
Abstract
BACKGROUND:
Nerve injury due to a movable cystic mass during knee motion is a rare neuropathy, which can be diagnosed precisely using a dynamic ultrasonogram.
OBJECTIVE:
To present a case with foot drop and common peroneal neuropathy that involved a movable cystic mass during knee flexion adjacent to the proximal tibiofibular joint.
METHODS:
Case report.
RESULTS:
A 47-year-old female was referred to our institute for a right foot drop. Common peroneal nerve (CPN) injury was confirmed by an electrophysiologic study. Upon a dynamic ultrasonographic study during knee flexion, a cystic mass was found that was not scanned on the static images. The mass displaced the lateral head of the gastrocnemius muscle and CPN. A cystic mass that was adjacent to the proximal tibiofibular joint was confirmed by magnetic resonance imaging.
CONCLUSION:
Ultrasonography is a convenient first-line diagnostic method of peripheral nerve disorder by virtue of its higher spatial resolution, cost-effectiveness, and prompt diagnosis. The real-time and dynamic scanning attributes are the discriminative merits of this imaging tool. This case report suggests that CPN compression occurred due to a movable cystic mass during knee flexion. Dynamic ultrasonographic evaluations could be helpful to diagnose pathologic musculoskeletal conditions.
Introduction
Peripheral neuropathy that is caused by a mass is rare around the knee joint. Masses related to mononeuropathy including ganglion, hematoma, schwannoma, intraneural cyst, and fabella have been reported as case studies.
The knee joint is the largest human joint [1]. The large hinge joint and circumferential musculature has a simple motion with a wide range and has a major role in shifting and bearing the body weight, even on flexion. The muscles and ligaments around the knee joint change in conformation during dynamic motion. Therefore, a dynamic examination is important to evaluate knee injury including neuropathy.
During the examination, several specific diagnostic manipulations are used to evoke a symptom, based on the dynamic mechanism of the knee. However, clinical imaging is static, and, in many cases, will not correlate with the dynamic examinations. Ultrasonography may bridge the gap between the clinical findings and image data. Prior results have demonstrated the validity of ultrasonography for knee dynamics [2].
Transverse sonogram (A, B) and T2-weighted magnetic resonance imaging (C, D) of the right knee. (A) shows the common peroneal nerve (dotted line) around the fibular head (FH) during knee extension. (B) shows a hypoechoic mass (asterisks) superficial to the fibular head during knee flexion. The mass was located under the lateral head of the gastrocnemius muscle (GCL) and adjacent to the circumferential fibular vessels (Ve). The proximal GCL muscle was pushed back (arrowhead), and the common peroneal nerve was compressed during knee flexion. (C) and (D) reveal a round mass (open arrow) adjacent to the proximal tibiofibular joint. The shortest distance between the mass and common peroneal nerve (dotted line) was about 11.5 mm.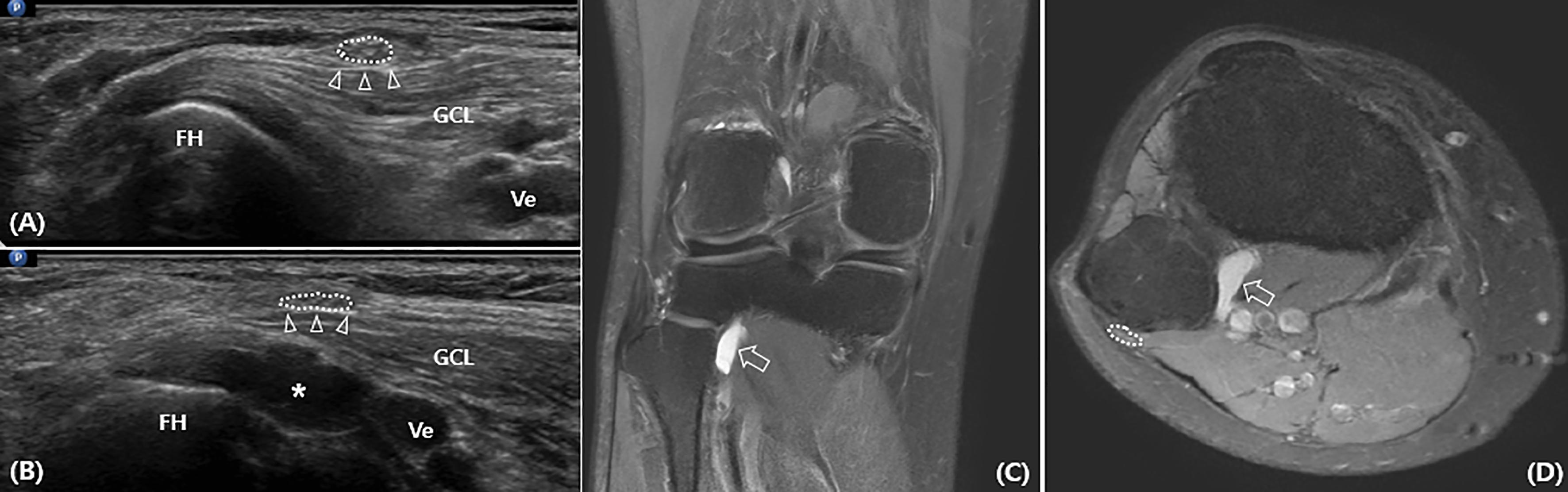
In the current case report, a common peroneal nerve (CPN) injury caused by a movable cystic mass during knee flexion was diagnosed using a dynamic ultrasonographic evaluation.
A 47-year-old female with a right foot drop was referred from the orthopedic department. The patient had fractured her right fifth metatarsal shaft fracture after falling down and had been immobilized in an ankle-foot cast for 6 weeks. A careful physical examination revealed weakness of the ankle dorsiflexor and long extensor of the toe trace grade according to the medical research council scale, and a positive Tinel’s sign on the posterior fibular head during knee flexion. The patient complained about aggravation of a tingling sensation on the right dorsal foot during knee flexion. During walking, the patient had a pattern of steppage and some atrophic appearances of pretibial muscles.
An electrophysiologic study revealed amplitude drops and decreased velocities of the compound muscle action potentials across the fibular head upon the recording of both the extensor digitorum brevis and tibialis anterior muscles. The needle electromyogram exhibited denervating insertional activities and polyphasic motor unit action potentials of the tibialis anterior, peroneus longus, extensor digitorum brevis muscles, and normal potentials of the short head of biceps femoris muscle. To specify the lesion site precisely, a nerve conduction study of the segmental common peroneal nerve was designed. The active recording electrode was secured just distal to or at the fibular neck, and the stimulating electrode was placed on the medial border of the lateral hamstring tendon at the popliteal crease. The amplitude of the compound nerve action potentials on the affected side resulted in less than half of that found in the sound side. The electrophysiologic diagnosis was made of a right common peroneal neuropathy around the knee.
In order to evaluate the lesion around the fibular head, ultrasonographic scanning using a 5–12 MHz linear array transducer (HD15 Ultrasound System; Philips, Bothell, WA) on the knee was applied. Initially, no abnormal findings around the fibular head on the knee extension posture were evident. However, based on the clinical findings that the Tinel’s sign on the fibular head was only observed during knee flexion, a dynamic ultrasonographic study was conducted during knee flexion. An abnormal small hypoechogenic round mass around the posterolateral fibular head on the transverse plane was revealed upon knee semiflexion. The mass was located under the lateral head of the gastrocnemius muscle and along the posteriolateral surface of the fibular head (Fig. 1). Because of this mass migration, the proximal lateral head of gastrocnemius was pushed back, and the CPN on the proximal lateral head of the gastrocnemius muscle was displaced and compressed indirectly.
To confirm the unrevealed injury of the knee, magnetic resonance imaging (MRI) was conducted. The non-contrast-enhanced 11.5
The patient was treated conservatively with prevention prolonged knee flexion. One month later, the ankle dorsiflexor power had improved to fair grade, and the patient did not complain of other symptoms.
Discussion
The CPN typically originates from the sciatic nerve at the apex of the popliteal fossa and courses along the medial margin of the biceps femoris muscle, which winds around the neck of the fibula. It has three articular branches to innervate the knee and proximal talofibular joints and two cutaneous branches (i.e., the lateral sural and sural communicating nerves), and then bifurcates the deep and superficial peroneal nerves. This short nerve segment, which courses into the fibular tunnel at approximately 1-centimeter distal to the head of the fibula, is clinically important for physicians. The tunnel consists of a thick fibrous arch formed by the deep aponeurosis of the fibularis longus muscle. This arch can contribute to irritation during dynamic motions, such as running, and is prone to entrapment on some prolonged postures.
Posture-related common peroneal neuropathy is considered a diagnostic feature of foot drop after prolonged positions, such as squatting, kneeling or habitual leg crossing while seated. Posture-related neuropathy involves the fibrous fibular tunnel, which indicates that the posterolateral part of knee suffers from structural and manometric alteration during motion. To prove posture-induced peroneal neuropathy, any clinical evidence, with the exception of obtaining a precise history, may not be enough. The patient in the present case said that she did not have a habit of adopting the aforementioned positions.
Foot drop after casting due to lower extremity injury is most frequently considered to be compressive peroneal neuropathy. Regardless of the injury site, the local lesion of the peroneal neuropathy is preferentially thought to involve the nearby fibular head, because of its anatomic susceptibility to injury [3]. To verify the neural compression by a cast, the patient must be interviewed in detail about where the proximal end of the cast has been exactly and if the cast has been too tight. In this case, the patient related that the proximal end of the cast had been located at the mid-tibial level and not over-tightened. The cast property was confirmed again when collaborating with the patient’s primary physician.
After the lower extremity injury, the physician may also consider traumatic mononeuropathy as a cause of the foot drop. Commonly, the blunt trauma may induce direct neural compromise and indirect impact by hematoma formation or soft tissue swelling. Rarely, peroneal nerve palsy following an ankle sprain is possible, which may result from sudden nerve traction injury [4, 5]. However, the patient in this case could not recollect a direct knee trauma and related that the ankle had not been inverted extremely. No observable skin scar was found around the knee, and there was no definite evidence of soft tissue injury, except for the cystic mass on the MRI and ultrasonography. Furthermore, other associated lesions, such as a peroneus longus muscle rupture or anterior talofibular ligament tear, were not found.
Peroneal neuropathy around the proximal fibula may have two actual anatomic lesion sites: a CPN lesion and more distal deep peroneal nerve. Even if a differential diagnosis of a specific lesion site is less helpful in planning clinical management, detailed etiologic information can aid in the prognosis and progress. An electrophysiologic study can differentiate between two lesion sites; however, a routine test protocol (i.e., extensor digitorum brevis muscle recording and ankle-fibular neck-popliteal fossa stimulating) may misinterpret the recoding data because the actual common peroneal nerve lesion can have less involvement of the proximal fibers of the superficial peroneal nerve. In this case, the superficial peroneal nerve was spared. So, a technique for common peroneal mixed nerve conduction was applied; it confirmed common peroneal neuropathy. This exact lesion site investigation was very important to correlate with the ultrasonographic findings.
On the MRI with a knee extension, a cystic mass was found adjacent to the PTFJ. It may have originated from the PTFJ due to the increased pressure of the knee joint by a traumatic injury [6]. However, the shortest distance between the mass and CPN was as much as 11.5 mm on the axial sections, and the mass did not directly compress the CPN. These findings might indicate that the neuropathy was not directly attributed to the mass. We could not conclude that the MRI demonstrated a mass arising from the PTFJ that extended along the peroneal nerve and directly compressed the peroneal nerve on the static images. Ultrasonographic scanning also did not display any definite abnormal findings with the knee extension in the supine position.
However, the ultrasonographic scanning during knee flexion exhibited a bulging mass on the lateral site along the posterior surface of the fibular head, which was not the site of cystic mass on MRI. The mass was surmised to migrate as the conformational change during a knee flexion of greater than 30 degrees. The tensile forces of the lateral head of the gastrocnemius muscle on the knee extension decreased during flexion because of the shortened muscular length. Therefore, it could displace a proximal portion of the gastrocnemius lateralis muscle and change the structural position.
Compared with the MRI, the ultrasonography had a higher spatial resolution. Furthermore, as a faster and more cost-effective method, it is a very convenient first-line imaging method for the diagnosis of peripheral nerve disorders [7, 8]. Ultrasonography has its strength in specific pathologies that require dynamic imaging for diagnosis, such as specific joint movement or positioning that routine MRI is unable to effectively diagnose. So, dynamic ultrasonographic studies can complement the limitation of the static characteristic of MRIs.
In this case, a dynamic ultrasonography demonstrated the cause of a foot drop by confirming the movable mass during knee flexion that could not be explained by MRI. This example is a rare case of an extraneural mass localized to the PTFJ that did not directly compress the adjacent CPN, but instead acted from a distance during joint motion. It is important to perform dynamic ultrasonographic studies and consider its association with abnormal findings in clinical practice for the diagnosis of peripheral nerve disorders around the motional joints.
Footnotes
Conflict of interest
No conflict of interest was reported by the authors or any individuals responsible for the content of this article. None of the authors have financial or commercial interests in connection with this study.