
Abstract
BACKGROUND:
Shoulder pain is one of the most common problems affecting people older than 60 years. Among the shoulder pathologies, the disorders of the periarticular soft tissue (e.g. rotator cuff) are considered to be the most common; moreover, these disorders are found in approximately 75% of patients with seropositive rheumatoid arthritis. The incidence of structural rotator cuff tendon pathology, including full-thickness rotator cuff tendon tears, increases with age. Recent researchers suggested that non-operative treatment of full-thickness rotator cuff tears could be successful in some patients; furthermore, in rheumatoid arthritis patients, there was a greater possibility of developing surgical complications compared with non-rheumatoid arthritis patients.
MATERIALS AND METHODS:
A case report of a woman, 72 years old, with rheumatoid arthritis, shoulder pain and pseudo-paralytic arm presented with a massive tear of Supraspinatus and Infraspinatus tendon. In accordance with evidence, the case was managed using pain education and exercise therapy for 2.5 months. The shoulder pain, the function and the range of motion improved following a physiotherapy program.
CONCLUSION:
Pain education in combination with exercise therapy was effective for improving pain and function in a full-thickness tear of Supraspinatus and Infraspinatus tendon in a patient also suffering from rheumatoid arthritis.
Keywords
Background
Pathology of the rotator cuff (RC), long head of biceps tendon and subacromial bursa represents the principal causes of pain, disability and symptoms arising from the shoulder complex [1]. Pathology of RC also afflicts patients with rheumatoid arthritis (RA), indeed shoulder involvement is seen in approximately 75% of patients with seropositive RA [2]. In particular, patients with RA often presented RC pathology in the late stage, ranging from 38% to 70% [3]. From prolonged reduced use, shoulder muscle atrophy occurs and painful crepitus could be observed during motion caused by articular degeneration and inflamed soft tissue [3]. Treatment for RC pathology ranges from conservative treatment (including exercise, electrotherapy, manual therapy, injection therapy, taping) to surgery [4], especially in patients with RA [2]. Pain relief and restoration of moderate function in the severely affected RA often require allo-arthroplasty of the shoulder joint. However, replacement surgery of the RA glenohumeral joint (GHJ) is often complicated by bone deficiencies of the glenoid, thinning or rupture of the RC, and internal rotation deformity [3].
Interestingly, in patients not eligible for the surgical repair of RC tears, the failure rate is between 25% and 90% [5], but in patients with repairs failure, satisfaction levels and functional outcome scores are almost indistinguishable from those whose repairs are intact [6]. The results of randomized controlled trials (RCTs) and systematic reviews (SRs) of surgical interventions for RC pathology and shoulder pain suggest exercise as an effective treatment [7], but the paucity of studies concerning the efficacy of conservative treatment in full thickness RC tear limits definitive conclusions.
With the existing evidence, it remains difficult to draw exhaustive evidence-based conclusions for the effectiveness of non-surgical interventions to treat patients with RA and massive RC tear, and studies with high methodological quality are needed. This case report shows a multimodal biopsychosocial approach for pain relief and complete motion restoration in a patient with full-thickness RC tear and RA.
Case presentation
On May 2017, a 72 year-old woman came to our outpatient rehabilitation clinic presenting a disabling left shoulder pain. She (A.C.) was a widowed English teacher, now retired. She complained about a left shoulder pain quite constant during the day, which started 4 months before the clinical examination. The patient felt a sudden sharp terrible pain, burn in her left shoulder while she was cleaning the fridge with the right hand and with the left hand trying to pick up a magnet that had fallen. From that moment, every time she tried to move the arm she felt pain in her shoulder irradiating to the half lateral arm. A few days after she first felt the pain, in January 2017, she went to her general practitioner (GP), who prescribed NSAIDs (nonsteroidal anti-inflammatory drugs). She reported no benefit after one week and a worsening of the symptoms. For this reason, the GP referred the patient to an orthopedic surgeon. The patient, before the orthopedic examination, performed a magnetic resonance imaging (MRI), on the 27
MRI, performed in axial plane with FSEDP/T2 technique, in the sagittal plane with FSET2 technique and in the coronal plane with SET1, GRET2
The patient reported anterolateral pain, dull at night and thus impairing sleep, and a sharp pain when she tried to move the arm actively. Every active movement was reduced and painful, and there was not easing position or strategy capable of decreasing the symptoms. In her past medical history, the patient reported: a colon cancer with two surgical procedures to implant and remove the stoma, high blood pressure, a total hip arthroplasty, an ankle fracture, and an RA diagnosed 23 years ago.
From a psychological perspective she was a woman with a strong personality, active, and with a high cultural level, with a family present in her life who concerned themselves with her problems. Coping strategies were active and positive. Before the shoulder problem, she also used to go out for a walk every day as prescribed by the cardiologist. She expected to heal completely and to live a normal retired life from a physiotherapy program.
The physical therapist (PT) dispensed two scales for the evaluation of pain and function of the arm. The NPRS (Numeric Pain Rating Scale) [8] showed 5 when the arm was at her side and 8 when the patient tried to move at about 40 degrees in flexion and abduction; the DASH (Disabilities of the Arm, Shoulder and Hand) scale [9] showed 84 points.
During the clinical observation, the patient presented on the frontal plane (anterior view) a significant asymmetry of the shoulders. On the left sagittal plane she displayed a dorsal hyperkyphosis with a forward head posture and, on the horizontal plane (posterior view), she showed a left scapula low, abducted and in downward rotation, corresponding to “SICK scapula syndrome” [10] and scoliosis (Fig. 2).
At clinical observation the patient showed in frontal plane anterior view, an important asymmetry of shoulders, on the left sagittal plane a dorsal hyperkyphosis with a forward head posture and on the frontal plane, posterior view, she showed a left scapula low, abducted and in downward rotation, corresponding at “SICK scapula syndrome” and scoliosis.
A passive evaluation was performed to screen for a stiff shoulder. It was carried out because of the long period of time (4 months) in which the woman had not lifted her arm with a full ROM (range of motion). With an inclinometer, the PT measured 165
In active evaluation measured with an inclinometer, a physiotherapist can measure 50
Furthermore, the PT performed some clinical tests (Neer sign, Hawkins-Kennedy test, IRRST (internal rotation resistance strength test), Yocum test, New pain provocation test, O’Brian test) to verify the load and the patient’s load ability (a measure of outcome to be re-evaluated in the future). Actually, the literature confirms that these tests are not able to identify the source of pain, due to the low value of reliability and validity [11, 12, 13, 14]. In fact, all these tests are positive in this category of patients, thus giving no useful information for clinical practice. The MRI also showed that there was complete ruptures of the Infraspinatus and Supraspinatus (the tendons was retracted as far as the glenoid) with a concomitant presence of a labral tear.
The choice of treatment for RA patients is medication, which includes NSAIDs, disease-modifying anti-rheumatic drugs, and recent biological agents, which are continuously being developed. When general symptoms are present, or when the disease activity is high, medical treatment should be considered. RA patients with disabling shoulder pain, not responding to conservative treatment, should also be considered as candidates for surgery [2, 15]. An increasing body of the literature suggests approaching musculoskeletal diseases from a biopsychosocial point of view. Under a psychosocial umbrella, PT should desensitize and, restore the patient’s functional abilities [16]. For desensitizing the system and prior to starting treatment, in this case, the gap between the perceptions of the patient and the health care professionals concerning pain and its treatment should be narrowed [17], so we should start with pain education for explaining pain before loading the system. Pain neuroscience education (PNE) is a cognitive-based educational intervention performed by musculoskeletal therapist that aims to desensitize the CNS (central nervous system) and consequently reduce pain and disability, through a reconceptualization of pain. Furthermore PNE is therapeutic on its own, with level A evidence supporting its use for changing pain beliefs and improving health status [18].
In this case, PT worked following a complete adherence to a biopsychosocial model, beyond a mechanical approach, thus treating the patient and conditioning her behavior, family environment and cognition [17].
The strategy adopted embraced the “Socratic Style” using irony and maieutic: the PT asks the patient about her beliefs, destroying false certainties, creating doubts about it, and building up beliefs in function to an optimization of conservative recovery [19]. The PT should be aware of the impact of their own attitudes and beliefs on the patients’ attitudes and beliefs, which in turn affect patients’ behavior and treatment adherence [17].
A biomedical interpretation of the imaging can increase fear and avoidance behavior in the patient so the PT should explain it as a normal age-related evolution. We decided to condition our patient to improve her adherence to her physiotherapy program and to destroy her fears and false beliefs. A therapist-focused knowledge translation intervention is very important for improving a patient’s adherence in musculoskeletal physiotherapy practice [20] and re-conceptualizing pain is a crucial step before starting treatment [17]. In this way, the clinical reasoning process will result in an individually tailored treatment program that specifically addresses the patient’s characteristics in order to improve treatment adherence and outcome [19].
For managing loads in patients with musculoskeletal pain, the PT should set the local load, possibly modifying symptoms and re-loading globally the shoulder and the whole body. In this regard, no consensus exists concerning non-operative treatment modalities such as indications, methods, and duration [21, 22, 23].
To treat the patient in the case study, the PT started with manual therapy techniques of traction and glides for reducing, in combination or not with exercise, the patient’s pain [23, 24]. To decrease pain in the early period of treatment, general exercise with isometric contraction was adopted [24].
However, heterogeneity of the exercise interventions, coupled with poor reporting of exercise protocols, prevented conclusions being drawn on specific components of the exercise protocols [25]. The optimal load, the speed, the number of repetitions, the frequency, the length of treatment, the pain during treatment, the type and the intensity associated with best outcomes are still unknown [25]. In this case, the authors tried to decrease patient’s pain starting with shoulder nonspecific mobilization and exercises with the scapular focused on isometric contraction. These were given with the aim of strengthening target muscle but also to re-condition the whole shoulder complex without enhancing pain. To start the rehabilitation program, in this case, the PT gave exercises like “inferior glide” (sitting by the side of an immovable object, the patient placed the arm in abduction to 90 degrees with a fist on the solid surface; the patient then applied pressure with the fist in the direction of arm adduction against the surface and instructed to inferiorly depress the scapula), “row low” (the patient stands upright placing her hand on the leading edge of the surface with the palm facing posteriorly; she was then instructed to extend the trunk, pushing the hand forcefully, with the elbow locked in full extension, against the edge while simultaneously retracting and depressing the scapula), “lawn mower” (the patient begins with flexed and rotated trunk towards the contro-lateral side with the hand at the level of the patella and then smoothly rotates and extends the trunk to a vertical orientation while simultaneously retracting the scapula with a forceful contraction as if she was trying to place the elbow into the back pocket) not for the application of selective criteria of muscle activation, but only to start to engage the whole shoulder complex [24]: the brain knows aims, not single muscle activity.
Exercises proposed to the patient are not muscle-specific strategies but a way to gradually expose the whole body to incremental load, to enhance the patient’s mindfulness, capacities and abilities, and training the involved and also the uninvolved arm. The use of different tools represents a character of variability of the therapeutic session in order to enhance patient’s adherence and to improve endurance, coordination and joint position sense.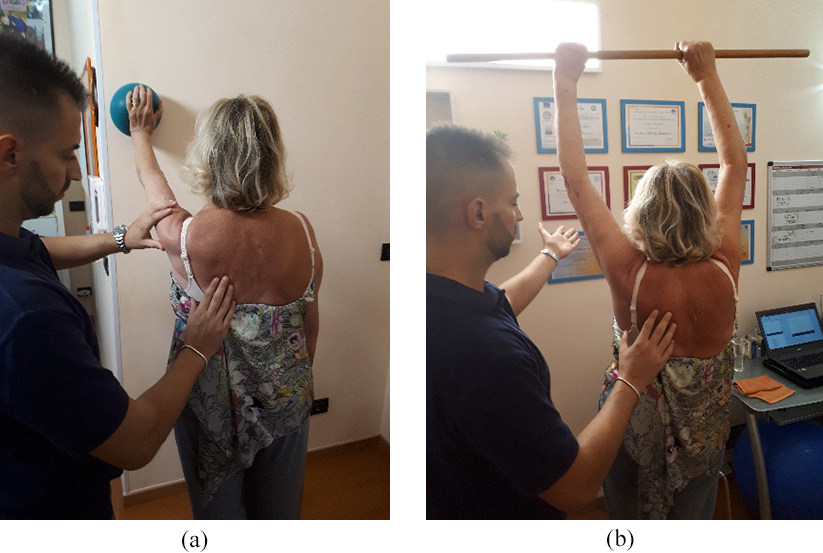
The PT chose an exercise to empower the Teres minor and Deltoid, knowing the limitations of the selective recruitment of muscular components, asking the patient to keep the position of abduction 90
The PT gave exercises to move and enforce “tensegrity” of the scapula and arm, expose the patient gradually to loads, with multiple strategies and modalities to improve variability of therapeutic treatment in order to enhance patient adherence. Variability of strategies can improve endurance, coordination and sense of joint position in people with shoulder pain. Since there was no consensus about optimal characteristics in exercises, we decided to refer to the patient’s daily SIN (severity, irritability and nature) of symptoms to increase or decrease exercise parameters. Exercises were not muscle-specific strategies but a way to gradually expose the whole body to incremental load and to reduce deconditioning of the musculoskeletal system. Furthermore exercises enhance the patient’s mindfulness, capacities and abilities that all together improve his or her self-efficacy [27, 28, 29]. In this way, we proposed an exercise-guided physiotherapy, a training more directed at SNC than at muscles (Fig. 4a and b). More details about exercises and progression are presented in Table 1.
Exercises and timing
Notes: T0
At the end of the 12 week physiotherapy program, the patient presented no pain in the shoulder, 0 points on NPRS [8] and 24 points on DASH scale [9]. She was able to resume her normal ADL (activities of daily life) and she was happy with the result.
Written informed consent was obtained from the patient for the publication of this Case report and all images. A copy of the written consent is available for review by the Editor of this journal.
Authors of this paper know that actually it is almost impossible to understand the exact cause of shoulder pain [30]. Although current evidence clearly emphasizes an incomplete understanding of the nature of pain, the clinicians often uses different theories not well supported by the literature to explain to patients why their shoulder hurts [30]. RC tears with the increase of age, apparently represent, to a certain extent, a “normal” condition in the asymptomatic shoulder population [31, 32], and it is reported in approximately 75% of patients with seropositive (RA). Moving from this perspective, results of MRI were taken into account but we decided to treat the shoulder as a simple painful shoulder in patients with RA. Unfortunately there is limited evidence that conservative treatment, including intra-articular steroid injections, can reverse or considerably influence the destructive process in the RA shoulder, and in rheumatic patients with prolonged symptoms of pain and disability there might be indication for surgery [33]. The authors in this paper think that the tendons had been in that situation for many years (confirmed by retractions in the tendons and fatty infiltration showed by the RMI) and that the episode reported by the patient was not a real trauma. Moreover, because the patient refused the surgical solution, the conservative treatment was agreed upon.
On the other hand, there were also many indications against the conservative option being capable of providing a successful outcome. The most important factor was that MRI. It is a useful tool to rule out Supraspinatus lesion and it is reliable for big RC lesion [34], but it shows the lowest PPV (Positive Predictive Value) for Subscapularis structural status. Furthermore, it often does not recognize the rotator interval pathologies [35]. It is plausible to think that the real situation could have been even worse than the MRI showed because we were sure that the posterior cable was torn but we did not know the real anterior structural status of the endoskeleton [36].
RC lesion in our clinical case had morphological features that could be linked with success through the use of conservative therapy. This data was in accordance with Collin et al. [37] that demonstrated how the outcomes of physiotherapy varied according to the site and length of the tear in patients with irreparable massive RC tear and shoulder pseudo paralysis.
Edwards [21] wrote about a sub-classification of the RC tear suggesting that the best treatment for our patient would be conservative, so we adopted this option.
Furthermore, psychological factors are consistently associated with outcomes. On the other hand, clinical examination findings that are suggestive of a structural diagnosis are not consistently associated with the outcomes of physiotherapy management. This is important when clinicians are assessing and managing shoulder pain [38]. High patient expectations regarding the role of physiotherapy are the strongest predictors of success of conservative treatment as suggested by Cormier et al. [39], Chester et al. [40] and Dunn et al. [29].
Adherence to self-management strategies is capable of providing better results in terms of pain and disability [40]. With the biopsychosocial approach however, we also take into account the non-structural features that studies link with the success or failure of conservative treatment.
Patients with a higher activity level are also more likely to undergo surgery [29, 40]. Our patient satisfied all that features because in her medical history she reported having have high expectations of physiotherapy and that her life was that of a normal retired person.
Because significant gains in contralateral strength and skill have been shown with unilateral exercise, regardless of the kind of exercise (active voluntary, facilitated or imagined) the PT chose to train both the involved and the uninvolved arm, because the presence of interhemispheric connections and ipsilateral corticospinal fibers from the primary motor cortex could provide neural drive to the contralateral muscle during unilateral contraction [41].
Baseline pain self-efficacy was investigated in previous studies: pain self-efficacy was the extent or strength of the patient’s belief in their ability to complete tasks and perform certain behaviours despite pain [29, 40]; our patient showed this characteristic that could positively influence outcomes in patients with shoulder pain.
At the end of the physiotherapy program we performed the “special” orthopedic test on our patient: according with Granviken [26] we found Neer sign, Hawkins-Kennedy, O’Brian and New Pain Provocation Test still positive, even though the NPRS was 0 and ADL were performed without any discomfort.
This study agrees with the results of Ainsworth et al. [42] thus suggesting that PTs could actively manage patients with massive RC tears; the exercise program could produce greater improvement restoring independence and ability in the activities of daily life without surgery.
Conclusion
Treatment of RC tendon disease in patients with RA for pain relief and restoration of moderate function in shoulder disorders unfortunately often requires allo-arthroplasty of the joint. However, replacement surgery of the rheumatoid GHJ could be complicated by bone deficiencies of the glenoid, thinning or rupture of the RC, internal rotation deformity or also in GHJ with Larsen grade III or higher. In addition, due to the thinning or the RC tear, the functional outcome is usually unfavorable in RA patients because function is not sufficiently improved [3]. Furthermore, in this patient, the presence of comorbidity could have increased the rate of failure. Despite these factors conservative treatment was successful in this case because the patient was instructed on the neurophysiology of pain [17, 18, 19]. This approach influenced her behavior, conception, and knowledge and enforced the expectation of a full recovery that is linked with better outcomes. Pain education and exercise also positively influenced pain modulation more than the “therapeutic” effect on the structurally damaged RC muscles and tendons [17, 18, 19]. Furthermore, in this case, the PT also considered that a placebo and “context effect”, muscular compensation for deficient movement strategies and reduction of kinesiophobia as a source of the patient’s improvement [20, 22]. The result of this case study suggests that, rather than surgery, conservative treatment represents the first and probably the best choice for people with massive RC tear and RA.
Footnotes
Acknowledgments
The authors are grateful to Giacomo Rossettini (PT, MSc, PhD) for his precious linguistic advice during the advancement of this manuscript.
Conflict of interest
The authors declare that they have no competing interests.