
Abstract
BACKGROUND:
Rehabilitation after anterior cruciate ligament (ACL) reconstruction focuses on restoring knee deficiencies and function. However, the extent of the clinician’s direct supervision that is required to recover knee function is unknown.
OBJECTIVE:
To investigate differences in isokinetic knee strength improvement, endurance, and proprioception between home-based (HBR) and supervised rehabilitation (SR).
METHODS:
Thirty participants were randomly allocated to each group after reconstruction. Isokinetic knee strength and proprioception were measured using the Biodex multi-joint and stability systems, respectively, before and after intervention.
RESULTS:
The SR group showed a significant improvement from baseline, but not the HBR group (SR group, from 1.94
CONCLUSIONS:
HBR recovered knee strength as effectively as the SR, but SR was more effective than HBR for the recovery of proprioception and functional knee movement. This result indicates that guidance from health professionals play an important role in enhancing proprioception for patients following ACL reconstruction.
Keywords
Introduction
The anterior cruciate ligament (ACL) is a ligament in the knee joint that is easily injured [1, 2], which leads to various musculoskeletal problems. ACL injury commonly leads to functional impairment and knee instability [3, 4]. The main problems after ACL injury are knee muscle strength deficits or weakness, joint instability, and proprioception deficits [5, 6, 7, 8, 9, 10, 11, 12].
After ACL reconstruction surgery, rehabilitation is important to return to the same levels of sport activities or activities of daily living as those before ACL injury. The goals of rehabilitation for patients after ACL reconstruction are to improve any knee deficiencies and to restore function [13]. Yabroudi and Irrgang [14] reported that rehabilitation after ACL reconstruction surgery is important to enable a safe and full recovery to previous levels of functional activities and sports participation. Van Grinsven et al. [15] reported that the most important aims of rehabilitation after ACL reconstruction surgery are regaining range of motion (ROM), and recovering knee strength and neuromuscular function.
Previous research investigated various different concepts of rehabilitation programs such as accelerated, non-accelerated, and those with special guidelines for ACL reconstruction [16, 19]. However, how much direct or indirect supervision of the therapist is required to achieve successful outcomes is unknown [20]. Several previous studies demonstrated no significant differences in outcomes such as knee ROM, strength, laxity, and functional scores between home-based rehabilitation (HBR) and supervised rehabilitation (SR) after ACL reconstruction [20, 21, 22]. However, to the best of our knowledge, no research has directly investigated improvements in proprioception and simultaneously compared differences in isokinetic knee strength and proprioception, especially postural stability, between HBR and SR in patients with ACL reconstruction.
After ACL reconstruction surgery, patients need to be educated about the full rehabilitation process to restore knee function. However, the extent of the physical therapist’s direct supervision that is required for the patient to successfully recover knee function, including muscle strength and proprioception, is unknown. Therefore, the main purpose of this study was to investigate differences in improvements in isokinetic knee strength, endurance, and proprioception between patients participating in an HBR or in an SR exercise program. We hypothesized that no marked difference exists between HBR and SR exercises after ACL reconstruction in terms of improving knee function as measured by regained isokinetic knee strength and proprioception.
Methods
Participants
The patients were selected using the following criteria: primary unilateral ACL reconstruction surgery to treat isolated ACL rupture; age between 16 and 45 yr; injury at least 12 weeks before with no swelling; and full knee ROM. ACL reconstruction in all the patients followed the same protocol, which uses hamstring tendon autograft surgery. The exclusion criteria were previous reconstruction on any knee ligament before the current ACL reconstruction surgery, combined meniscus and knee ligament injuries, osteoarthritis or rheumatoid arthritis, complications during surgery, and professional athletes.
Thirty patients, consisting of 19 men and 11 women who met the inclusion criteria, participated in this study. Then, the participants were randomly allocated to the HBR or SR group by using an online randomization tool (
Demographics at baseline in the home-based rehabilitation (HBR) and supervised rehabilitation (SR) groups (mean
standard deviation)
Demographics at baseline in the home-based rehabilitation (HBR) and supervised rehabilitation (SR) groups (mean
The difference between each group is shown according to the results of the Student
Flowchart of the study.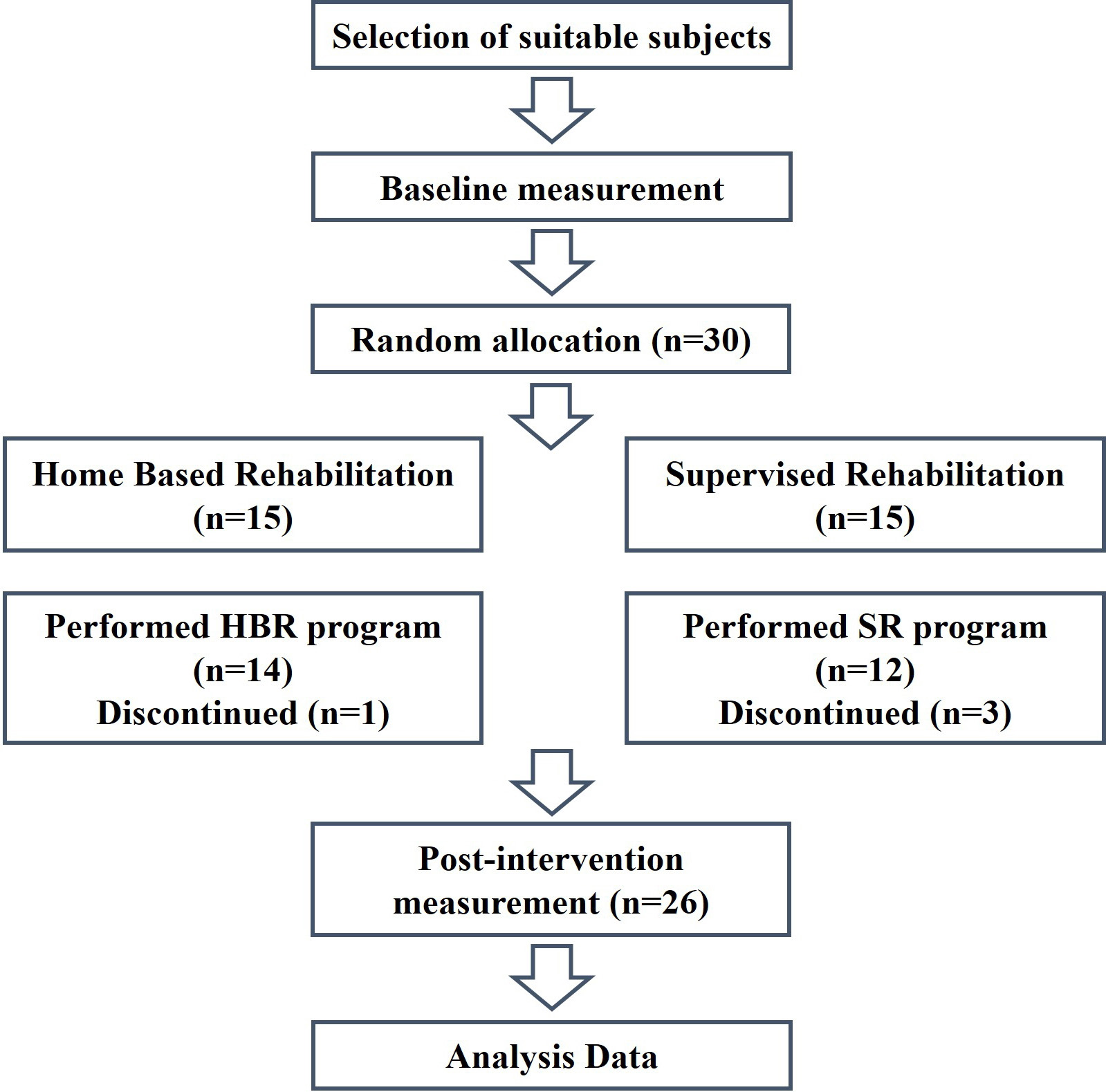
In the 2 weeks preceding the study, all the patients participated in a preconditioning program. In this period, all the patients were educated about the basic exercise program, which consisted of a quadriceps setting (Q-setting) with coactivation, hamstring stretching in a long-sitting position, and full knee extension. During the Q-setting exercise, we asked the patients to keep their heels in contact with the ground.
Components of exercise program
Components of exercise program
SLR, straight leg raise.
After a 2-week preconditioning period, all the patients visited the rehabilitation center. The same rehabilitation protocol based on a previous study was used [19]. In this study, the rehabilitation protocol consisted of phases 1 to 4 for 22 weeks, including knee muscle strengthening, knee stretching, ROM, and one-legged balance exercise. Including the preconditioning period, the total duration of the rehabilitation program was 6 months. All the patients gradually performed the rehabilitation protocol from phases 1 to 4. The specific components of exercise program are presented in Table 2.
Phase 1 consisted of Q-setting during knee full extension, mini wall squat with 60
Phase 2 consisted of a stationary cycle to warm up for 15 min, followed by SLR with elastic bands, squat until 60
Phase 3 consisted of a stationary cycle to warm up for 15 min, followed by squat to 60
Phase 4 consisted of a stationary cycling to warm up for 15 min, followed by squats to 90
After receiving education on the rehabilitation protocol, the patients in the HBR group received elastic bands and a balance board. The HBR group received printed matter containing all details of the rehabilitation program after receiving instruction on how to perform the exercises. We recommend that patients perform the exercise twice per week. A physical therapist with 10 years of clinical experience in sports rehabilitation confirmed the progress of the patients in the program and other remarkable information (band looseness, pain, symptom, complaint, etc.) every week by phone.
SR group
The subjects in the SR group received printed matter containing rehabilitation programs and were fully educated with pictures on the first visit. The rehabilitation exercises were performed under the supervision of the same physical therapist, twice per week. Moreover, SR group were conducted as individual sessions under the supervision of a physical therapist and did not involve any home exercise program during the entire intervention period.
Isokinetic knee strength evaluation.
Our study involved the use of the Biodex multi-joint system 4 (Biodex System 4, Biodex Medical Systems Inc, Shirley, New York, USA) for isokinetic knee strength evaluation (Fig. 2). The patients sat on a dynamometer chair in an upright sitting position, with 90
Postural stability evaluation.
We used the Biodex Stability System SD (BSS; Biodex Medical Systems Inc., Shirley, New York, USA) for proprioception tests (Fig. 3). The patients were positioned without shoes and socks on the BSS platform and stood on one foot, with the weight-bearing knee in a semi-flexed position at 20
Once the participants were in the correct position, the examiner immediately recorded the location of the lateral malleolus and Achilles tendon. Once the participants were positioned, they were instructed to fix their foot until the end of each test.
If the participants lost their balance during the test, they were allowed to briefly toe touch with the opposite foot or grasp the handrails for a short time to reestablish balance as soon as possible. If they were unable to quickly reestablish their balance, the test was deleted.
The platform of the BSS on which the participants stood can tilt 20
Evaluation of outcome
The two groups were tested twice, preoperatively for baseline measurements and at 24 weeks postoperatively. A therapist with
Statistical analysis
The Shapiro-Wilk test was used to ensure normal distribution of all outcomes. The paired
Results
Twenty-six of the 30 participants completed the entire training session and posttest. One participant in the HBR group dropped out of the study because of personal scheduling difficulties. Three participants from the SR group dropped out: two were excluded due to overseas travel, and one was excluded due to relocation of residence. The dropout participants did not affect any demographic measures or outcomes at baseline in either group. The Student
A comparison of isokinetic knee strength demonstrated that postoperative isokinetic knee strength had significantly improved in both groups compared with the preoperative baseline results (
A comparison of proprioception demonstrated that postoperative proprioception in the SR group significantly increased from the preoperative baseline results, but in the HBR group, no significant difference was observed between the preoperative and postoperative outcomes (
No significant interaction effects were found between the covariates and the factors. The ANOVA revealed no significant differences in postoperative outcomes between the groups.
Discussion
This study was designed to investigate differences in
Isokinetic strength and proprioception scores in both groups
Isokinetic strength and proprioception scores in both groups
The mean changes in the pre- and post-test scores of each group are shown based on the results of the Wilcoxon test
isokinetic knee strength and proprioception improvement after participation in a HBR or SR exercise program in patients who had undergone previous ACL reconstruction surgery. After the 24-week intervention, we found that both groups showed a statistically significant improvement in the isokinetic knee strengths of the knee extensor and flexor muscles, except for KET in the HBR group. However, proprioception scores revealed a statistically significant decrease only in the SR group, indicating that proprioception improved only in the SR group. In addition, no statistically significant differences were found between the two groups in the isokinetic knee strength of the extensors and flexors, but a statistically significant difference in proprioception was observed between the two groups.
In the isokinetic knee strength evaluation, we found that both groups experienced significant improvements in all the measures except KET in the HBR group; however, no significant differences were found between the two groups. In a study by Grant and Mohtadi [30], patients who had undergone ACL reconstruction surgery were divided into two groups, a HBR group and a SR group. They received a structured rehabilitation program for the first 3 months after ACL reconstruction and underwent the first assessment, which was isokinetic knee strength at 60
In addition, isokinetic knee strength evaluated at 180
The anterior cruciate ligament plays a role as the primary restraint to anterior tibial translation and is the static stabilizer of secondary restraint against rotator instabilities of the knee [27, 28]. Anterior cruciate ligament injury can result in a decrease in functional performance, a misaligned neutral position, and in the modification of central motor programs [34, 35]. Ageberg et al. [34] previously reported that after acute ACL injury, both the injured and uninjured legs were affected by postural control. Although patients who had ACL injury could perform postural control exercises, their single-limb stance ability did not recover fully, although their functional performance was restored. However, no previous studies compared the restoration of postural stability between home-based exercise and supervised exercise groups after ACL reconstruction.
We found that both groups had significant improvements; however, proprioception showed a statistically significant improvement only in the SR group. In addition, the KET (a measure of quadriceps muscle endurance) in the SR group showed a significant improvement, but that in the HBR group did not show any improvement. Although a direct comparison is difficult, we think that this difference in KET could affect proprioception. Ekdahl [36] reported that isokinetic muscle endurance of the knee is related with postural control. The greater total work of an improved knee extensor can affect proprioception positively. In addition, our evaluation method for proprioception consisted of standing on one leg for 20 seconds. This method requires more muscle endurance rather than momentary muscle strength. Although the two groups had sufficient information for rehabilitation from the physical therapists, the SR group had an advantage over the HBR group in that they could receive feedback on their body posture and exercise position from the clinician. For this reason, proprioception in the SR group showed significant improvements, whereas proprioception in the HBR group did not. However, in their previous work, Ageberg et al. [34] insisted that in spite of functional performance recovery, sensory system injury might persistent. As a result of this injury, despite the improvement of proprioception in patients who had undergone ACL reconstruction surgery as compared with the preoperative status, patients still need more specific postural control exercises for full participation in activities of daily living or sports.
This study has some limitations. A functional test was not used; thus, it was difficult to prove that the improvements in isokinetic knee strength were related directly to knee function. As the patients in this study were young and could walk independently, we thought that improving isokinetic strength may have a positive effect on knee function in both groups on the basis of previous reports. Our rehabilitation program mainly consisted of closed-chain kinetic exercises that confer relatively low stress on the ACL because open-chain kinetic exercises of the knee joint could exert an excessive load to the ACL [37]. Thus, we have added a band exercise with low resistance in phase 4 to minimize adverse effects. Further studies may be interesting if the load in a training is progressively increased under special guidance. Despite these limitations, our study is the first research to evaluate endurance in relation to isokinetic knee strength and proprioception between HBR and SR after ACL reconstruction.
Conclusion
We found that HBR recovered knee strength as effectively as the SR, but SR was more effective than HBR for the recovery of proprioception and functional knee movement. This result indicates that patients may not be able to fully recognize their body position and postural status by themselves during a home-based intervention. Thus, in order to successfully regain functional status following ACL reconstruction surgery, patients may receive more guidance and correction when performing rehabilitation exercises under the supervision of a clinician.
Footnotes
Acknowledgments
The authors thank the participants who volunteered in this study.
Conflict of interest
None to report.