
Abstract
BACKGROUND:
Proprioception is essential for the normal movement of knee joints. How proprioception training affects the postoperative knee functional recovery after anterior cruciate ligament (ACL) reconstruction remains unknown.
OBJECTIVE:
This study investigated the effect of proprioception training on the knee joint kinematics of patients after ACL reconstruction (ACLR).
METHODS:
The randomized controlled study was performed at the Department of Orthopaedics and Traumatology of Guangdong Provincial People’s Hospital between December 2019 and April 2021. Forty-five patients who underwent ACLR were randomly divided into a proprioception group (
RESULTS:
After surgery, the proprioception group did not exhibit significantly higher hop distances than the control group at the 6-month (114.8
CONCLUSIONS:
The results suggested that proprioceptive rehabilitation training enhances knee joint functional performance and shows altered knee joint kinematics in ACL-reconstructed populations during unanticipated jump-cut maneuvering compared with the common rehabilitation training.
Introduction
The anterior cruciate ligament (ACL) is the most frequently injured knee ligament in sports [1]. Patients with ruptured ACLs often show knee instability, which may lead to degenerative changes and damage to other joint structures [2]. Athletes find it difficult to return to full function after ACL injury [3]. Recently, reconstructive techniques have been refined to achieve improved stabilization of the knee joint and, consequently, improved functional recovery [4]. Despite these efforts, the functional recovery of the knee after ACL surgery is still unsatisfactory in many cases [5]. The lack of full recovery of knee function after ACL reconstruction (ACLR) could be a result of sensory and motor behavior deficits.
It has been reported that ACL injury and reconstruction lead to the disruption of local mechanoreceptors that help maintain muscle co-activation and joint stabilization [6, 7]. Stimulation of mechanoreceptors in joint structures may stimulate the sensitivity of muscle spindles around the joint, in turn creating a state of readiness of muscles to respond to destabilizing forces applied to the joint and thereby improve active joint stability [8]. Accordingly, the recovery of proprioceptive functions after ACLR is critically important for restoring the strength, range of motion (ROM), and integrity of the graft. Therefore, proprioceptive exercises, which are defined as exercises that challenge stability and neuromuscular control, have been advocated in clinical practices [9]. The aim of rehabilitation after ACLR is to restore the patients joint stability and enable them to return to unrestricted, pre-injury levels of activity as safely as possible [10]. In recent years, rehabilitation programs following ACLR have become more aggressive than common rehabilitation programs, and proprioception training, neuromuscular training programs, and functional activities are all used in clinical practice [11, 12]. The purpose of these modified rehabilitation programs is to comprehensively enhance knee joint stability and aid in decision-making about returning to sports.
In a critical review, Han et al. [13] extensively investigated the role of proprioception in daily activities, exercises, and sports. However, few researchers have investigated the associations between proprioception and sports performance. Many researchers used passive angle reproduction and joint position sensing (JPS) to evaluate proprioception recovery [14]. However, these outcomes such as passive angle reproduction and JPS are associated with static sensation ability, which cannot be used to predict dynamic sensations in movement. Moreover, dynamic sensation is positively correlated with rotational stability in daily life activity, positive sports performance, and injury prevention and re-injury prevention after ACLR [15]. The kinematics involved in the jump-stop, unanticipated cut (JSUC) maneuver have not been investigated before in ACL-reconstructed populations [16]. Therefore, it is critical to evaluate the efficacy of proprioception training in restoring dynamic motions. Nagai et al. [17] revealed the relationship between knee proprioception and strength and landing kinematics and found that individuals with enhanced proprioception and muscular strength had better control of initial contact knee flexion angle during a dynamic task. However, the investigation was focusing on physically active men instead of ACL-reconstructed populations. The effect of proprioception training on knee kinematics in ACL-reconstructed populations remains unknown.
Although sensory and motor changes have been described in individuals with ACL lesions, such changes have not been well described in individuals who have undergone ACLR [18]. After ACLR, these sensory and motor changes vary more than they did before, and therefore, they are difficult to describe [19]. Even though proprioception cannot be directly measured, it affects the knee joint kinematics during highly demanding motion tasks, such as loading and extreme rotation conditions [20]. The current study is the first study to investigate the kinematic alterations during highly demanding motion tasks after proprioceptive rehabilitation training in ACL-reconstructed populations. Therefore, in this study, we compared the functional activity levels and knee joint kinematics of ACL-reconstructed knees among patients who underwent a proprioception rehabilitation program and a common training program.
CONSORT flowchart.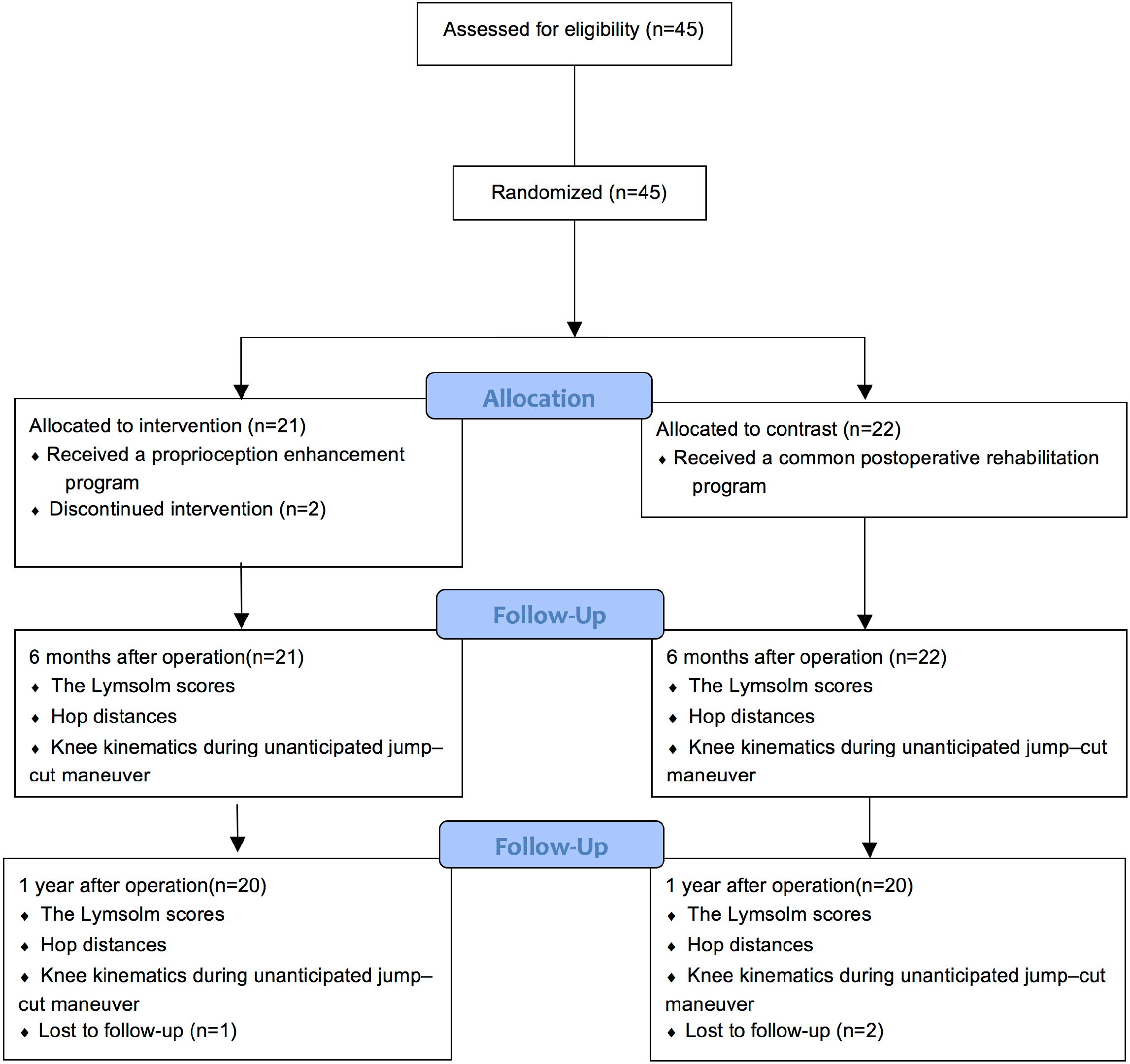
Participants
Between December 2019 and April 2021, 45 patients who underwent ACLR involving a hamstring graft technique were recruited for this study (Fig. 1) at the Orthopaedic Research Center of our institute. The included patients were asked to perform preoperative rehabilitation program, which was followed by ACLR postoperative rehabilitation program. The experimental group contained 23 patients and the controlled group contained 22 patients. Ethical approval for the study was obtained from the institutional review board of the Orthopaedic Research Center (Approval number: KY-N-2021-005-02). The study was registered at chictr.org.cn (ChiCTR2100045292). All included patients signed an informed consent form. The patients were randomly divided into an experimental group and a control group according to whether the final digits of their ID numbers were odd (experimental group) or even (control group). Only patients who met the following criteria participated in the study: (1) They only underwent one surgery for a tear of the ACL (2) they were between the ages of 18 and 40 and (3) International Knee Documentation Committee (IKDC) radiographic grading system was used to assess the degeneration of the knees [21], and patients were graded less than Grade B. Patients who met the following exclusion criteria were removed from this study: (1) They underwent a concomitant tear of the posterior cruciate ligament; (2) They had a history of collateral ligament repair, (3) They had a history of contralateral knee injury or surgery, (4) They had a history of ankle injury or surgery, (5) They had hip trauma or surgical history, (6) They had complications with severe primary diseases of cardiovascular, cerebrovascular, liver, kidney, endocrine, or hematopoietic systems, (7) They had emotional and mental disorders, and (8) They were pregnant women. The patients were clinically evaluated before participating in testing. None of the patients or controls had instability or additional lesions during the study period. None of the patients were graded over IKDC Grade B, which means the initial radiographic statuses of the knee joints of the two groups were comparable.
Common rehabilitation program
Common rehabilitation program
Proprioception training program
Proprioceptive training and testing procedure. [Panel a] Proprioceptive training: open eyes in a single-leg stance using the involved limb on a cushion. [Panel b] A demonstration of JSUC maneuver motion during the testing procedure. [Panel c] A crossover cut was performed when patients were landing to collect knee knees. A: The path direction after crossover cut for left feet; B: The path direction after crossover cut for right feet.
For sample size estimation, knee joint kinematics served as the primary study outcome. Specifically, internal – external tibial rotation was used as a determinant outcome of this study to calculate the sample size. Because no previous reports guided the expected results, our preliminary pilot data guided our calculations. Based on our previous study with a control group and a proprioception training group, we noted the average tibial rotations as 36.4
Before the ACLR, all included patients performed the same preoperative rehabilitation program to regain the strength and movement in the involved knee to improve the functional recovery after surgery. For the common rehabilitation program, all patients underwent a standardized rehabilitation protocol [23]. The details about the protocol can be found in Table 1. Apart from the common rehabilitation program, the proprioception group accepted proprioceptive training (Fig. 2a). The details can be found in Table 2. The proprioceptive rehabilitation protocol was based on a previous study [24]. The program was conducted by one experienced physiotherapist. For the blinding purposes, a double-blinded procedure was followed. The patients were not told what kind of training they were accepting to avoid performance bias. Besides, the physiotherapist did not know the grouping of the included subjects or whether his patients were subjects in this study.
Outcome measures
Lysholm scores were used to assess patients abilities to manage daily activities [25, 26]. Based on previous studies associated with the minimum clinically important difference (MCID) of Lysholm scale, the MCID score for Lysholm scores were set at 8.9 [27, 28]. The kinematic assessment protocol used in this study was the following: before testing, patients were required to complete a 5-minute warm-up on a stationary exercise bike. For the kinematic assessment, a portal optical tracking system (Opti_Knee, Shanghai Innomotion Company) was used to collect kinematic data about ACL-reconstructed knees during JSUC. This validated system was used in previous studies [29, 30]. Firstly, spatial orientation was identified for bone landmarks with the assistance of handheld markers, including the greater trochanter of the femur, lateral and medial femoral condyle, lateral and medial tibial plateau, lateral fibular head, tibial tubercle, and medial and lateral malleolus. Two infrared inductors were fixed on the distal femurs and proximal tibias of participants. Three-dimensional coordinate systems for the femur and tibia were built based on the bone landmarks in the system. Rotation was defined as the tibia rotation along with the origin of the coordinate system in the femur. Similarly, displacement was defined as the tibia movement relative to the origin of the coordinate system in the femur.
Demographic information of the included subjects
Demographic information of the included subjects
Values indicate the mean (standard deviation).
Lysholm scores, hop distances and kinematics measured between the two groups. [Panel a] Lysholm scores measured in the common training group and the proprioception training group, *: denoted as 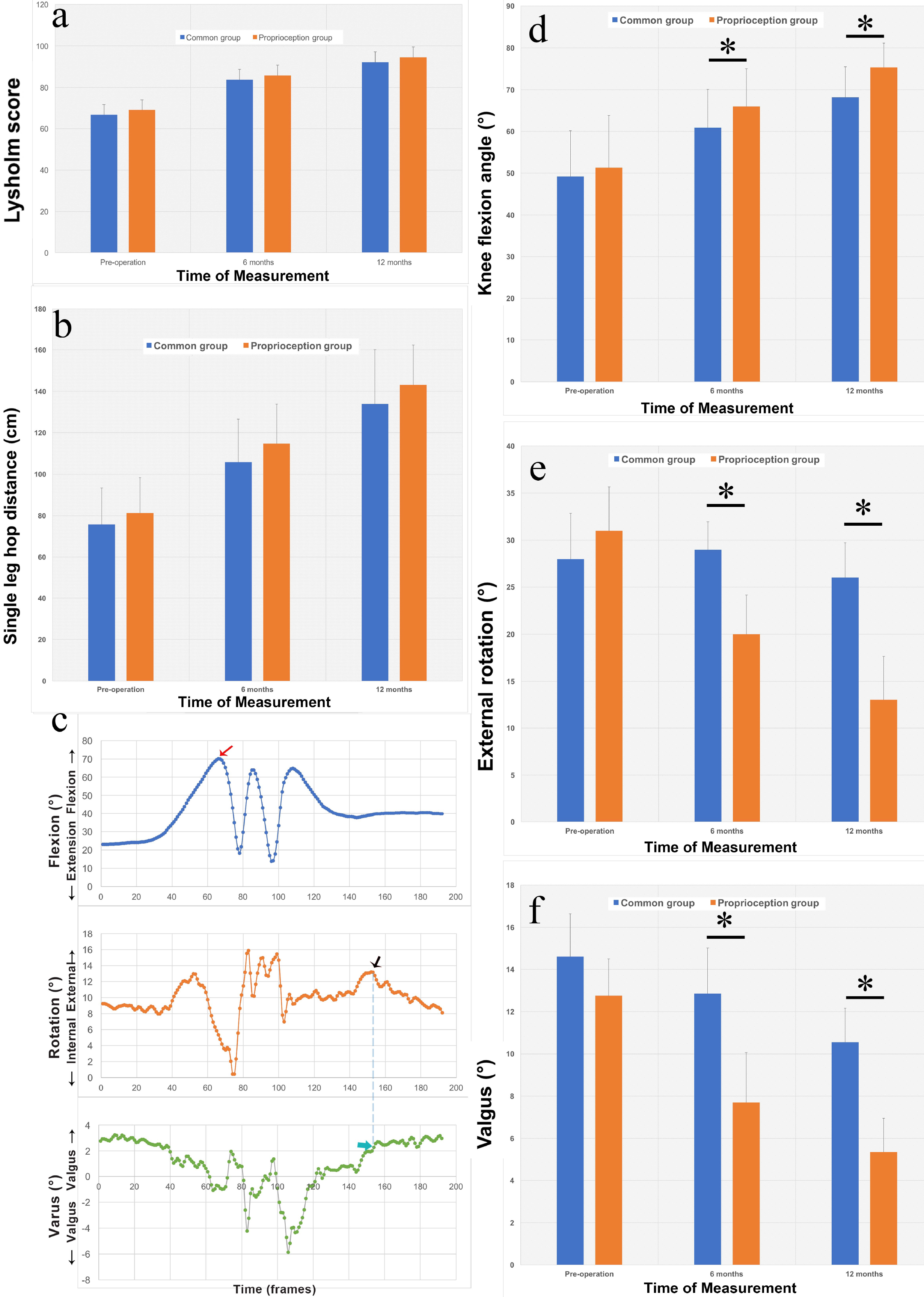
The patients were shown how to perform the JSUC and allowed to practice the maneuver without observing the visual unanticipated direction cue. This maneuver was selected due to its common occurrence in sports and high potential to cause ACL injuries. The incorporation of unanticipated elements into testing protocols may better mimic the demands placed on the lower extremities during sports. Each subject was positioned in an athletic ready position to react to randomized, unanticipated direction cues. The ready position was established before the cutting trials commenced. The subject was asked to perform a single-leg hop. When landing, the subject was instructed to perform a sidestep cut at 45 degrees and run past a marker 2.5 m away (Fig. 2b). The subjects were asked to perform a crossover cut immediately when they landed on the floor because the knee demonstrated valgus and external tibial rotation with this movement (Fig. 2c). It is well established that this position is a risk factor for ACL injury. A custom computer program was used to signal left and right on a digital monitor to cue the subjects when they were going to land within 0.3 seconds. The subjects were instructed to reposition their knees to the same flexed position before the start of each JSUC trial. The patients were asked to try to perform all JSUC trials in consistent postures to minimize variations of movement.
The patients were asked to perform a total of six trials, three for each knee. The orders of trials were randomized to examine the patients’ performance reactions to unanticipated movement direction ques. After testing, we only exacted the data when patients performed JSUC maneuvers. Kinematic data were collected over 15 seconds at a frequency of 60 frames per second. Rotational motions were analyzed, including abduction and external rotation at toe-off when cutting and peak flexion angles during single-leg hop tests. Upon data collection, these parameters were calculated and compared between the two groups preoperatively, as well as 6 months and 12 months postoperatively.
For demographic data about the included patients, the time between injury and reconstruction were compared between the two groups using independent
For kinematics, the peak values of knee flexion angles during single-leg hopping, abduction – adduction angles, and external tibial rotations during cutting were compared using two-way repeated-measures ANOVA at different follow-up times. The dependent variables were kinematics as mentioned above. The independent variables were the training conditions (proprioceptive and common training) and follow-up timing (preoperatively, 6 months after operation, 12 months after operation). The significance threshold was set to 0.05. Statistical analysis were conducted in SPSS22 (IBM, Armonk, NY, USA).
Results
Forty patients finished the testing procedures at different follow-up times (20 patients in the proprioception group and 20 patients in the control group). Three patients in the proprioception group and two patients in the controlled group did not complete the study. The demographic data about the included patients are shown in Table 3. No significant differences were found in gender, age, BMI, dominant side, or the time between injury and reconstruction between the control group and the proprioception group.
The Lysholm scores are shown in Fig. 3a. There were no significant differences between the two groups in preoperative Lysholm scores. However, the patients in the proprioception group had higher Lysholm scores at both 6 months (85.7
For hop distances (Fig. 3b), no significant differences were identified between the two groups preoperatively (
Clinically, for knee joint kinematics, the MCID for knee translational changes are 5 mm and 3
The proprioception group showed decreased external knee rotation angles compared to control group at the 6-month (20.0
Discussion
The purpose of the current study was to compare dynamic knee function and knee joint kinematics between patients who underwent a common rehabilitation program and a proprioception training program. The results suggested that proprioceptive rehabilitation training enhances knee joint functional performance and shows altered knee joint kinematics in ACL-reconstructed populations during unanticipated jump-cut maneuvering compared with the common rehabilitation training. These findings support our hypothesis that proprioception training programs enhance dynamic knee function. These findings could be used as evidence to support the efficacy of the use of proprioception training in the recovery of rotational knee stability in unanticipated cutting, which is a positive indication for any injury prevention program aimed at reducing ACL re-injury after ACLR.
The Lysholm scores indicated that both the proprioception training program and common training program could help patients manage daily activities after ACLR. However, no significant differences between the two training programs were identified. The Lysholm scale was used to measure the domains of symptoms and complaints and slightly measure functionality in daily activities, but it was not used to measure functionality in sports and recreational activities, such as motion tasks [32]. Therefore, scales like Lysholm scores cannot be used to comprehensively evaluate knee function.
In highly demanding tasks, such as jumping and side cutting, the ability to control dynamic movement is crucial and extremely important for the prevention of ACL re-injury in ACL-reconstructed populations. Single-leg hop distance was used as a movement that is comparable to the high functional demands in sports for analysis [33]. It is already used as a functional test for lower extremities and has turned out to be a reliable measure [34]. Although the findings of the present study indicate that proprioceptive training does not lead to significant improvements in helping ACL-reconstructed patients restore readiness for sports, the higher hop distances we observed in the proprioceptive group compared to the control group imply that patients may benefit from additional training due to the improvement of proprioception. We speculated that this is because the patients in the proprioceptive group had increased confidence concerning their ability to control their postures and balance during the high functional demanding task. The collection of further data from larger study populations is warranted.
Specifically, the patients in the proprioceptive group showed increased knee flexion angles compared to those in the control group 6 months after their ACLR operations. Similarly, one year after operation, the participants knee flexion angles were greater than those measured 6 months after operation. Nagai et al. reported that enhanced knee proprioception and greater knee strength were correlated with increased knee flexion angles at initial contact during a single-legged stop-jump task [17]. With increased knee flexion angles during landing, proprioception may be enhanced due to the increased afferent mechanoreceptor feedback associated with the loading of the ACL
The proprioception group showed reduced external knee rotation compared to the control group. One of the main functions of the ACL is to maintain rotational knee stability. ACL-reconstructed knees demonstrate greater internal–external rotation than healthy ones, especially during loading and under extreme rotation conditions [35]. In this current study, ACL-reconstructed knees in the proprioceptive group showed decreased external knee rotation during JSUC maneuvers. The significantly reduced external knee rotation observed in the proprioceptive group indicated that proprioception training is beneficial to the restoration of rotational knee stability. We speculated that the enhancement of rotational stability is associated with the increased mechanoreceptor function via proprioceptive training on the knee joint.
The patients in the proprioception group showed reduced knee abduction (valgus) angles compared to those in the control group. It is well established that one of the most common mechanisms of noncontact ACL injury is dynamic knee valgus [36]. Knee joint valgus is often found to be a hazardous position for the ACL due to the increased shared loading between the ligament and the bone in this position. In the present study, the proprioceptive group showed an enhanced capacity to make the knee joint expose a significant valgus position. This capacity improvement is crucial to preventing ACL re-injury among ACL-reconstructed populations.
Certain limitations exist in this study. Firstly, we did not measure the contralateral ACL-intact knee as a control. Secondly, simultaneous myasthenic and electromyographic analysis were not used to measure kinematics, which may have affected our understanding of the kinematic results. Thirdly, the follow-up period was relatively short. In further studies, mid-term and long-term follow-ups should be investigated and the durability of changes exhibited in the current study can be further assessed. Besides, future studies should include several ACLR techniques to generalize the results.
Conclusions
Proprioceptive rehabilitation training enhances the kinematic performance in ACL-reconstructed populations during JSUC maneuvers. The findings are scientific evidence that will help clinicians and physiotherapists evaluate ACL-reconstructed patient readiness for exercises and sports.
Footnotes
Acknowledgments
The authors acknowledge the contributions of all patients recruited in the present study.
Conflict of interest
The authors have no conflict of interest in this study.
Funding
This study was supported by the Doctor Launch Fund of Guangdong Provincial People’s hospital (grant number: 2020bq10), the National Natural Science Foundation of China (grant number: 81874032, 82072528, 82002380) and the Project of Administration of Traditional Chinese Medicine of Guangdong Province of China (No. 20211006).