
Abstract
BACKGROUND:
Rowing-related low back disorders may occur from inconsistent technique, high trunk flexion and training volumes, overactivation of paraspinal muscles, and fatigue.
OBJECTIVE:
To examine if kinesiology tape (KT) affixed to the trunk dorsum affects muscular co-activation and neuromuscular control to limit dangerous rowing movements and associated injuries.
METHODS:
Participants (
RESULTS:
Responding participants (
CONCLUSION:
KT can be an effective at reducing mean trunk co-activation during a rowing trial in the flexed catch position. Variable responses suggest that further work is necessary to optimize the efficacy of sensory cues derived from KT during rowing movements.
Introduction
Low back disorders (LBDs) are one of the largest health-related complaints among rowing athletes [1, 2]. One potential method to mitigate some of these risk factors is by using a supplementary sensory stimulus to cue the neuromuscular control of a movement. Supporting literature suggests that tactile stimuli delivered via a skin adhesive may be effective to augment the motor control of the trunk and lower extremities during sagittal plane spine movement tasks such as lifting [3, 4]. One style of athletic tape receiving considerable interest is elastic kinesiology tape (KT) [5, 6]. KT was developed by Japanese chiropractor Dr. Kenso Kase in the 1970s as a therapeutic tape for treating sports injuries and other disorders [7]. The intention of KT is to relieve pain, prevent, and treat injured muscles and joints while lifting the skin to allow for improved blood and lymph flow [8]. KT application has various proposed benefits which include improvements to proprioception, lymphatic draining, joint stability, and joint positioning, while also reducing pain and fatigue [9]. To facilitate improved proprioception, KT has the potential to target mechanoreceptors embedded within the skin, deep fascia, muscle, and joint tissues as the tape can transfer force through these tissues to any embedded mechanosensitive afferent [10, 11]. Further, pain relieving effects can be obtained by the tape’s purported ability to lift the skin and reduce excess pressure or mechanical deformation on any subcutaneous nociceptor [12, 13]. Recent research has noted enhanced therapeutic effects in reducing pain and improving disability when using KT as an adjunctive therapy in individuals with chronic lower back pain [14]. Despite this, the potential effects of KT on the control of a highly dynamic aerobic movement of the lumbar spine are largely unclear.
A 2000 m rowing regatta is a style of competitive rowing that is highly aerobic in nature. Often indoor ergometers are used for training, fitness testing, and crew selection through seat racing to select the fastest and fittest rowers [15]. While scull rowing (two oars), the rowing stroke consists of the “drive” and “recovery” phase. The “recovery” phase starts when removing the oars in a feathered position from the water (parallel to water). The recovery phase is sequenced as arms, hips, legs (full flexion at the knee). The “drive” phase has the oars “squared” (perpendicular to water) and begins in the “catch” position with arms fully extended, legs and trunk in complete flexion [16]. The drive phase is sequenced in reverse of the recovery phase as knees, hips, lumbar spine, and shoulders begin to extend. As the oars enter the water, quadricep leg muscles are activated to apply force through knee extension and contracting the gluteal muscles, to reach the “finish” or “release” position of a fully extended trunk with arm flexion at the chest [17].
Previous research suggests that repeated high flexion postures are a potential risk factor for LBDs because of repeated strain to ligamentous structures, which may cause damage to intervertebral discs [18]. Fatigue can also contribute to these greater high-risk postures by generating increased lumbar spine flexion at the catch position. This may indicate that an increased training volume on an ergometer in the off-season may cause an LBD risk for rowers [19]. Throughout scientific literature, there is inconsistency in the utility of KT to enhance performance outcomes in training and in sports competition. Given this, there is a clear need to explore the potential utility of KT as a supplementary sensory stimulus to both change the coordination of a rowing-based movement, and potentially reduce the mechanical risks associated with the development of LBDs. This is a natural extension of research assessing the utility of KT to evoke similar changes in the motor control of the lumbar spine during slow and constrained lumbar movement [4, 20, 21].
Despite large quantities of KT research, there is very little quality evidence for KT applications to either improve performance or prevent LBDs [5, 22, 23]. Further studies are required to clarify functional utility of KT approaches related to areas of athletic injury prevention and improving performance. The purpose of this study is to examine if KT-mediated sensory feedback has the capacity to augment the neuromuscular control of a rowing movement, with particular interest in the ability of KT to increase trunk muscle co-activation and reduce perceived fatiguability. It was hypothesized that a positive response to the KT-mediated feedback would result in reduced lumbar flexion, which would demonstrate increases in trunk muscle co-activation and reduced perceived fatiguability.
Demographics and anthropometrics of all participants (
18), and those partitioned into responder (
5) and non-responder (
13) groups. All data are presented as means
standard errors
Demographics and anthropometrics of all participants (
Participants
Eighteen healthy, amateur or elite rowing athletes, aged 18–30 years, participated in the current study. To guide the a priori sample size estimation, two studies were reviewed which utilized tactile cues to elicit a reduction in lumbar ROM during spine flexion movements [4, 20]. Collectively the effect sizes (Cohen’s
Protocol
A Noraxon Ultium Wireless Electromyography (EMG) system quantified time-varying electromyograms. Prior to electrode and sensor application, the skin was shaved and cleansed with rubbing alcohol. All electrodes were placed according to Surface EMG for Non-Invasive Assessment of Muscles (SENIAM) guidelines. Specifically, EMG data was collected bilaterally from the rectus femoris (RF), vastus lateralis (VL), rectus abdominis (RA), external obliques (EO), thoracic erector spinae (TES), gluteus medius (GMED), and biceps femoris (BF) [15]. EMG sensors had an interelectrode distance of 20 mm and were placed bilaterally on the muscles of interest, parallel with muscle fibers [26]. Raw EMG data were sampled at a rate of 2000 Hz and were exported as .csv files for further analysis in MATLAB (2020b, MathWorks Inc.).
Concurrent acquisition of 3D body kinematic data was facilitated by a set of 17 wireless inertial measurement units (IMUs) (XSens MVN Awinda). IMU sensors were placed on the head via headband, sternum and shoulders via neoprene shirt, upper arms (UA), lower arms (LA), upper legs (UL), lower legs (LL), pelvis, and feet as per manufacturer instructions. Full body dimensions of the participants were measured (cm), including body height, foot or shoe length, shoulder height, elbow span, wrist span, arm span, hip height, hip width, knee height, ankle height, and extra shoe or sole thickness. These data were used to refine a kinematic model within XSens MVN Analyse software. Following HD re-processing, all kinematic data (including ZYX joint angles) were extracted at a rate of 60 Hz, and subsequently saved as .xlsx files for further analysis in MATLAB (2020b, MathWorks Inc.).
Following instrumentation, each participant completed a self-directed five-minute warm-up to fine tune their preferred setup, a consistent stroke rate, and drag factor (DF) on a Concept 2 rowing ergometer. Specifically, participants set the appropriate DF as per weight category (i.e., lightweight, or open class men and women) and an appropriate race pace that they could maintain for both rowing bouts. Following the warmup, two 2000 m rowing bouts (BASELINE and KT) were completed at race pace, with each separated by a 30-minute rest period to mitigate any effects of neuromuscular fatigue on the study outcomes. During the rest period, three pre-cut 15 cm strips (two vertical, one horizontal) of KT were applied at a perceived 60% tension superficial to the lumbar and thoracic paraspinal muscles in an area that was shaved and prepped with rubbing alcohol (Fig. 1). All KT application was completed with the participant in a neutral standing posture. The mechanism of effect of tension and direction of tape is based on supplier’s guidelines and the direction of underlying muscle fibres. Bilaterally and longitudinally along the paravertebral muscles, KT was anchored medially to the iliac crest at approximately L4 vertebral level [27]. When applying, 100% tension is applied then modulated back to 60% tension and placed laterally of approximately T7 vertebral level (below scapula). Both anchored ends of the tape use 0% stretch. The tape is activated on the paraspinals by rubbing on the adhesive. The horizontal tape mitigates any torsion effects in the lumbopelvic region.
Following the application of KT (prior to the second rowing bout), participants were instructed to “adjust their movement pattern during the rowing movement to minimize the sensation of tension caused by the KT affixed to their low back” to limit conscious proprioceptive changes in posture and ROM [3, 11]. In addition to kinematic and EMG data, subjective fatigue data were obtained during both rowing bouts. Specifically, participants were instructed to complete a Borg-10 rating of perceived exertion (RPE) scale with anchors placed at rest (0), really easy (1), easy (2), moderate (3), sort of hard (4), hard (5–6), really hard (7–8), really really hard (9), and maximal exertion (10) immediately preceding and following each simulated racing bout.
Pictorial demonstration of KT application for the second 2000 m trial. KT is applied using the anchor (vertical tape) and zone (horizontal tape) methods on stretch bilaterally, superficial to the lumbar and thoracic paraspinals. The tape is applied at a pre-stretch of 60%. The horizontal tape is to limit torsion movements of the spine and symmetry of the hip joint.
To understand the effect of KT on perceived fatiguability, the POST-PRE difference in RPE score was compared across BASELINE to KT conditions to discern if the addition of KT has any potential protective effects against acute muscle fatigue. Absolute sagittal plane trunk angles were used to partition all joint angle data (i.e., catch-to-catch position), after which each stroke was time-normalized to 101 frames. From these joint angle ensembles (representing all rowing strokes from 0–2000 m), mean maximum and minimum sagittal plane joint angle data of the lumbar spine, shoulders, knees, hips, and ankles were analysed to assess the impacts of KT on trunk and lower extremity ROM. Further, to partition participants into responders and non-responders the average maximum lumbar flexion was utilized. Specifically, those who reduced mean maximum lumbar flexion in response to the KT were classified as responders, whereas those who had an equal or greater mean maximum lumbar flexion were classified as non-responders.
Surface EMG waveforms were processed to yield agonist-antagonist co-activation indices (CAIs) about the lumbar spine, hip, and knee. To accomplish this, raw EMG signals were full wave rectified and filtered using a zero-lag Butterworth filter with an effective low-pass cut off of 10 Hz [28]. Following this, signals were segmented into individual cycles and subsequently time-normalized to 101 frames using events derived from the forward flexion of the trunk, mirroring the analysis of the kinematic data. After segmentation, peak surface EMG amplitudes were calculated for each cycle of the rowing bout, and the 95th percentile peak amplitude for each muscle was used to facilitate the amplitude normalization of each respective muscle (as a percentage of this value) prior to the computation of each CAI. Although conceptually similar to maximum voluntary contraction normalization, this approach facilitates the representation of all data relative to data derived from a similar neural condition (i.e., dynamic rowing) rather than simple isometric activation, while also avoiding any effects from remaining spurious noise. To estimate agonist-antagonist CAIs the following formula was used [6, 29]:
Specifically, at each time-step (
Summary of discrete outcomes related to joint range of motion, and perceptions of fatigue. All data are presented as means
standard errors
Summary of discrete outcomes related to joint range of motion, and perceptions of fatigue. All data are presented as means
All statistical analyses were completed in SAS (version 9.4). Independent variables for these analyses included the rowing condition (i.e., BASELINE vs. KT) and the responder group (i.e., responder vs. non-responder). Dependent variables included the maximum and minimum joint angles, as well as the maximum, mean, and minimum CAI values. All outcomes were analysed using a two-way ANOVA (condition*response) with any statistically significant interactions being further analysed using a Tukey-Kramer /post hoc/ analyses (
Results
The demographic characteristics of all responders and non-responders is reported in Table 1.
Fatigue (RPE)
RPE was observed to increase as a response to the 2000 m rowing bout across both groups (i.e., responders and non-responders to KT) and conditions (i.e., BASELINE and KT). No significant group (
Average joint posture and ROM
For the majority of joints, there were no significant changes in the average maximum or minimum joint postures. Despite this, the average maximum (
Co-Activation Index Waveforms. (a) Trunk ((RA 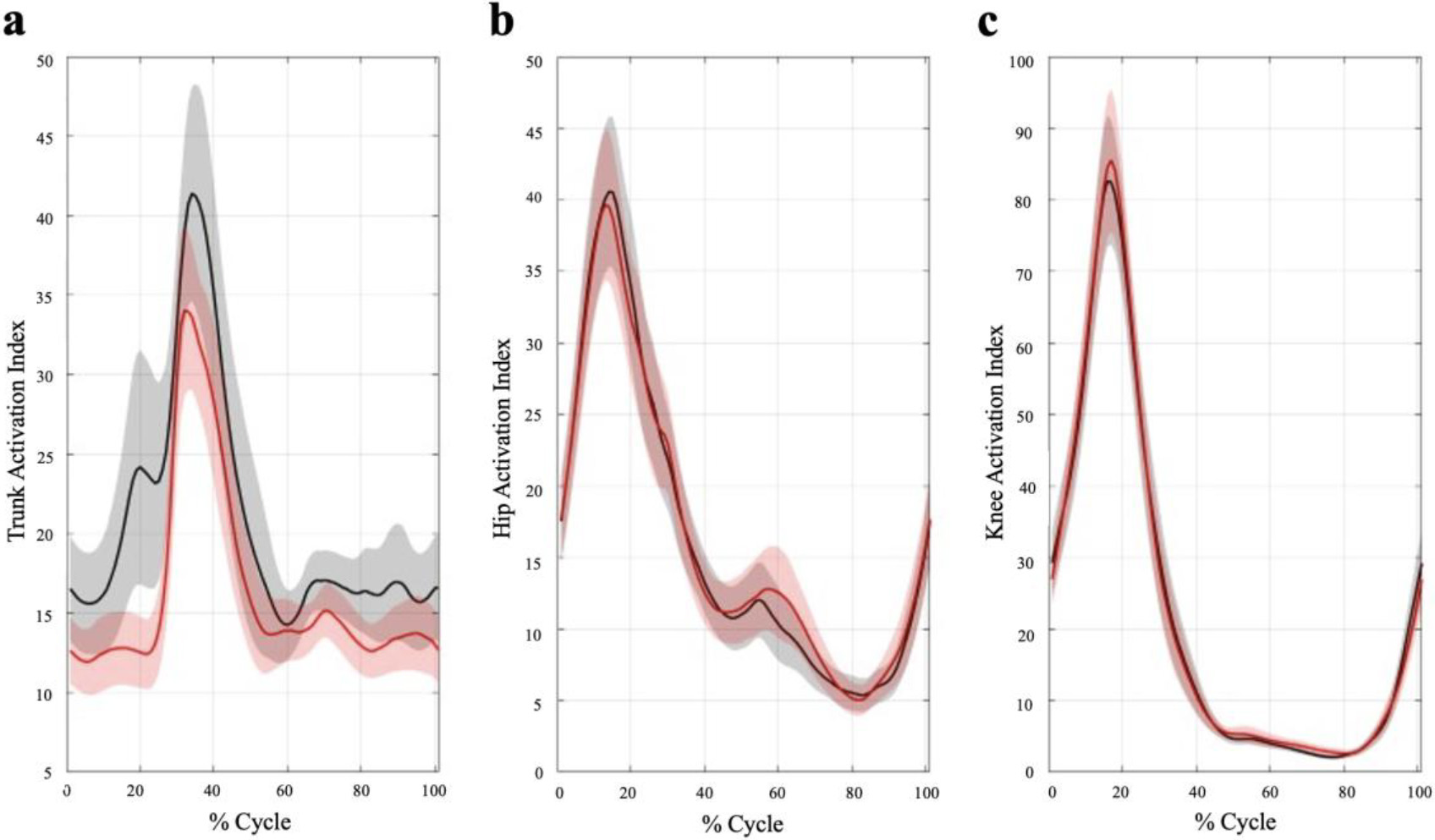
Average maximum, mean, and minimum (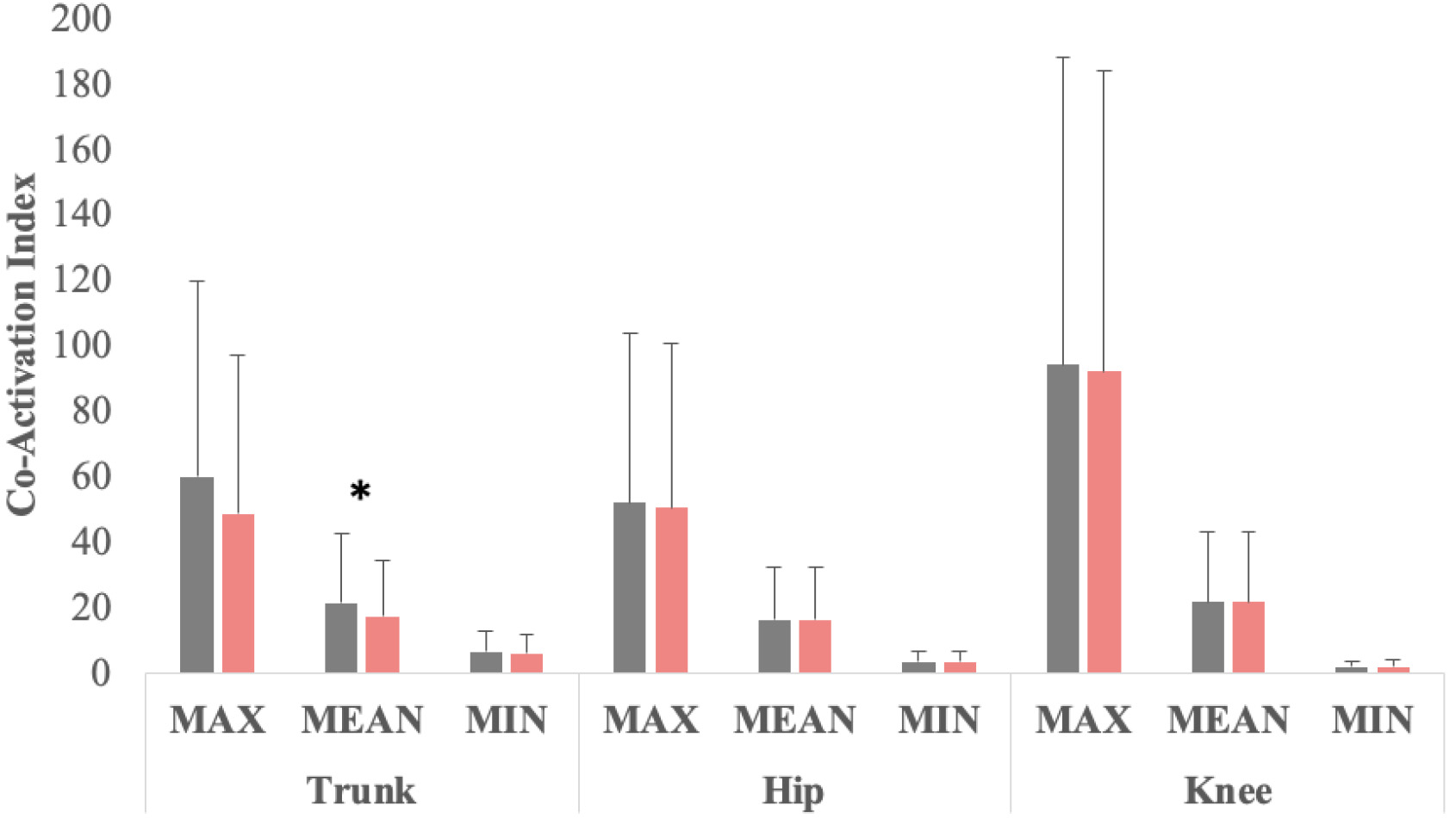
No statistically significant group, condition, or interactions were observed for the average maximum, mean, or minimum hip or knee flexion-extension CAIs. Despite this, a significant condition effect was observed for the mean trunk flexion-extension CAI such that the BASELINE condition was statistically larger than the KT condition (
Discussion
The purpose of this study was to assess the effects of tactile cues, derived from KT placed on the skin of the trunk dorsum, on the neuromuscular control of a dynamic performance-based task (i.e., rowing movement). Based on previous research during sagittal plane movement tasks, it was hypothesized that KT would result in a reduced maximum lumbar flexion. Evidence shows a reduced peak flexion would result in concomitant redistributions of motion across joints of the lower extremity [3, 11]. These findings are consistent with altering neuromuscular control patterns using tactile feedback affecting movement variability during a rowing trial. With a reduction in peak lumbar flexion, it was also hypothesized that KT would result in an increase lumbar agonist-antagonist co-activation and a reduction of perceived fatigue. The results of the study largely refute these hypotheses. Although responses to KT were notably heterogenous, some group-level effects of KT on trunk muscle co-activation were observed suggesting some effects of KT may reduce the degree of trunk muscle agonist-antagonist co-activation indices across the rowing cycle. This is in opposition to the original hypothesis where an increase in agonist-antagonist co-activation was expected to brake forward flexion momentum and reduce forward flexion ROM in response to the supplementary sensory stimuli derived from the KT. In contrast, Fig. 2a demonstrates a reduction in trunk co-activation in the catch position (i.e., high flexion) in response to KT. By reducing lumbar flexion in a dangerous posture for a subset of participants (i.e., responders) while also reducing agonist-antagonist co-activation (across both responding and non-responding participants), these findings suggest that KT has the potential to reduce the exposure of the lumbar spine to excessively high muscle and posture-mediated internal joint forces while concurrently improving rowing performance by reducing the metabolically inefficiency of agonist-antagonist muscle co-activation.
The controversy of therapeutic effects of KT lies in how the stimulus is perceived and how the body responds to tactile cues. Previous work has suggested that KT has the capacity to systematically evoke mechanical strain of skin and superficial muscles of the lower extremity [10, 11], suggesting the capacity of KT to be used as a supplementary kinaesthetic cue to facilitate a desirable motor change. The motor changes of interest in this study include both the reduction of lumbar flexion and the potential change in the co-activation of the trunk musculature during dynamic rowing bouts to reduce risk of LBDs. Further to this, tactile cues have been used to evoke both a re-distribution of movement within the spinal column [3], as well as between the lumbar spine and joints of the lower extremity [4] during slow and controlled spine flexion-based movements. This literature found a reduction in lumbar spine flexion yet was compensated for by increases in hip and knee flexion, indicating a re-distribution across joints [11]. Mirroring the current work, the participants were instructed to pay attention to the sensations elicited by the tape, such that they were instructed to minimize the amount of stretch they felt while moving to optimize the tape’s utility as a supplementary tactile cue [4]. These instructions to minimize tape stretch sensation encourages the re-distributing of movement away from the lumbar region and into neighbouring joints. The aim of this research was to assess the utility of KT-derived supplementary sensory feedback on the control of a highly aerobic, closed chain, performance-based task, with a particular focus on the assessment of the mechanics of lumbar spine rather than the lower extremities [30, 31]. For a subset of the participants (i.e., responders,
Other literature has demonstrated that the posture of the spinal column, and neuromuscular characteristics of the paraspinal musculature, have the capacity to vary through the generation of muscle fatigue throughout a dynamic rowing trial [30]. Despite this, very little research has assessed the capacity to augment the neuromuscular control of rowing movements with supplementary sensory stimuli. Further, very little research has assessed the therapeutic potential of KT-derived sensory stimuli to evoke changes in agonist-antagonist co-activation. A secondary aim of the current work was to assess if KT-derived sensory stimuli could evoke a change in the agonist-antagonist co-activation of the trunk musculature. Figure 2a suggests that KT has the capacity to reduce trunk muscle co-activation, and that this effect was present in both response groups (i.e., those with a notable reduction in lumbar ROM, and those without). Although metabolically inefficient, muscle co-activation would both effectively enhance lumbar stability, while also potentially accelerating neuromuscular controls including fatigue.
The previous work assessing rowing biomechanics has provided a description of sequencing, force production, and kinematics of a conventional rowing stroke [1, 16]; however, relatively little work has quantified the within and between athlete variation in rowing mechanics, nor the capacity to evoke a systematic motor change within a single athlete to optimize performance or avoid injury. Previous work has identified the stabilizing role of the trunk musculature within a rowing movement; however, despite this, the prevalence of LBDs in rowing athletes remains high [2, 33, 34]. The current study expands on this literature by assessing the efficacy of a commonly used therapeutic aid in performance settings (i.e., KT). This study quantifies postural changes among rowing athletes, while noting heterogenous responses through the reduction of peak lumbar flexion. At the neuromuscular level, all participants had notable reductions in agonist-antagonist co-activation with the application of KT, no matter whether a reduction in peak lumbar flexion (i.e., KT response) was observed.
Limitations and considerations for future work
Certain considerations should be made when interpreting the results of this study. Only average maximum and minimum flexion-extension joint ROMs and trunk CAIs were investigated in this study with rowing-specific scenarios. It is notable to address the potential rehabilitation utility of KT-derived sensory stimuli to evoke changes in a wide range of performance scenarios, including movements taking place outside of the sagittal plane. In addition, the low response rate to KT also suggests further investigation is necessary to optimize KT’s implementation in decreasing LBD risks across a greater population. Specifically, care needs to be taken to address an athlete’s perceptual or conscious abilities and biases to optimize the utility of sensory feedback to evoke changes in lumbar movement. Specifically, this study is limited to only 60% tension and a variety of pre-strains should be compared to ensure all participants are able to perceive the tactile cue and respond to the intervention, even in demanding performance-based settings where multiple internal and external stimuli require attention. Finally, due to convenience sampling, the sample for the current study is biased towards university-level rowing athletes, a majority of whom were from the same rowing team or coaching staff. It is possible that different responses may be present in different age or performance sub-demographics, and these should be explored with further research. Future work is required to both optimize the pre-strain of any KT applied to the trunk dorsum to induce a perceptible skin stretching stimulus at high lumbar flexion (including a range of pre-strains about the 60% used here). It should address the utility of such stimuli across a wide range of performance-based movements (including open-chain exercises, and on-water rowing) to assess the utility of KT-derived sensory stimuli to evoke changes in joint kinematics across more complex, or stability-challenging performance tasks. By examining spine stability enhancement and protecting against objective indicators of muscle fatigue (i.e., EMG spectral characteristics) may help quantify the potential effects of KT-derived sensory stimuli (e.g., [30]). In addition to EMG characteristics, it is important to assess the potential role of KT-derived sensory stimuli to evoke changes in both spatial measures of joint posture and EMG-derived CAIs, as well as spatiotemporal measures related to joint coordination, and performance.
Conclusions
This study investigated the effects of KT-derived supplementary sensory feedback on the kinematics and neuromuscular control of a dynamic rowing movement. The postural responses to KT varied with some participants demonstrating a reduction in lumbar flexion, which refutes the hypothesis of increasing mean lumbar co-activation indices in response to KT. Despite some participants presenting with reduced lumbar flexion in response to KT, no statistically significant changes were seen in neighbouring joints to suggest a redistribution of motion to from the lumbar spine to lower extremities [3, 4]. Despite the absence of postural changes, this research suggests that KT may be effective in reducing LBD risks in dangerous positions and improve performance for rowing athletes through reduction of trunk muscle co-activation. Specific reductions in trunk muscle co-activation were noted in the catch or repeated high flexion position where the spine is in a flexed posture and the paraspinal musculature is beginning to bear load during the drive phase of a rowing stroke. The biomechanical response to tactile stimuli suggests it is necessary to both optimize the application of KT in sport-based settings, as well as to assess the effects of KT-derived sensor stimuli in open-chain performance-based tasks outside of the sagittal plane.
Author contributions
JW designed the study, performed data collections, and drafted/revised the manuscript. AB and CV assisted with data collections, performed data analysis, and assisted in the drafting and revision of the manuscript. SMB supervised junior authors, conceived, and designed statistical analysis, obtained research ethics approval, and assisted in the drafting and revision of the manuscript. All authors read and approved the final manuscript.
Data availability statement
The authors confirm the data supporting the findings are included within the article. Raw data are available from the corresponding author upon reasonable request.
Ethical approval
This study was approved by Brock University’s Research Ethics Board (REB 19–310), St. Catharines, ON, Canada.
Funding
This project was funded by the Natural Sciences and Engineering Research Council (NSERC) of Canada (RGPIN-2020-05195) and supported by Concept 2.
Informed consent
Informed consent was obtained prior to performing the data collection.
Footnotes
Acknowledgments
The authors thank the participants of this study for their valuable contributions to the research.
Conflict of interest
The authors declare that they have no conflict of interest.