
Abstract
BACKGROUND:
Low back pain is an important widespread health problem that can occur at any age, causing serious socioeconomic losses.
OBJECTIVE:
The objective of this study is to investigate the relationship between kinesiophobia severity and pain severity, depression, and quality of life in patients with mechanical low back pain.
METHODS:
The study sample consisted of 155 patients, of whom 72 were female and 83 were male, aged between 18 and 75 years with mechanical low back pain. Quality of life was assessed with the 36-Item Short Form Health Survey (SF-36), pain intensity with the Visual Analogue Scale (VAS), kinesiophobia with the Tampa Kinesiophobia Scale (TKS), and depression with the Beck Depression Inventory (BDI). Patients were divided into the low (TKS
RESULTS:
VAS-pain severity and BDI scores were significantly higher in the high kinesiophobia group than in the low kinesiophobia group (
CONCLUSION:
The results indicated that the severity of kinesiophobia in patients with non-inflammatory low back pain is associated with pain severity, depression, and poor quality of life.
Introduction
Low back pain is an important widespread health problem that can occur at any age, causing serious socioeconomic losses [1]. The lifetime prevalence of low back pain, which is the most common ailment after the common cold, was found to be 59–80% in developed countries and 44–79% in Turkey [2, 3]. Physical factors such as sedentary life, heavy physical load, frequent weight lifting, vibration, and postural stress, as well as low vitamin D levels, can cause low back pain [4]. In vitro, Vitamin D has been shown to stimulate the synthesis of proteoglycans, the most important extracellular matrix component of bone and cartilage. It has been stated that vitamin D deficiency affects the structure and amount of the extracellular matrix of the intervertebral disc by causing structural defects in proteoglycans and contributes to the formation of disc degeneration [5]. Vitamin D also plays an important role in the inflammatory/immune response mechanism of inflammatory diseases. Vitamin D deficiency can exacerbate chronic inflammatory pain through enhanced inflammatory cell infiltration and inflammatory cytokine release [6]. Determining the specific etiology of low back pain can be challenging. Investigating the symptoms and signs pointing to a serious underlying pathology, the ‘red flags’ so to speak, will provide a great convenience for the physician in classifying the low back pain. Most low back pain is of mechanical origin
Considering that kinesiophobia affects rehabilitation strategies, it should be given due attention in the clinical setting in order to prevent the disability of the patient [13]. As a reason, fear of movement due to the possibility of experiencing pain may result in disability, worsening in functional status, and depression in the patient in the long term. In order to establish an effective treatment, medical therapy, physical therapy modalities, and invasive interventions, as well as kinesiophobia affecting physical exercise should not be overlooked and the factors affecting kinesiophobia should be put forward. Understanding the role of pain-related fear and avoidance behaviors can make a significant contribution to the treatment of low back pain and reduce the disability rate, thereby helping patients to return to their daily activities. Therefore, it is crucial to inform clinicians about the presence of kinesiophobia and the factors that increase kinesiophobia.
In light of this information, this study was carried out to determine the level of kinesiophobia in patients with low back pain and evaluate the relationship between kinesiophobia and pain severity, depression, and quality of life (QoL).
Materials and method
Research design
This study was designed as a cross-sectional descriptive study. The study protocol was approved by the Ethics Committee of Mustafa Kemal University (2022–11/2022–23). Informed consent was obtained from all patients prior to the study. The study was carried out in accordance with the principles set forth in the Declaration of Helsinki. Patients were administered the assessment tools under the supervision of a medical doctor in order to obtain objective data.
Population and sample
The population of this cross-sectional descriptive study consisted of the patients diagnosed with MLBP at the Algology Outpatient Clinic of Hatay Training and Research Hospital between January and June 2022. Patients aged between 18 and 75, with normal hip and sacroiliac joint examination findings, less than 30 minutes of morning stiffness in the waist, a diagnosis of MLBP that increases with physical exercise, decreases with rest, and at a level that would not wake them up at night were included in the study. On the other hand, patients who underwent any surgical procedure in the last 6 months, had a history of malignancy or spinal fracture, had an orthopedic or neurological disease that affects ambulation, a cognitive dysfunction, an inflammatory joint disease, and were illiterate were excluded from the study.
Sample size
G*Power (G*Power Ver. 3.1.9.2, Franz Faul, Universität Kiel, Germany) software package was used to determine the effective sample size for the study. With reference to the study conducted by Uçurum et al., based on a mean Tampa Kinesiophobia Scale (TKS) score of 43.14
Data collection
Demographic and clinical characteristics of the pa-tients, including age, gender, height, weight, body mass index (BMI) (kg/m2), and educational level, were recorded. Patients’ CRP (mg/L) and serum vitamin D3 levels measured in the last 3 months were also recorded. Tests were performed on blood samples taken from peripheral venous veins of the forearm. CRP (mg/dL) and 25(OH)D (ng/ml) levels of all patients were recorded. CRP serum levels were measured with a modified latex-enhanced immunoturbidimetric assay using a CRP Latex kit (Olympus Life and Material Science Europe) according to the manufacturer’s instructions. Serum levels of 0–5 mg/L were defined as normal. Vitamin D level was studied with chemiluminescence measurement method in Beckman Coulter Dxl 800 brand and model device. Patients’ kinesiophobia status was assessed with the Turkish version of TKS, pain intensity with the Visual Analogue Scale (VAS), QoL with the 36-Item Short Form Health Survey (SF-36), and psychological condition with Beck Depression Inventory (BDI).
Kinesiophobia
The kinesiophobia status of the patients was assessed with the Turkish version of TKS. The reliability and validity studies of the Turkish version of TKS were completed previously [12]. TKS is a 17-item scale used in assessing acute and chronic low back pain, fibromyalgia and musculoskeletal injuries, and whiplash-related health problems. TKS is a 4-point Likert-type scale. Thus, one can get between 17 and 68 points from the scale [14]. The cut-off value for TKS was determined as 37 in previous studies [15, 16]. Accordingly, patients with a TKS score of
Quality of life
The QoL of the patients was assessed with the Turkish version of SF-36. The reliability and validity studies of the Turkish version of SF-36 were completed previously [17]. SF-36, which consists of 36 items and 8 subscales, is the most commonly used assessment tool in medicine in assessing physical and mental health. The subscales of SF-36 are physical functioning, Role limitations due to Physical Health Problems, Role Limitations due to Emotional Problems, Energy/Fatigue, Emotional Well-Being, Social Functioning, Bodily Pain, and General Health Perceptions.
Psychological condition
The depression status of the patients was assessed with BDI. BDI consists of 21 items that address the characteristic attitudes and symptoms of depression. BDI scores of 10 and above indicate depression [18].
Pain
The pain levels of the patients were evaluated with VAS. VAS is a widely used and validated measurement tool for assessing bodily pains. In assessing pain with VAS, one end of a 100 mm (10 cm) ruler is considered to indicate zero pain level and the other end severe pain level, and patients are asked to show the point corresponding to the pain they feel on this ruler. Higher values indicate more severe pains.
Statistical analysis
The statistical analyses were conducted with the SPSS 23.0 software package (IBM Corp., Armonk, NY, USA). The descriptive statistics obtained from the research data were expressed as numbers (n) and percentage (%) values in the case of categorical variables and as mean
Distribution of patients’ demographic characteristics by low and high kinesiophobia groups
Distribution of patients’ demographic characteristics by low and high kinesiophobia groups
Descriptive data were expressed as
Distribution of patients’ clinical characteristics by low and high kinesiophobia groups
Descriptive data were expressed as
Correlation of TKS scores with other variables
Spearman’s and Pearson’s analyses were used in the correlation analysis. TKS: Tampa Kinesiophobia Scale, BMI: body mass index, CRP: C-reactive protein, VAS: Visual Analogue Scale, BDI: Beck’s Depression Inventory, SF: 36: 36-Item Short Form Health Survey.
The study sample consisted of 155 MLBP patients, 72 female and 83 male, aged between 18 and 75 years. The distribution of the patients’ characteristics by low and high kinesiophobia groups is given in Table 1. Accordingly, 54.2% of the patients had a high (TKS score
Correlation between TKS and SF36-General health perceptions.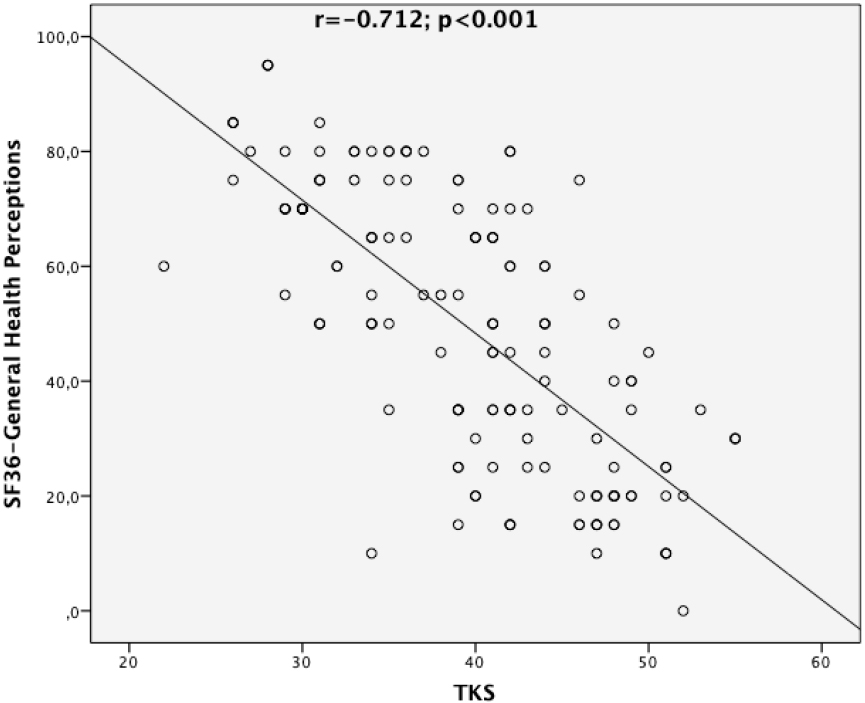
Correlation between TKS and SF36-body pain.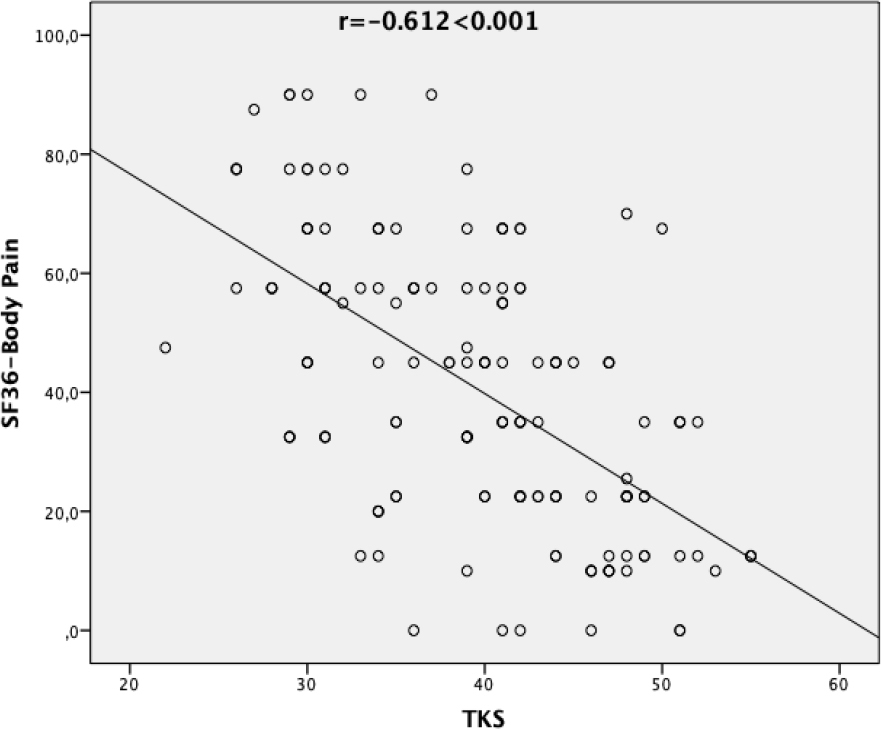
Correlation between TKS and SF36-Social functioning.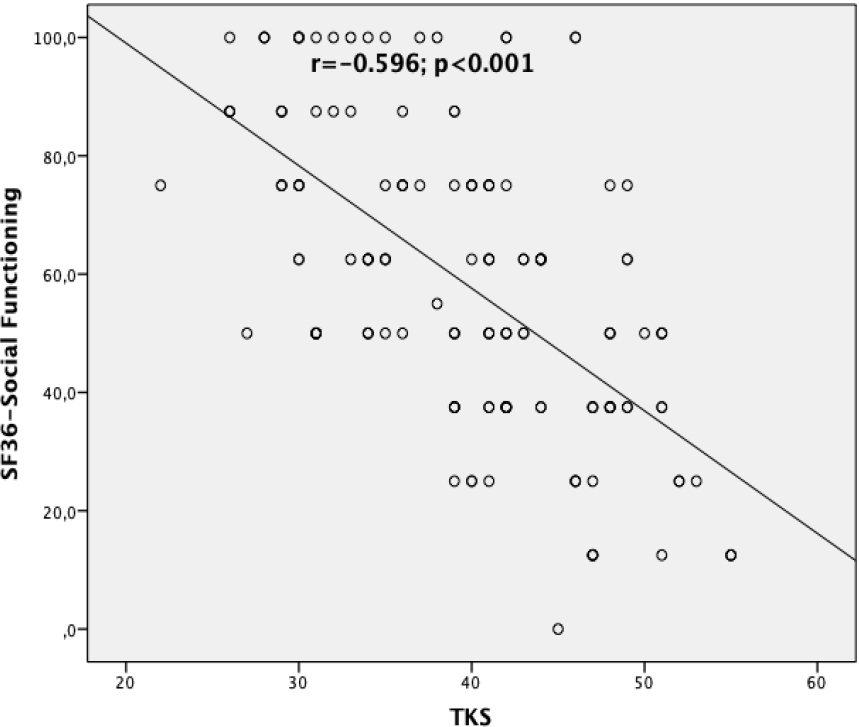
Correlation between TKS and SF36-Emotional well-being.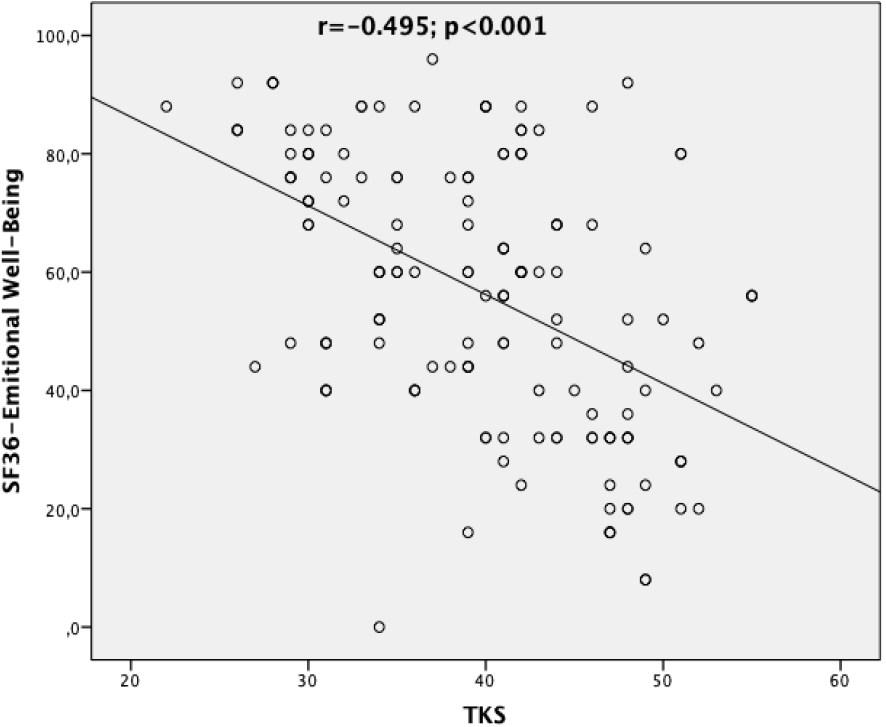
Correlation between TKS and SF36-Energy/Fatigue.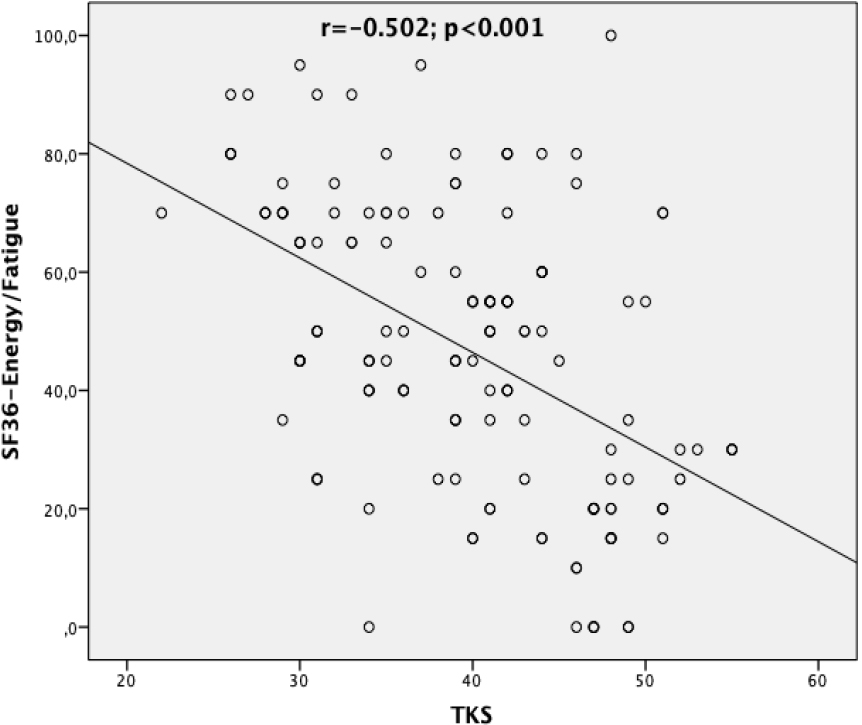
Correlation between TKS and SF36-Role limitations due to emotional problems.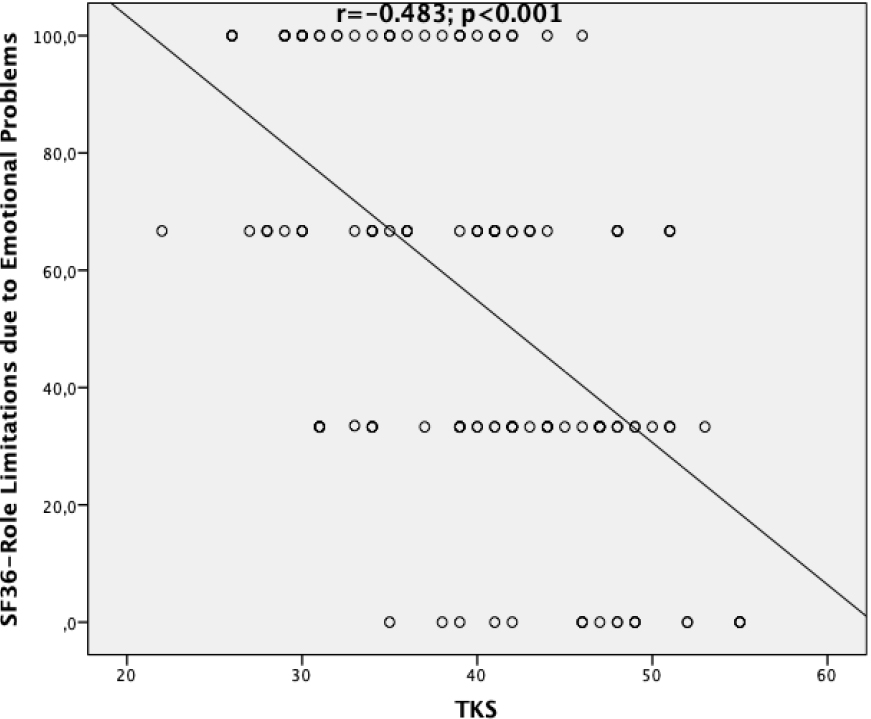
Correlation between TKS and SF36-Role limitations due to physical health problems.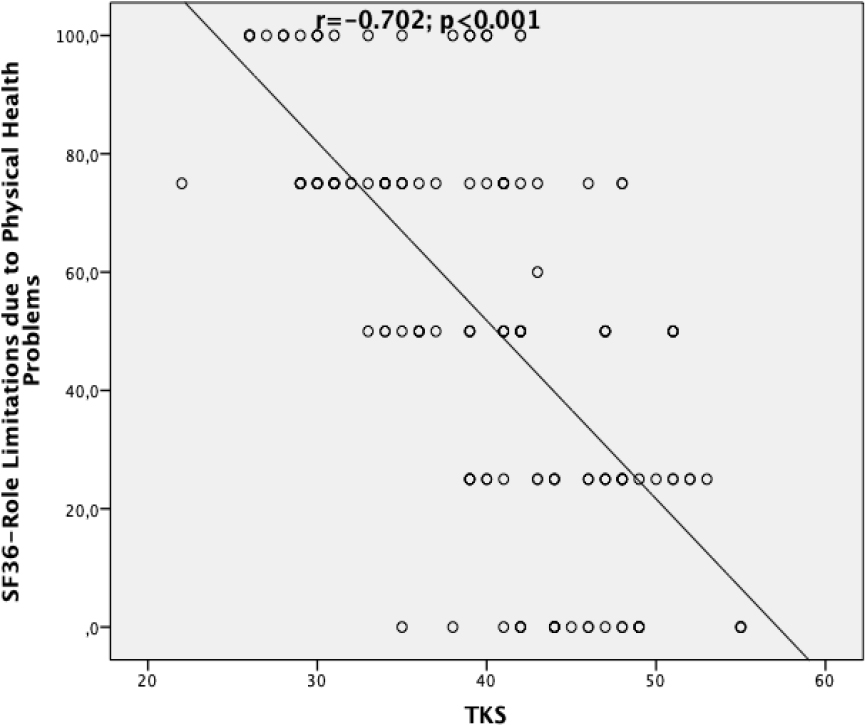
Correlation between TKS and SF36-physical functioning.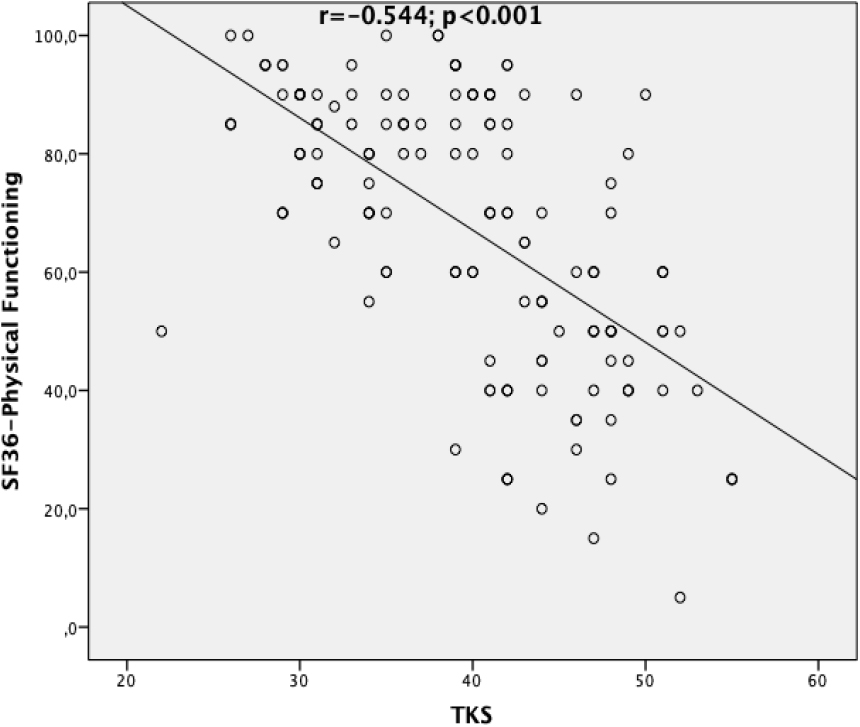
Correlation between TKS and Beck’s depression inventory.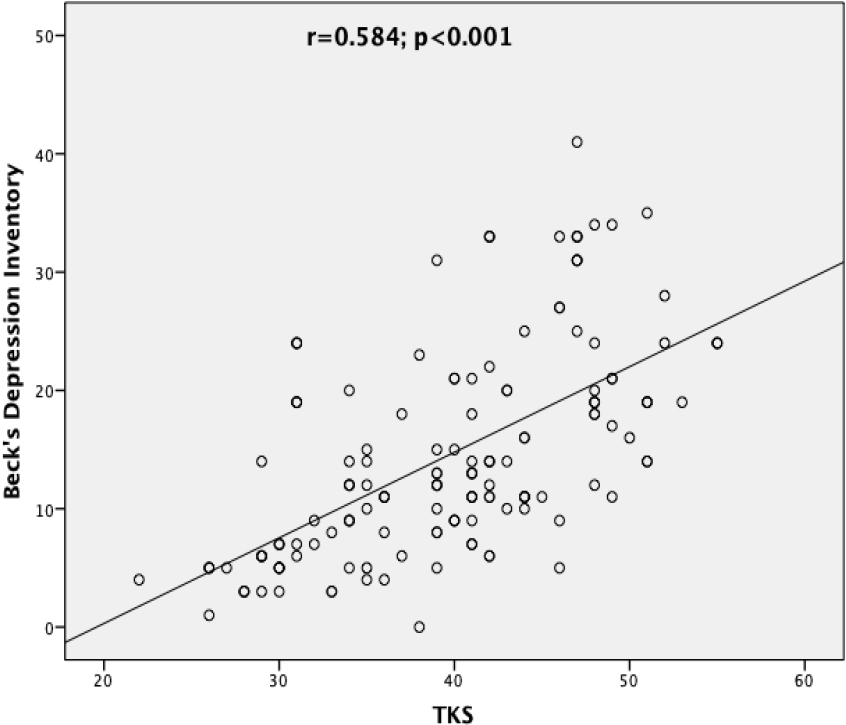
Correlation between TKS and visual analogue scale.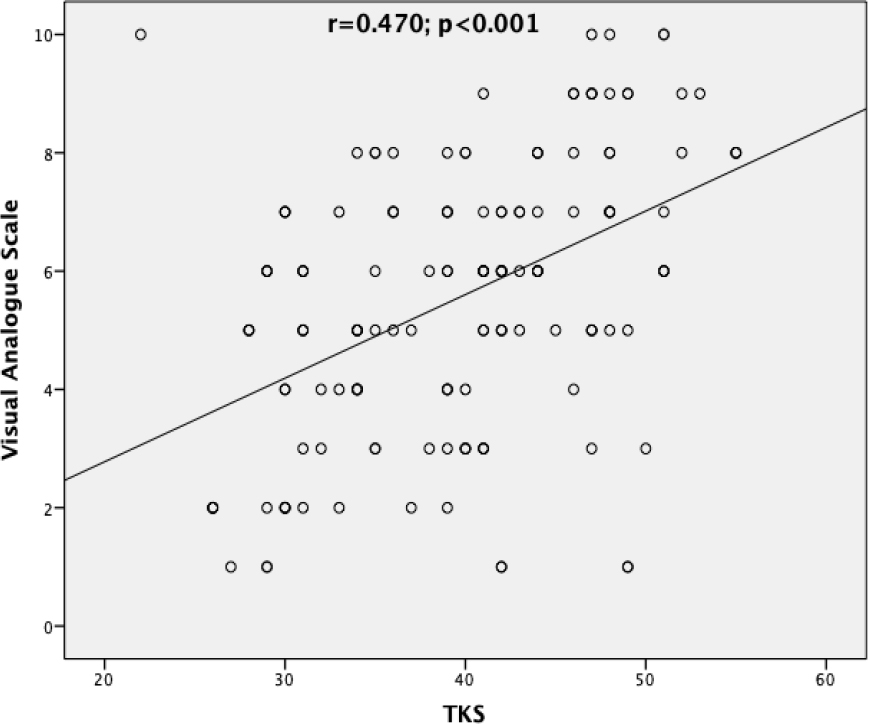
Understanding the role of pain-related kinesiophobia may contribute significantly to the treatment of low back pain. It is important to inform clinicians about the presence of kinesiophobia and the factors that increase kinesiophobia. In this context, this study was carried out to evaluate kinesiophobia and determine the relationship between kinesiophobia severity and pain severity, depression, and QoL in patients with MLBP. Consequentially, the study’s findings revealed a positive correlation between kinesiophobia and pain severity and depression, and a negative correlation between kinesiophobia and QoL. In other words, the QoL levels of patients with high kinesiophobia levels were significantly lower, whereas their pain severity and depression levels were significantly higher than those with low kinesiophobia levels. On the other hand, there was no significant relationship between kinesiophobia and age, educational status, BMI, Vitamin D, and CRP levels.
The results of the relevant studies in the literature are contradictory. For instance, while a study found a significant relationship between educational status and kinesiophobia [19], another study [20], as in this study, did not find any relationship between educational status and kinesiophobia. Similarly, while a study found a weak significant relationship between BMI and kinesiophobia [21], another study [22], as in this study, did not find any relationship between BMI and kinesiophobia. However, further prospective studies are needed to elucidate the relationship between kinesiophobia and BMI in patients with low back pain.
In a meta-analysis, vitamin D deficiency was reported to be associated with low back pain. However, it has been stated that the relationship between vitamin D levels and pain severity is controversial [6]. In the current study, although the VAS score was high in the group with high motion phobia, no statistically significant difference was found in terms of vitamin D levels in the comparison between the groups.
A thorough literature review did not reveal any study on the relationship between vitamin D concentrations and kinesiophobia in patients with low back pain. The only study available in the literature on the relationship between vitamin D concentrations and kinesiophobia was conducted with fibromyalgia patients [23]. In the said study, contrary to this study, a significant relationship was found between low vitamin D concentrations and kinesiophobia. Large-scale studies may further elucidate the relationship between vitamin D concentrations and kinesiophobia.
QoLis a multidimensional concept that includes the physical, psychological, and social aspects of health and is often considered an important outcome of healthcare services. Health-related QoL, on the other hand, contributes to the assessment of the health status of an individual and the development of individual treatment plans, primarily through health screenings, disease burden, and epidemiological studies [24].
There are many benefits of assessing health-related QoL in patients with low back pain. QoL data help clinicians assess the care needs of patients with low back pain, establish treatment goals and plan treatments for these patients. In addition, QoL data provide potentially useful information for monitoring patients with low back pain outside working hours and evaluating treatment outcomes. Studies have reported that chronic low back pain patients have worse health-related QoL, especially in physical components of QoL, compared to healthy individuals. Pain severity as well as poor clinical and functional status associated with low back pain negatively affect the physical components of the QoL [25, 26, 27]. The studies on the relationship between kinesiophobia and QoL parameters in patients with chronic low back pain reported that the presence of kinesiophobia was negatively correlated with QoL parameters of general health perceptions, physical functioning, social functioning, bodily pain, and role limitations due to physical health problems [28, 29, 30, 31]. In contrast, a study conducted with 94 patients did not find any significant relationship between kinesiophobia and QoL parameters, even though kinesiophobia values were higher in patients with low back pain [32]. In comparison, the assessment of the health-related QoL of the MLBP patients included in this study with the SF-36 questionnaire revealed that the scores obtained from all eight subscales of SF-36 were significantly lower in the high kinesiophobia group compared to the low kinesiophobia group. Based on these data, high kinesiophobia can be said to adversely affect QoL. On the other hand, no significant relationship was found between low and high-risk kinesiophobia groups in terms of pre- and post-treatment QoL parameters, i.e., Numeric Pain Scale scores, Modified Low Back Outcome scores, and occupational status (employed or unemployed), in patients with low back pain who were included in a rehabilitation program [33]. In the current study, Numeric Pain Scale, Modified Low Back Outcome Score and occupational status were used as QoL. Instead, the SF-36 QoL scale used in our study evaluates general health, emotional state, and social activities as well as physical functions. Assessing the psychological risk factors and especially kinesiophobia in patients with chronic pain helps determine treatment outcomes, and also contributes to the adoption of a positive approach by the medical staff to the patients and the planning of relevant physical therapies and exercises [34]. Therefore, the discrepancy between the aforementioned study and this study might be attributed to the fact that patients’ emotional and mental statuses were not evaluated within the scope of the assessment of QoL and that no individualized multidisciplinary treatments were administered in the said study.
Depressed individuals with chronic low back pain reportedly fear movement, physical activity, and exercise, rendering themselves more sensitive to pain and re-injury [35, 36]. Studies have reported higher pain, depression, and disability scores in those with high levels of kinesiophobia [16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31, 32, 33, 34, 35, 36, 37]. In comparison, in this study, patients in the high kinesiophobia group had significantly higher pain and depression scores than those in the low kinesiophobia group. In parallel, a significant correlation was found between the TKS and BDI scores in the positive direction. These findings indicate the need for early diagnosis and treatment of psychological disorders such as fear of movement and depression in patients with chronic low back pain, considering that such psychological disorders predict worse prognosis. It has been reported that fear of movement is significantly related to pain in the context of chronic low back [38, 39, 40]. Accordingly, both pain severity and pain-related fear are among the primary factors negatively affecting routine daily and social activities. Chronic pain causes fear of movement and avoidance of movement causes pain, creating a vicious cycle. In line with the findings reported in the literature, the findings of this study support the hypothesis that pain causes fear of movement and fear of movement causes pain, creating a vicious circle.
The strengths of this study are that it addressed the relationship between kinesiophobia and QoL, functional status and psychological state between low and high kinesiophobia groups in patients with MLBP and that it is the first study to examine the relationship between kinesiophobia and Vitamin D levels in this patient group. In addition, patients were administered the assessment tools under the supervision of a medical doctor in order to obtain objective data.
Limitations of the study
Apart from the strengths mentioned above, there were also some limitations to the study. First, the sample size was relatively small. Increasing the sample size could help minimize the margin of error. Secondly, low back pain could have been classified as acute, subacute, and chronic according to the durations that the patients have been suffering from low back pain. Such a classification could allow assessing the pain, kinesiophobia, and QoL separately in each stage, and thereby guide physiotherapists in terms of treatment management.
Conclusion
The study findings revealed that kinesiophobia was negatively correlated with all QoL subscale scores and positively correlated with depression and pain scores in patients with MLBP. Understanding the role of pain-related fear of movement and avoidance behaviors in the development of chronic low back pain and functional disability is key to planning the right treatment modality for the treatment of low back pain and reducing the rate of related disabilities. Kinesiophobia is one of the most significant factors that reduce exercise compliance in individuals with low back pain. Therefore, early detection of kinesiophobia is crucial in order to increase exercise compliance and prevent chronic pain. Clinicians and therapists should keep in mind the fear of movement in patients with low back pain and take the necessary measures to prevent complications that may arise from inactivity. It is important to adopt a multidisciplinary approach toward these patients and assess them also psychiatrically to increase the efficacy of the treatment modalities used in the treatment of kinesiophobia.
Ethics statement
The study protocol was approved by the ethics reviewing committee guidelines of Mustafa Kemal University, Hatay, Turkey (2022–11/2022–23).
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Informed consent
Written informed consent was obtained from each subject.
Footnotes
Acknowledgments
Not applicable.
Conflict of interest
The authors have no conflicts of interest to declare.