
Abstract
BACKGROUND:
Kinesiophobia is an important problem that increases neck pain and causes it to become chronic.
OBJECTIVE:
This study aims to compare the relationship between pain, quality of life, and kinesophobia in non-specific chronic neck pain.
METHODS:
In total 87 patients were included in the study. Pain was assessed with Visual Analog Scale (VAS), kinesiophobia with Tampa Kinesiophobia Scale (TKS), and quality of life with Health Status Questionnaire Short Form-36 (SF-36).
RESULTS:
The median age was 50 (40–59) years and the median complaint duration was 12 (8–48) months. The median value of VAS at rest was 4 (2–6) and the median value of VAS during the activity was 7 (5–8). The median TKS scores were 41 (39–45), the median SF-36 general health scores were 61 (45–75), and the median SF-36 mental health scores were 72 (52–80). There was a weak correlation between the TSK scores and gender, education level, and SF-36 general health scores (
CONCLUSION:
TSK scores showed a correlation with gender, education level, and SF-36 general health scores. We conclude that as the education level decreases, kinesophobia scores increase, and as kinesophobia scores increase, the quality of life decreases.
Introduction
Non-specific neck pain is one of the most common spinal problems in the community. Approximately half of individuals experience neck pain over the course of their lives [1]. Although most of them respond well to therapy, the problem may recur or becomes chronic in 1.7 to 11.5% of the general population [2].
Chronic pain is defined as the pain that does not heal at the end of normal recovery period and may result in alterations in both physical and psychological behaviors of the individual [3]. Despite the fact that many factors such as age, gender, poor posture, and repeated injuries play a role in the etiology of neck pain [4, 5], psychological factors such as anxiety and cognitive problems have shown to be also influential [6]. These factors may play a key role in the formation of pain-related fear (kinesiophobia), increased pain or chronicity, and the formation of disability [7, 8, 9]. In addition, several studies have demonstrated that kinesiophobia and fear of avoidance are adverse psychological factors which affect the functioning, treatment process, and recovery [10, 11, 12, 13].
Kinesiophobia or fear associated with pain is a term described by Miler, Kori, and Todd in 1990 as the excessive, unreasonable state of fear which results in reduced physical activity and movement due to the patient’s feeling of anxiety about the pain in the event of an injury and the risk of re-injury [3, 13, 14]. Patients with pain problems often fear that physical activity would worsen their conditions, which leads to avoidance from movement and exercise. However, avoidance from movement or exercise may lead to physical and functional disability, and depression in the long-term. In addition, these psychological factors may play an important role in the chronicity of the disease and pain [7, 9]. Several studies have shown that depression and behavior of pain avoidance are closely related to the chronicity of pain and, consequently, loss of function [15, 16]. Feleus et al. [17] demonstrated a relationship between kinesiophobia, disability, and musculoskeletal system injuries in patients with neck and shoulder pain. In another study, Bahat et al. [18] found a relationship between the severity of pain, avoidance of movement, and disability.
As a result, the presence of kinesophobia can lead to a more severe perception of the pain, an impairment of the quality of life, and ultimately an increase in disability. Therefore, investigation of the presence of kinesiophobia in chronic neck pain and an understanding of the relationship between kinesiophobia and quality of life and pain may be a significant contributor to the arrangement of treatment program and exact treatment of neck problems and the prevention of chronicity of the problem. Therefore, in the present study, we aimed to evaluate the relationship between kinesiophobia, pain, and quality of life in patients with non-specific chronic neck pain, which is frequent in the general population and has many adverse effects. Two two hypotheses that were questioned in our study are as follows:
Participants
Our study was planned as a survey to investigate the incidence of kinesiophobia in patients with neck pain to evaluate its effects on pain, disability, and quality of life. Patients who were admitted to the Physical Therapy and Rehabilitation outpatient clinic and were diagnosed with neck pain were included in study. Inclusion criteria were: 1) having chronic neck pain for at least three months; 2) aged between 18 and 70 years; and 3) having good understanding and communication skills. Exclusion criteria were: 1) having a history of any fracture or surgery; and 2) having an inflammatory disease, and neurological, sensorial, or muscular paralysis.
All participants were informed about the nature of the study and those who met the inclusion criteria were enrolled. A written informed consent was obtained from each participant. The study was approved by the Non-Interventional Clinical Research Ethics Committee (Decision No: 32/22.02.2017) and conducted in accordance with the principles of the Declaration of Helsinki.
Procedure
In this cross-sectional study, 120 patients were screened, of which 93 met the inclusion criteria and were included in the study. However, six patients were excluded as they did not complete the survey. Eighty-seven patients completed the study (Fig. 1). Demographic characteristics such as age, gender, height, weight and body mass index (kg/m
The flowchart of the participants.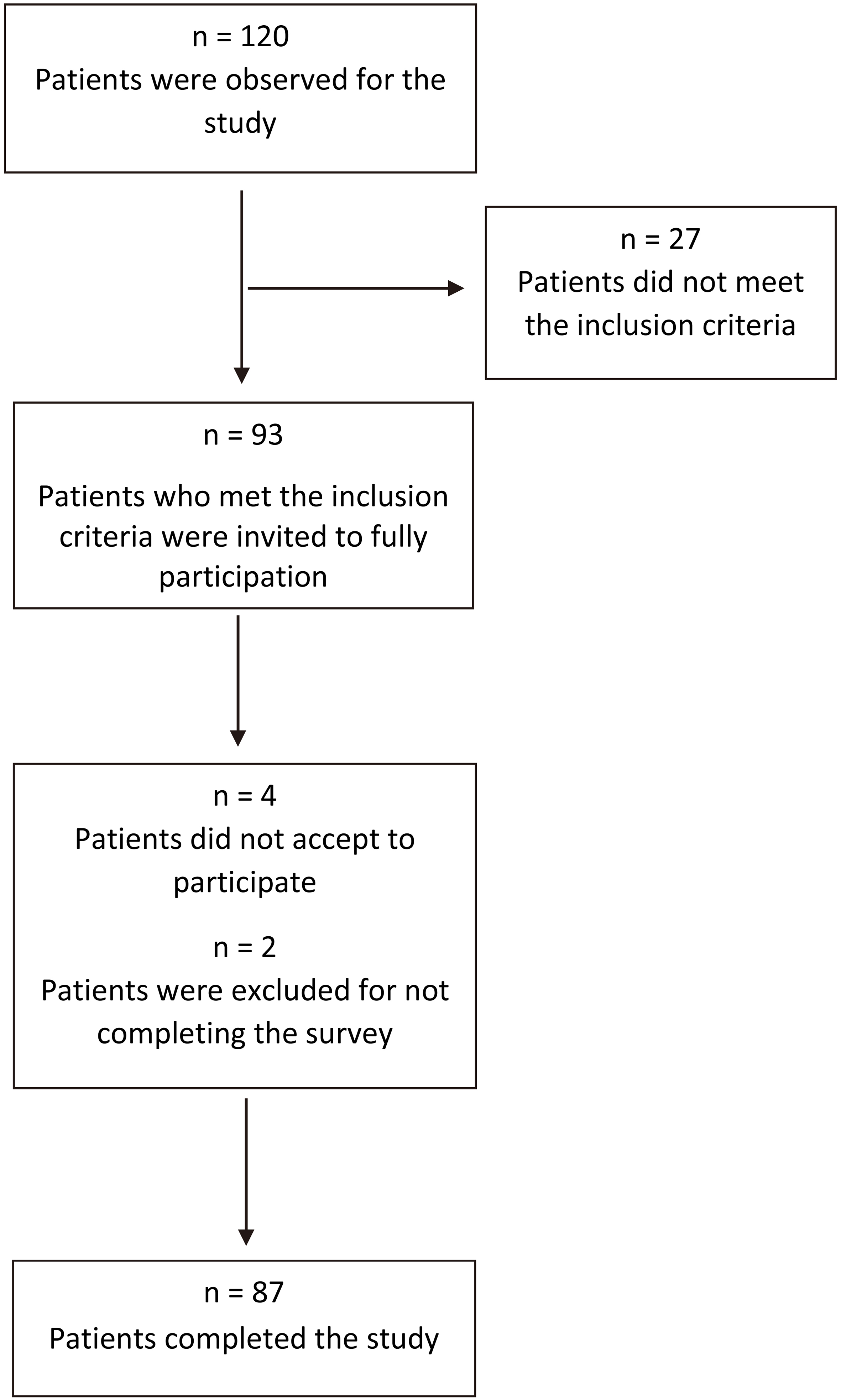
Pain assessment
The VAS is a tool which is widely used to measure the severity of pain. It is a horizontal line, 10 cm in length, and 0 indicates no pain, while 10 indicate intolerable pain. All patients were asked to mark the line indicating the severity of pain in rest and activity they felt, and the results were recorded in cm [18].
Kinesiophobia assessment
The TSK was a questionnaire composed of 17 questions developed by Kori et al. [19, 20] in 1991 for musculoskeletal pain. This scale includes injury/re-injury and fear-avoidance parameters in work-related activities. In this scale, a 4-point Likert score (1
Quality of Life Health Status Assessment (SF-36 Questionnaire)
The SF-36 is a questionnaire which includes 36 items in eight domains: physical functioning, physical, bodily pain, general health, vitality, general mental health, social functioning, and emotional roles. It is used to evaluate the health status of an individual. The reliability and validity of the questionnaire have been reported in many studies and the Turkish reliability and validity study was conducted by Kocyigit et al. [22, 23]. In this scale, high scores indicate a better level of health. The total score ranges between 0 and 100 [24].
Demographic data and characteristics of the cases
Demographic data and characteristics of the cases
IQR: interquartile range. TSK: The Tampa Scale for Kinesiophobia. VAS: Visual Analog Scale. SF36GH: SF-36 General Health. SF36MH: SF-36 Mental Health.
G*Power software v.3.1.9.2 (Heinrich-Heine-Universität Düsseldorf, Düsseldorf, Germany) correlation: point biserial model was used to determine the required sample size for this study. We used a medium effect size (0.3) in power analyses. Eighty-eight participants in group were determined in order to correlations with a power of at least 90% at an alpha level of 0.05.
Statistical analysis was performed using the SPSS version 20.0 software (IBM Corp., Armonk, NY, USA). The variables were analyzed using the visual (histograms, probability plots) and analytical methods (Kolmogorov-Smirnov/Shapiro-Wilks test) to determine whether they were normally distributed. The data were expressed in median and interquartile range (IQR). As the variables were not normally distributed, the Mann-Whitney U and Kruskal-Wallis test were used to compare them according to gender and education level. The relationship between kinesophobia values and quality of life and pain parameters was assessed using the Spearman correlation analysis. The relationship between kinesophobia values and education level and complaint duration was assessed using the Kendall correlation analysis. A p value of
Variable outcomes according to gender and education level
Variable outcomes according to gender and education level
Correlation coefficient results between kinesiophobia and variables
Demographic characteristics, kinesiophobia, and quality of life scores of the participants are shown in Table 1. A total of 87 patients (69 females and 18 males) were included in the study. The median age was 50 (range, 40 to 59) years and the median duration of complaints was 12(range, 8 to 48) months. The median value of VAS at rest was 4 (range, 2 to 6) and the median value of VAS during the activity was 7 (range, 5 to 8). The median TKS scores were 41 (range, 39 to 45), the median SF-36 general health scores were 61 (range, 45 to 75), and the median SF-36 mental health scores were 72 (range, 52 to 80). The patients with neck pain had a higher level of kinesiophobia.
According to the gender, although there was no significant difference in the duration of complaints and pain (
In terms of correlation, TSK scores showed a correlation with gender, education level, and SF-36 general health scores (
Correlation coefficient results between kinesiophobia and the variables
Correlation coefficient results between kinesiophobia and the variables
In the present study, we aimed to evaluate kinesiophobia in the patients with neck pain and to investigate its relationship with demographic data, pain, and quality of life. Based on our study results, we found that the patient with chronic neck pain had kinesiophobia. Kinesiophobia scores in women were significantly higher than men and lower in the college graduates than the others. Furthermore, TSK scores showed a correlation with gender, education level, and SF-36 general health scores. However, there was no relationship between kinesiophobia and the other variables.
Kinesiophobia or, in other words, behavior of fear avoidance can be defined as the avoidance of moving with the idea of pain or re-injury may occur. Although it is well-known that the presence of kinesiophobia is a contributing factor to the increased severity of pain and chronicity of the disease, there is a limited number of studies showing such an association in patients with neck pain. In several studies, the cut-off value of TKS was 37 points, and
The relationship between kinesophobia and other predictors such as demographic characteristics, pain severity, duration of complaints, education level, and quality of life may be helpful for further interpretation and management of the fear and musculoskeletal pain. Several studies in the literature have addressed into these relationships. Feleus et al. [17] evaluated kinesiophobia in patients with non-traumatic arm, neck, and shoulder complaints, and they reported that one of seven variables which were significantly related to the kinesiophobia scores was education level. Similarly, we found a relationship between kinesophobia and education level: as the education level of the patient decreased, kinesiophobia scores increased. High level education might be effective to better understand the importance of movement and exercise in treating the problem and the harmful effects of immobilization. The easy and rapid early realization and recognition according to the education level may reduce the severity of kinesiophobia, increase adaptation of exercise programs and success the rehabilitation process. In addition, good communication between physiotherapists and patients may be also important and education level may affect this type of communication.
Many studies in the literature have previously shown that there is a relationship between kinesiophobia and pain severity, although some of them have not. Cheung et al. [25] reported that there was a weak correlation between the kinesiophobia scores and severity of pain in patients with mechanical neck pain. Vangronsveld et al. [26] also found a relationship between pain severity and kinesiophobia in patients with neck pain secondary to whiplash syndrome. Similarly, Thompson et al. [27] evaluated neck pain after chronic whiplash syndrome and found a relationship between the severity of pain and kinesiophobia scores. On the other hand, Demirbuken et al. [21] showed no relationship between pain and kinesiophobia in patients with neck pain in their study. In our study, consistent with the study of Demirbuken et al. [21], we were unable to find a relationship between the severity of pain and kinesiophobia during both resting and activity. This result suggests that the severity of pain is not effective in the kinesiophobia, more like fear of re-injury may lead to kinesiophobia.
In addition, although previous studies found a relationship between the severity of pain and kinesiophobia in patients with post-traumatic neck pain, there was no correlation between the pain severity and kinesiophobia in patients with chronic neck pain [28]. In our study, the patients suffered from chronic neck pain, and we found no relationship between the pain severity and kinesiophobia. This can be attributed to the fact that pain sensation is not associated with the movement in patients with non-traumatic injuries and that patients are unable to perceive kinesiophobia level similar to pain.
Furthermore, the presence of pain and kinesiophobia may adversely affect the quality of life of an individual. Although there are many studies in the literature evaluating the relationship between kinesiophobia and physical activity, the number of studies evaluating the effects of current kinesiophobia on the quality of life is limited. Altug et al. [29] evaluated pain, physical activity level, kinesiophobia, and quality of life in patients with chronic low back pain and found a higher-degree negative correlation between the subscales of the SF-36 Quality of Life Questionnaire and kinesiophobia. Also, Hansen et al. [30] assessed physical activity, fear of movement, and quality of life in patients with chronic neck pain and reported that as the level of physical activity increased, the quality of life improved and fear of movement decreased. In our study, we found a weakly negative correlation between kinesiophobia scores and general health scores of the SF-36 Quality of Life Questionnaire in the patients with neck pain. In addition, as the kinesiophobia scores increased, the quality of life and general health were negatively affected. This can be explained by the fact that as the level of kinesiophobia increased, the concern of the patients about that the movement and exercise increased the severity of pain or could lead to re-injury arose. We believe that increased kinesiophobia may prevent patients from movement and exercise, resulting in long-term physical disabilities, increased functional disability, thereby, worsening the general health and quality of life.
Nonetheless, this study has some limitations. First, we assessed the patients who were diagnosed with neck pain. However, the patients could not be divided into subgroups according to the cause of pain, such as disk hernia, whiplash injury, spondylitis, or degenerative disc disease. Second, the patients included in this study were in chronic stage. However, as well as chronic stage, acute and sub-acute stages could be also important for kinesiophobia. Therefore, the effects of kinesophobia at different stages should be examined. Third, we also compared kinesiophobia with gender and education level; however, our sample size was small and not homogeneous for an accurate evaluation. As these features may be important in rehabilitation, further, large-scale studies are needed with homogeneous and adequate case numbers. Finally, we did not evaluate functional disability in the study. But the presence of kinesiophobia may be a factor that increases functional disability. For this reason, the evaluation of functional disability in the study could help us to better understand the effect of kinesiophobia.
Conclusion
In conclusion, our study results showed that patients with neck pain had a high score of kinesiophobia, which adversely affected the general health status and quality of life of the patients. High kinesiophobia can cause a decrease in physical activity and avoided exercise. However, this might reduce the effectiveness of treatment and increase the amount of existing disability. Based on our study results, we suggest that, in addition to physiotherapy, multidisciplinary approaches for kinesiophobia may be appropriate to increase the effectiveness of treatment in the management of patients with neck pain.
Footnotes
Conflict of interest
None to report.