
Abstract
BACKGROUND:
Myofascial pain syndrome is a common form of musculoskeletal disorder that originates from a painful site in a muscle or related fascia. There are various non-invasive and invasive treatment methods.
OBJECTIVE:
To investigate the efficacy of myofascial trigger point kinesiotaping with that of local anesthetic injection alone on the degree of pain and quality of life in myofascial pain syndrome.
METHODS:
Seventy-six patients with myofascial pain syndrome were randomly assigned to three study groups. Group 1 (
RESULTS:
Group 3 showed significantly more improvement than other groups at post-treatment VAS, SF-12 physical component evaluations (
CONCLUSION:
This study indicated that kinesiotaping may be useful to increase the efficacy of myofascial trigger point lidocaine injection in myofascial pain syndrome.
Introduction
Myofascial pain syndrome (MPS) is a common form of musculoskeletal disorder that originates from a painful site in a muscle or related fascia. It has been described as a common cause of musculoskeletal pain with the prevalence from 21 to 85% [1]. It is characterized by myofascial trigger points (MTrP) in muscles, taut bands, referred pain, sensory changes, and local twitch response. An initial injury to muscle fibers may cause trigger points. This injury is sometimes major trauma or repetitive micro-trauma to the muscles. The injured muscle causes pain and stress after that. As the stress on the fibers continues, additional trigger points occur. There are various noninvasive (Spray [freeze] and stretch, transcutaneous electrical stimulation, ultrasound, massage, ischemic compression therapy) and invasive (local anesthetics, corticosteroids and botulinum toxin injections, dry needling) treatment modalities to decrease the pain by inactivating trigger points and loosening taut bands [2]. The local anesthetic injection is known as one of the most common and effective methods in the treatment of MPS [3]. MTrP injections can be painful but using lidocaine may provide immediate anti-nociceptive effect and better treatment results. A study comparing effects of local anesthetic injection with dry needling reported better results with local anesthetic injection [4].
There are three main taping techniques currently used for musculoskeletal conditions: White Athletic Taping, McConnell Taping Technique and Kinesiotaping (KT) method. KT is an alternative taping technique that was developed by Dr. Kenzo Kase and it has been applied in a number of musculoskeletal conditions. Although the full mechanism of KT has yet to be proved, some effects of this technique have been claimed including: enhancement of muscular function, facilitation of lymphatic and vascular circulation and motion due to elevation of skin and subcutaneous tissues, reduction in inflammation and pain, reinforcement of possible articular malalignments [5, 6]. The main mechanism of reduction in pain has been explained to lift of skin away from the tender tissues beneath and to provide space for lymphatic flow by the means of diminishing pressure on tender tissue [7].
Recent studies suggest that KT may be a new treatment option in patients with musculoskeletal problems such as: acute whiplash-associated disorders of the cervical spine [8], subacromial impingement syndrome [9, 10], mechanical neck pain [11], low back pain [12, 13, 14, 15, 16], hamstring muscle flexibility [17], knee osteoarthritis [18], and meralgia paresthetica [19]. According to our knowledge there is one study that investigated the effect of KT method for the relief of MPS [20] and there is a case report of a patient with shoulder pain of myofascial origin who was treated with KT [21]. Although KT is commonly used by clinicians, we consider that there is lack of literature about KT use in MPS treatment. Hence, the present study aimed to investigate the efficacy of MTrP KT with that of local anesthetic injection alone on the degree of pain and quality of life in myofascial pain syndrome.
Method
Design
The present study was a prospective randomized controlled clinical trial with blinded assessment in which only local anesthetic injection, local anesthetic injection
Participants
Seventy-six patients who were admitted to the outpatient clinic with neck and shoulder pain who had at least one painful MTrP located on muscles including trapezius, levator scapula, rhomboids, supraspinatus and infraspinatus due to MPS were recruited in this study (Fig. 1).
Study flow diagram.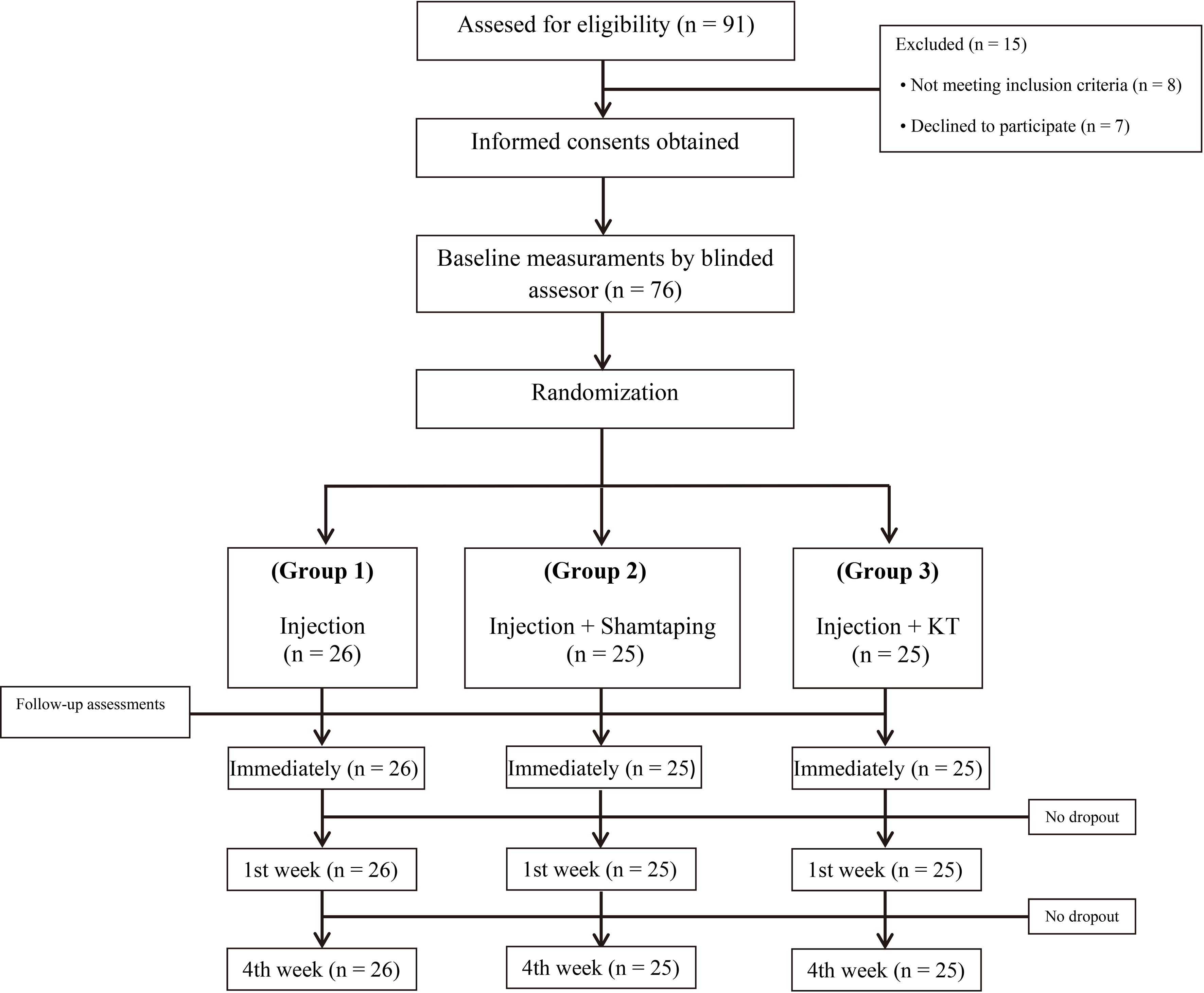
The criteria defined by Simons et al. [22] was used for MPS diagnosis whereby five major and at least one minor criteria are required for clinical diagnosis. Patients 18 to 65 years of age (either sex) were eligible for participation. Pregnant, lactating women and patients with fibromyalgia, mental disorder and a history of lidocaine allergy were excluded.
The patients who met inclusion criteria were assigned to three groups by using randomized numbers obtained from QuickCalcs (©GraphPath software) software. Group 1 received only local anesthetic injection (
Musculus trapezius, m.levator scapula, m.rhom- boideus, m.infraspinatus and m.supraspinatus were the muscles where MTrP were found. Injections and KT applications were done in these muscles.
Trigger point injections were performed as follows: at first, trigger points were determined with palpation and marked by a skin-marker while patients were kept in sitting position and then skin was cleaned with an appropriate antiseptic solution (Fig. 2a).
a. Trigger point that was palpated and marked by a skin-marker. b. Sham kinesiotape was applied in star shape without tension on myofascial trigger point immediately after the injection. c. Kinesiotape was applied in star shape with the space correction technique on myofascial trigger point immediately after the injection.
A 40 mm long 27-gauge needle was inserted perpendicularly through the skin and moved forward until the trigger point that was ensured to be immobilized between thumb and index finger. 1 ml of 0.5% lidocaine solution was injected after negative aspiration into each MTrP and then the needle was withdrawn.
In group 2, four 7 cm
Pain intensity was measured by using a 10-cm visual analog scale (VAS) at baseline, at immediately after the treatment, at 1st week and at 4th week post-treatment [23]. To evaluate the effect of treatment on quality of life, Short Form-12 (SF-12) was used at baseline and at 4th week post treatment. Physical Component Summary (PCS) and the Mental Component Summary (MCS) of SF-12 was calculated. The assessments were conducted by another clinician who was blinded to the patients’ groups.
Statistical analysis
Statistical analysis was done using SPSS version 19.0. (IBM SPSS Statistics 19, SPSS inc., Somers, NY, USA). Data were expressed as mean
Results
Seventy-six patients (25 males and 51 females, 43.09
Baseline characteristics of the patients
Baseline characteristics of the patients
VAS scores and SF-12 parameters at baseline, immediately after injection, at 1st week and at 4th week follow-up of patients
There were significant differences in 1
Post-hoc comparisons for all outcome measures
baseline minus immediately after treatment,
Comparison of VAS and SF-12 changes between the groups showed that VAS and SF-12 PCS scores at post-treatment evaluations in group 3 improved more than groups 1 and 2. No significant difference in SF-12 MCS scores was found between groups 2 and 3, but improvement of group 3 was significantly better than group 1.
In the current study, we tried to investigate the efficacy of MTrP kinesiotaping with that of local anesthetic injection alone on the degree of pain and quality of life in myofascial pain syndrome. We achieved significant improvement in pain, and physical and mental health status with KT application in combination with MTrP injection and KT increased the efficacy of the treatment of MPS.
The most recent systematic reviews on the KT [24, 25, 26] included one randomized controlled study investigating the effect of KT on pain and ROM in patients with acute whiplash injury [8] and another study investigating the effects of shoulder joint stabilization exercises with taping that was applied before stabilization exercises to the upper trapezius muscle on patients with MPS [27].
In the first study, Gonzales et al. reported statistically significant effects of KT compared to sham taping for pain or range of motion (ROM) in individuals with neck pain due to acute whiplash injury; however, improvements in pain and ROM were small and the investigators reported that this improvement may not be clinically significant [8]. Assessment of KT treatment was done after 24 hours in the study of Gonzales et al. [8]. Similarly, in the current study, assessments in immediately after treatment period showed that there is no significant difference in patient groups. But at 1
In the second study, Lee et al. concluded that applying non-elastic taping (twice a week for four weeks) before stabilization exercises is more effective in relieving pain and improving the ability to perform activities of daily living in patients with MAS in the upper trapezius [27]. In the current study, KT was performed by thin and elastic tapes with proper tension. In addition, these tapes have similar physical properties with human skin to allow normal range of motion and aeration. The main difference of KT from traditional tapes is the ability to activate the muscle tissue [28]. Pain relieving mechanisms of KT on musculoskeletal tissues are not clear [29]. It was claimed that KT application may increase intramuscular blood flow may by stimulating the autonomic nervous system and may decrease algogenic substances within muscle [28]. Furthermore, it was also suggested that activating the endogenous analgesic system and inhibiting pain transmission according to the gate control theory by stimulating mechanoreceptors are other hypotheses for pain reduction with KT [30]. When anti-nociception by lidocaine injection and above mentioned effects by KT are taken into account, this may explain how KT increases the efficacy of local anesthetic injection.
In addition to pain assessment with VAS rating, the current study showed superior effects of KT in MPS treatment by SF-12 scale. In 4
Major limitation of the study was the lack of long-term follow-up and small sample size. Additionally, in order to achieve better recovery of MPS, more than one KT application could have been performed.
Conclusion
In conclusion, significant improvement in pain, and physical and mental health status were achieved with KT application in combination with MTrP injection and KT increased the efficacy of the treatment of MPS. In the light of the present study, it can be claimed that KT may be useful to increase the efficacy of myofascial trigger point lidocaine injection in myofascial pain syndrome. Further studies with longer follow-up and larger number of subjects are necessary to investigate the efficacy of KT and to optimize the KT application.
Footnotes
Conflict of interest
None to report.