion of the lower limb, pelvis, or spine. Reliance on the lower limb musculature, and possibly a reduced use of trunk musculature, makes a case for the movement strategy outlined in Fig. 5, in which the lower limb is held rigid by the SL and ST. In contrast, the healthy cohort appeared to use an upper body strategy, with a greater focus on trunk muscle contraction. However, the small cohort sizes and inability to match healthy and hLBP subjects necessitates further study of a larger population. Additionally, there is substantial variability observed across trunk, pelvis, and lower limb responses amongst different subjects, suggesting that people use a variety of strategies to maintain balance. Thus, a larger cohort of subjects may be necessary to adequately detect the potentially interesting range of strategies.
Observed changes in the hLBP cohort. Schematic of global changes observed within the hLBP cohort, including stiffening of the soleus and semitendinosus.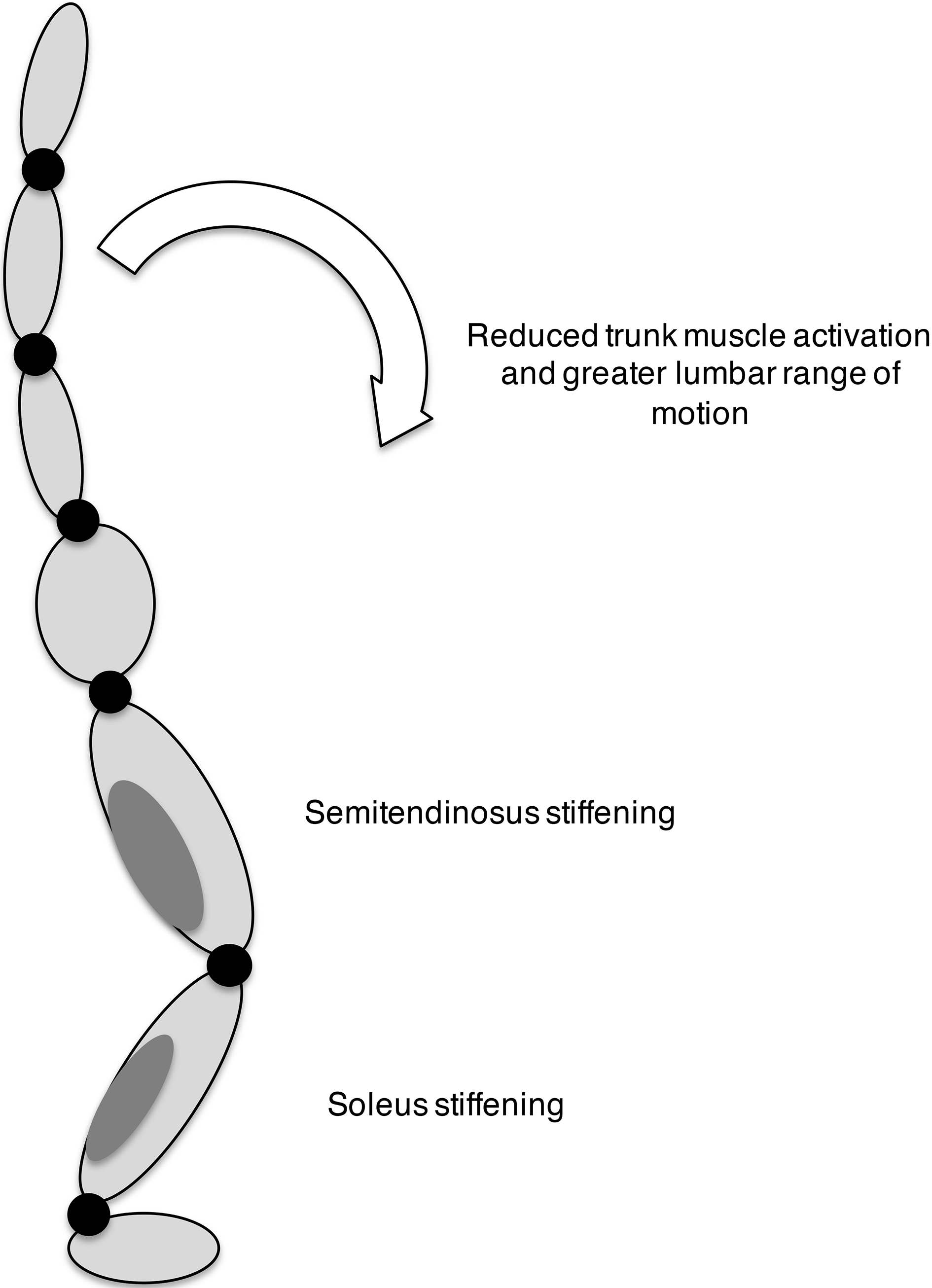
Similar to the present study, Jacobs et al. [13] explored the effect of hLBP on EMG activation in response to a postural perturbation. However, Jacobs et al. found increased resting muscle activation in hLBP subjects, which was not identified in the present study. This difference may be due to the cohorts selected as hLBP subjects and lower study power. The present study identified subjects with a history of LBP, but no current pain, while Jacobs et al. identified subjects that may have mild levels of pain. Examination of muscle activation during the perturbation response was reported by Jacobs et al. to be reduced in both the ankle and trunk muscles in the hLBP cohort relative to the healthy subjects. However, the present study found an increase in SL muscle activation in the hLBP group compared to the healthy cohort.
Although knowledge of these global strategies may be helpful in the development of rehabilitation programs, the results of this study further clarify the wide variability between subjects and highlight the need to study large populations of people with hLBP. Based on the variability in the present study, power analyses indicate that 27 to 68 subjects are required to adequately power future studies, depending on the primary outcome to be compared between cohorts (G*Power 3.1 software package). Future studies should also consider key cohort groups, including patients with degenerative disc disease and disc herniation. Secondly, results presented in this study are limited to movement in the sagittal plane and motion in the other planes may reveal important information.
Conclusion
Using a novel seven-segment model to process experimental marker data, it was noted that subjects with hLBP exhibited a different movement strategy than healthy subjects. The hLBP cohort was found to implement a lower limb-focused strategy, while healthy subjects may employ greater activation of trunk musculature. Additional work is required with a larger study population to further investigate differences, particularly in light of the high degree of variability in kinematic responses observed.
Footnotes
Acknowledgments
The authors thank the volunteers who participated in this study. MMS acknowledges a fellowship from the Whitaker International Program.
Conflict of interest
None to report.