
Abstract
BACKGROUND:
Shoulder imbalance is a problem for scoliosis patients. Rasterstereography uses radiation-free surface topography to follow up these patients. Its use for assessing shoulder level has not been investigated earlier.
OBJECTIVE:
This study aimed to determine the accuracy of shoulder assessment using rasterstereography (versus radiography) and to analyze its relationship with patients’ self-image.
METHODS:
In a cross-sectional setting, the reliability and validity of five rasterstereographic shoulder variables were measured in comparison with six radiographic shoulder parameters, using correlation analysis. The patients’ self-perception was documented using the Scoliosis Research Society-22 (SRS-22) questionnaire and Trunk Appearance Perception Scale (TAPS).
RESULTS:
Forty patients were included in the study. The test-retest reliability of all rasterstereographic shoulder parameters was excellent (ICC
CONCLUSIONS:
Rasterstereography is a reliable and valid method for assessing shoulder level in idiopathic scoliosis. The parameters can be recommended as a complement to radiography and clinical evaluation for follow-up purposes. Radiographic and rasterstereographic shoulder parameters are significantly related to patients’ self-perception. Shoulder variables thus need to be considered in scoliosis patients.
Keywords
Introduction
In patients with idiopathic scoliosis (IS), shoulder level is known to affect both the patients’ own self-perception and also body appearance ratings by others [1, 2, 3, 4]. It is therefore commonly measured during consultations with IS patients. Standard assessments include clinical and radiographic evaluation of shoulder height [5, 6, 7].
Qiu et al. [8] were the first to describe a divergence between shoulder parameters measured using radiography and clinical photographs, and others confirmed these results [9, 10, 11]. Some authors suspected that the poor concordance between certain clinical and radiological shoulder variables resulted from assessment of two separate areas – the medial and lateral shoulder regions – using distinct parameters [8, 9, 12]. Patient-reported outcomes have also recently been taken into account but the associations between questionnaire data and photographic shoulder levels were weak or not significant [13]. This called into question the usefulness of assessing shoulder parameters on the body surface in general.
Radiation-free surface topography systems have been available for monitoring scoliosis progression for more than 30 years [3, 14]. Rasterstereography, an established example, digitizes the body surface by projecting horizontal light stripes onto a body area and recording a photographic image. It achieves an accuracy of less than a millimeter [15, 16]. Its validity for following up IS patients with Cobb angles of up to 80
This study was conducted to assess the reliability and validity of relevant shoulder parameters in rasterstereography in comparison with radiography. Secondly, this study aimed to investigate the relationship between shoulder balance and patients’ self-perception of their body using patient-reported outcome questionnaires since the relevance of shoulder level for IS patients remained unclear in the recent literature.
Materials and methods
Forty individuals (33 females and seven males) with IS agreed to participate in this cross-sectional study during routine outpatient visits between July 2014 and January 2015. All investigations, including radiography, were indicated and performed exclusively for clinical routine care, completely independent of the study. Patients with clear IS deformities who were undergoing radiography were included. Exclusion criteria were braces worn on the radiograph, spinal deformities other than IS and patients with reasons for shoulder imbalance other than IS. Written informed consent for this publication and any accompanying images was obtained from all patients included in the study or their legal representatives (for patients younger than 18 years).
Rasterstereographic shoulder assessment
Three rasterstereographic examinations per participant were conducted on the day of consultation, using the Formetric system (Diers International, Wiesbaden, Germany). For this purpose, adhesive surface markers were placed above the spinous process of the seventh cervical vertebra and above the palpated acromioclavicular joint lines bilaterally. The patients were positioned facing a wall, with their backs toward the rasterstereography hardware, consisting of a projector and a digital camera. The distance from machine to the patient’s back was 2 meters. The horizontal stripes projected onto the patients’ backs were adjusted to their height, and an automatic series of 12 images was taken using the rasterstereography system, which then calculated an average image to reduce movement artifacts. After two repetitions of this procedure (including marker replacement) to assess the reliability of the measurement technique, three averaged images were available for further analysis. Rasterstereographic images were stored and analyzed using the Formetric software.
A sample image obtained with rasterstereography. The three larger dark points are recognition spots of the adhesive markers mentioned in the text po, outer perpendiculars for measuring the Outer Shoulder Height Difference; pi, inner perpendiculars for measuring the Inner Shoulder Height Difference; ac, line for measuring the Acromion Angle; ax, line for measuring the Axillary Angle; ts, trapezial slopes.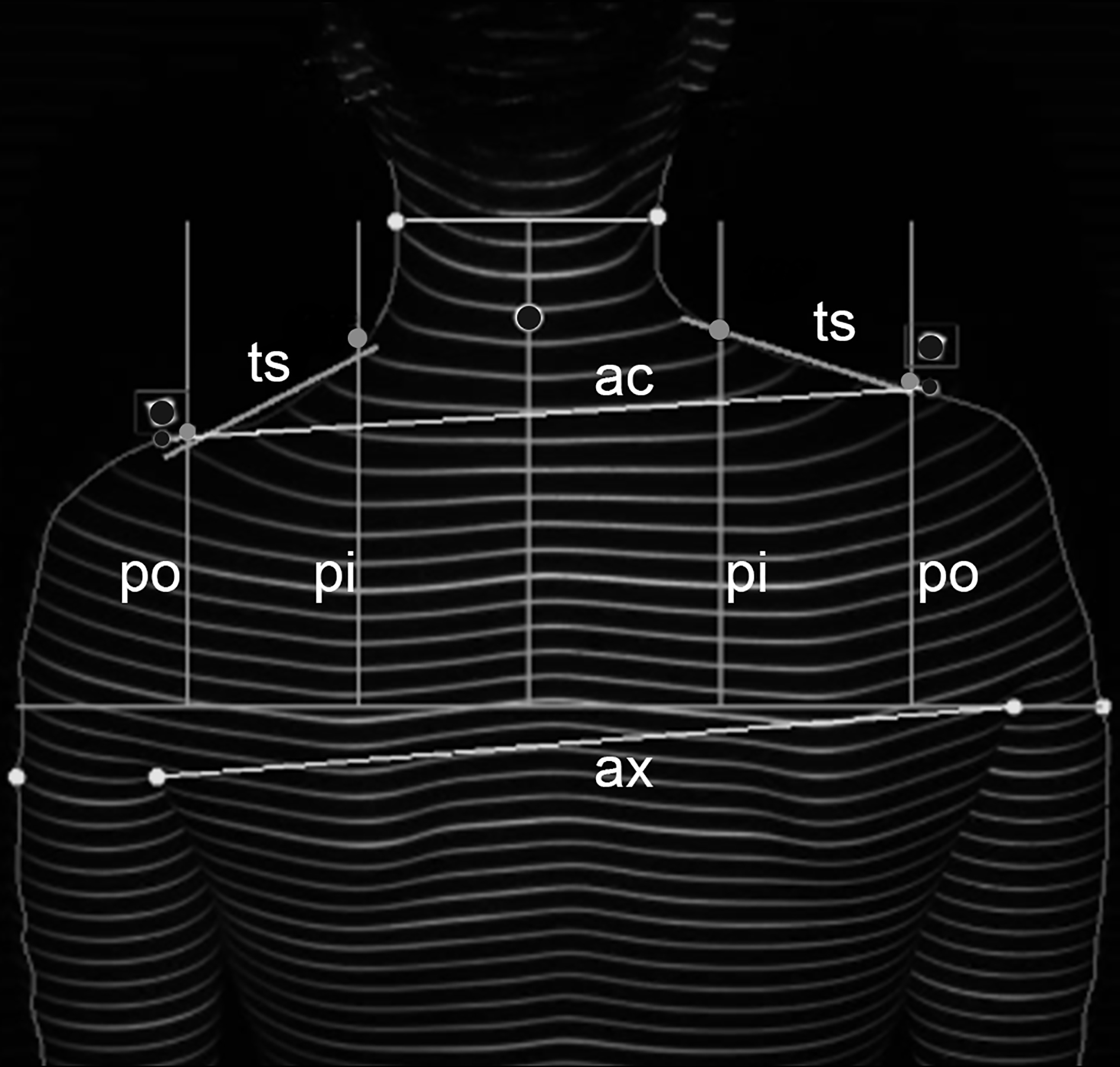
Five variables in each rasterstereographic image (Fig. 1) were automatically captured using a software module developed for this study. These variables are similar to parameters described in earlier studies of clinical photographs by other groups [8, 10]. In all shoulder parameters, elevation of the left shoulder was represented by a positive value and lowering of the left shoulder by a negative value according to the literature [8, 9, 10, 11].
To measure the Outer and Inner Shoulder Height Difference (in millimeters), a perpendicular line was dropped from the C7 marker to a horizontal line drawn through the most cephalad axillary fold. This line was split into thirds on each side of the perpendicular, up to the lateral body margin. Four perpendicular lines were produced in the upward direction at the intersection points. The distances along these perpendiculars between the axillary horizontal line and the upper body margin were measured (Fig. 1: left outer perpendicular line, po; left inner perpendicular line, pi; and right pi and po, respectively). The difference between the left and right po line was named oH (Outer Shoulder Height Difference). The difference between the two pi lines was named iH (Inner Shoulder Height Difference). The Acromion Angle (Ac, in degrees) was measured between a horizontal line through the right adhesive marker and a line between the left and right markers (Fig. 1: ac line). The Axillary Angle (Ax, in degrees) was defined as the angle between a horizontal line through the right axillary fold and a line between the left and right axillary folds (Fig. 1: ax line). Finally, the Trapezius Angle (Tr, in degrees) was defined as the difference between the right and left trapezial slopes (Fig. 1: ts). For this purpose, the trapezial slope was computed using the method of least squares of the shoulder silhouette.
Erect standing anteroposterior whole spine radiographs of all patients were taken for reasons completely independent of the study. The tube–film distance was 3 meters. The radiographs included all relevant anatomic landmarks of the shoulders. The PACS program (GE Medical Systems, 2006) was used for storing and processing the radiographs.
In the radiographs, six established parameters were used to assess shoulder level [5, 7, 8, 19]. Again, positive values represented a higher left shoulder. The Coracoid Height Difference (CoHD, in millimeters; Fig. 2a) was defined as the height difference between the upper margins of the two coracoid processes. The Clavicular Angle (CA, in degrees; Fig. 2a) was measured between a line connecting the most cephalad points of the two clavicles and a horizontal line. The Clavicle Height Difference (ClavHD, in millimeters; Fig. 2b) represented the height difference between the lateral superior edges of the two clavicles, resembling the Ac measurement points in rasterstereography. The Clavicle – Rib Intersection Difference (CRID, in millimeters; Fig. 2b) was the height difference between the superior lateral intersection points of the second rib and the clavicle on each side. The First Rib Angle (FRA; Fig. 2a) was defined as the inclination of a line through the upper edges of the first ribs on both sides towards a horizontal line. The T1 Tilt Angle (T1T, in degrees; Fig. 2b) was measured between the cranial T1 endplate and a horizontal line.
The radiographic shoulder parameters assessed in the study. (a) FRA, First Rib Angle; CA, Clavicular Angle; CoHD, Coracoid Height Difference. (b) T1T, T1 Tilt Angle; ClavHD, Clavicle Height Difference; CRID, Clavicle–Rib Intersection Difference.
The Cobb angles of the proximal thoracic, distal thoracic, and lumbar curves, as well as the patients’ age at consultation and their gender, were also recorded.
All patients were asked to complete two questionnaires, to assess their self-image [20]. The German version of the Scoliosis Research Society-22 questionnaire (SRS-22) [21, 22] includes 22 items with 5-point Likert scales (5
Methodology
The reliability of the rasterstereographic parameters was investigated using intraclass correlation analysis. The validity of the measurements obtained with rasterstereography (using the mean of the values obtained from the three images) was reviewed in comparison with radiography using Pearson correlation coefficients. Linear regression models were built to investigate which rasterstereographic variables had the closest relation to radiographic parameters as the gold standard. The questionnaire data were analyzed using Spearman’s rho. Statistical analyses were carried out with IBM SPSS Statistics for Windows, version 22.0 (IBM Corporation, Armonk, New York, USA) and R, version 3.2.5 (R Development Core Team, Vienna, Austria). The level of statistical significance was
Results
The patients’ mean age was 15.9 years. The average Cobb angles were 16
Descriptive statistics for shoulder level according to rasterstereography and radiography using the absolute shoulder height values
Descriptive statistics for shoulder level according to rasterstereography and radiography using the absolute shoulder height values
oH, Outer Shoulder Height Difference; iH, Inner Shoulder Height Difference; Ac, Acromion Angle; Ax, Axillary Angle; Tr, Trapezius Angle; CoHD, Coracoid Height Difference; CA, Clavicular Angle; ClavHD, Clavicle Height Difference; CRID, Clavicle–Rib Intersection Difference; FRA, First Rib Angle; T1T, T1 Tilt Angle.
With regard to the reliability of the measurement technique, the three values per variable obtained from rasterstereography were compared via intraclass correlation coefficients (ICCs). The standard error of measurement (SEM) was also calculated, using the formula SEM
Reliability measures for rasterstereographic shoulder parameters
Reliability measures for rasterstereographic shoulder parameters
ICC, intraclass correlation coefficient; SEM, standard error of measurement; oH, Outer Shoulder Height Difference; iH, Inner Shoulder Height Difference; Ac, Acromion Angle; Ax, Axillary Angle; Tr, Trapezius Angle.
Significant correlation coefficients of the rasterstereographic parameters with each other ranged from 0.324 (iH and Ac,
Validity of rasterstereographic shoulder assessment
The table displays Pearson correlation coefficients and significance levels of radiographic shoulder parameters (columns) with rasterstereographic variables (rows). Correlation coefficients shown in bold were statistically significant. oH, Outer Shoulder Height Difference; iH, Inner Shoulder Height Difference; Ac, Acromion Angle; Ax, Axillary Angle; Tr, Trapezius Angle; CoHD, Coracoid Height Difference; CA, Clavicular Angle; ClavHD, Clavicle Height Difference; CRID, Clavicle–Rib Intersection Difference; FRA, First Rib Angle; T1T, T1 Tilt Angle.
Scatter plots, showing the correlation between the first measurement (abscissa) and the second/third measurements (ordinate) of the Acromion Angle (a) and Trapezius Angle (b), both obtained from rasterstereography.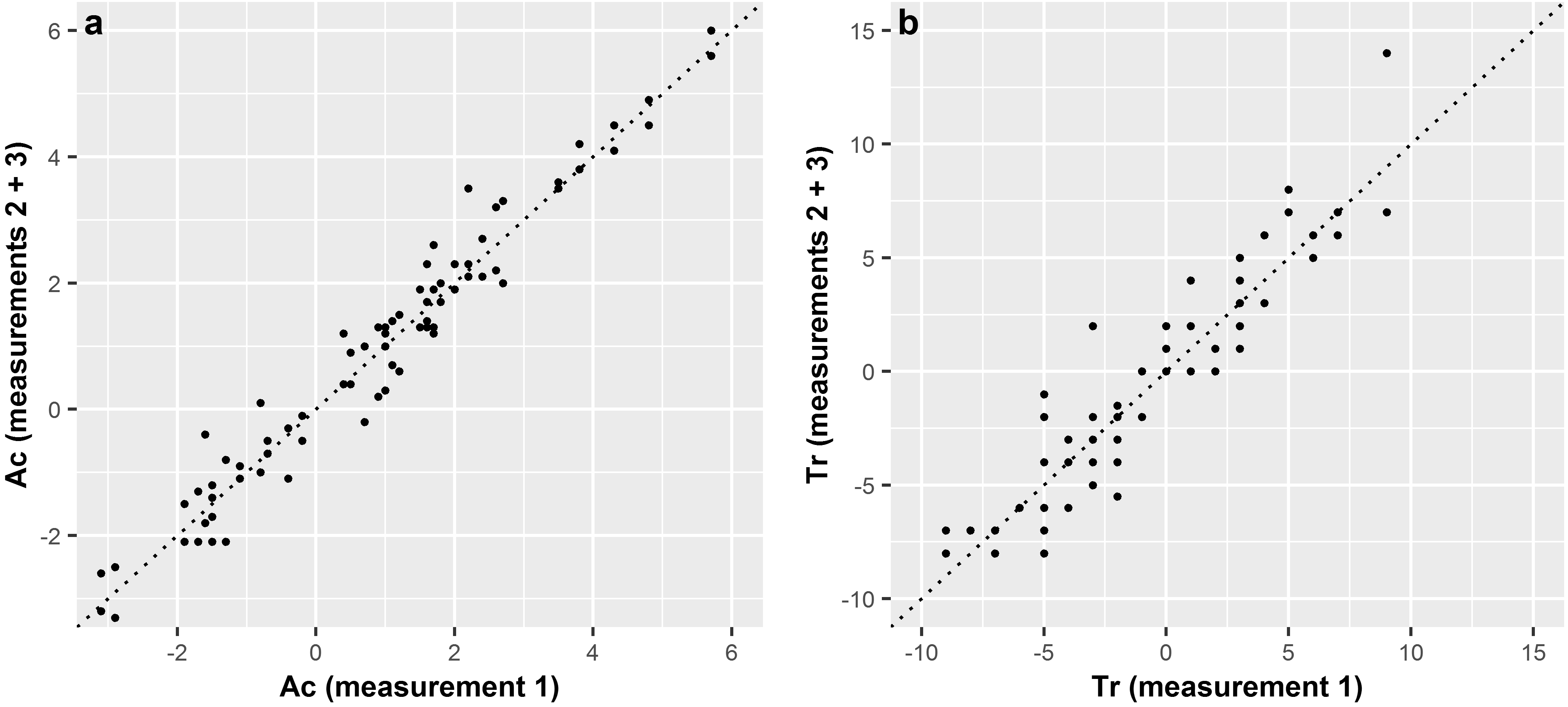
With regard to validity, the correlation coefficients and
Visualization of the two most accurate regression models with 95% confidence intervals: the First Rib Angle, depending on the Outer Shoulder Height Difference (a) and the Clavicle Height Difference, as a function of the Acromion Angle (b).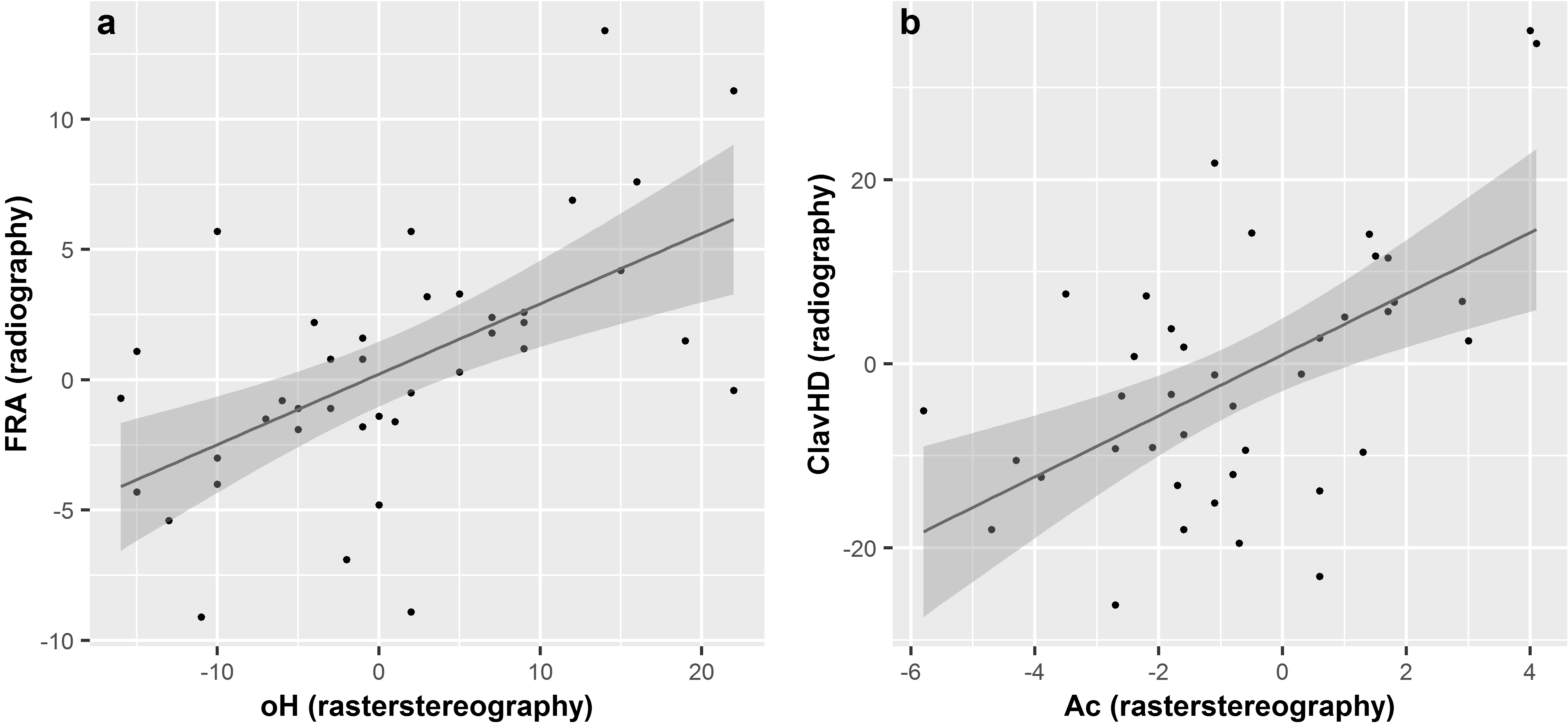
The mean SRS-22 total score was 4.0 out of 5 points (
Shoulder parameters significantly associated with patient-reported outcome questionnaires and the corresponding correlation coefficients (Spearman)
Shoulder parameters significantly associated with patient-reported outcome questionnaires and the corresponding correlation coefficients (Spearman)
In addition to spinal deformity, shoulder imbalance plays a major role for IS patients and their families. Methods available to date for assessing shoulder balance have included clinical examination, radiography, and clinical photography. Rasterstereography is a fast and radiation-free method for following up scoliosis patients, focusing mainly on their spine. Major advantages of the technique lie in the high level of accuracy of body surface detection and automatic, simultaneous measurement of all parameters (including deformity parameters other than shoulder level). No further work is needed after patients have been scanned [15, 18].
Reliability and validity
The present study aimed to evaluate whether rasterstereography is also valid for measuring shoulder parameters, in addition to spinal assessment. It is the largest trial conducted to date that has directly investigated rasterstereographic shoulder balance assessment in comparison with radiography.
The test – retest reliability of the three examinations was assessed using intraclass correlation and standard errors of measurement. The results show that rasterstereography is a reliable method for determining all five proposed parameters. The highest ICC was obtained for the Acromion Angle. The reliability of the method (ICC
The validity of rasterstereographic shoulder parameters was measured by correlating the results with established radiographic parameters [5, 7, 8, 19]. Twenty-five of 30 correlation coefficients proved significant. Most rasterstereographic shoulder variables were thus comparable to radiographic shoulder level. In particular, the rasterstereographic parameter Acromion Angle, defined using measurement points similar to the radiographic parameter Clavicle Height Difference, showed a noticeable correlation coefficient of 0.551 with this radiographic variable. In linear regression, the rasterstereographic variables Acromion Angle and Outer Shoulder Height Difference were most strongly associated with radiographic shoulder height. However, the strongest correlations were only moderate (
Comparison of radiographic and clinical photographic shoulder assessment showed similar correlation coefficients, up to 0.7, in previous studies [8, 9, 10, 11]. Interestingly, Yang et al. [11] reported stronger associations between the parameters on anterior photographs and radiographic variables in comparison with posterior photographs. However, correlation coefficients with the anterior parameters in their study were weaker than the correlation coefficients in the present study using posterior variables.
Bagó et al. [5] investigated the radiographic parameters Coracoid Height Difference and Clavicle–Rib Intersection Difference in comparison with clinical shoulder level examination. The respective correlation coefficients were 0.96 and 0.90. The present study did not reproduce such high coefficients using rasterstereography.
In summary, the rasterstereographic parameters presented here cannot fully replace radiographic shoulder assessment. However, the authors recommend rasterstereography as a complementary technique for routine clinical use, to assess not only curve magnitudes in the spine but also shoulder balance. When IS patients are followed up using rasterstereography, shoulder parameters should thus be considered in the future. However, rasterstereography can be recommended as a tool to complement radiographic measurements but not to replace them.
Patients’ self-perception
Besides evaluating the validity of rasterstereogra-phic shoulder assessment, the present study also aimed to investigate the relationship between shoulder balance and patients’ body self-perception using patient-reported outcome questionnaires (SRS-22 and TAPS). According to Raso et al. [1], 75% of trunk deformity perception is determined by the shoulders, scapulae, and waist. Kuklo et al. [6] found a significant correlation between postoperative clinical shoulder level and patients’ perceptions (
In the present study, four radiographic shoulder parameters had up to moderate, significant correlations with the SRS-22 questionnaire (total score and self-image subscore) and the TAPS (
Assessing shoulder parameters on the body surface consequently reveals a relevant part of the way IS patients perceive their deformity since not only the bone structures are considered. It is therefore obligatory to take radiographic shoulder level and surface shoulder variables into account in IS patients.
Limitations
This study has several limitations. Firstly, the cohort is only of limited size. However, the number of patients included in the present study is similar to that in other studies on the topic [8, 18]. Secondly, the patients only had moderately severe scoliosis curves, with a mean proximal thoracic Cobb angle of 16
Conclusions
Rasterstereography proved to be a reliable method of measuring surface variables at the shoulder in idiopathic scoliosis patients. The rasterstereographic shoulder parameters analyzed in this study correlated significantly with radiographic variables, indicating acceptable validity. Rasterstereography should include shoulder parameters such as Acromion Angle and Outer Shoulder Height Difference as useful complements to clinical examination and radiographic variables in scoliosis patients in the future. Self-perception in patients with idiopathic scoliosis was significantly related to radiographic and surface shoulder variables. Measuring shoulder level is obligatory in patients with idiopathic scoliosis from the physician’s and patient’s perspectives.
Footnotes
Conflict of interest
None to report.