
Abstract
BACKGROUND:
Flexibility changes according to stretching intensity have been rarely investigated. I aimed to assess the effect of different stretching intensities on hamstring flexibility by measuring them in a setting similar to real clinical settings.
METHODS
: Stretching intensities were quantified using an easy method, and participants were grouped according to intensity: 100% (P100), 70% (P70), 40% (P40), and 10% (P10) of maximum voluntary isometric contraction. Proprioceptive neuromuscular facilitation stretching intensities were measured using a sling system and tension dynamometer. Hamstring flexibility was measured (before; immediately after; and 3, 6, 9, 12, and 15 min after stretching) using the active knee extension test. Flexibility was compared between subgroups, and longitudinal changes in flexibility were additionally observed in each group.
RESULTS:
At identical time points, no significant difference in hamstring flexibility was found between the high-intensity (P100) and moderate-intensity (P70, P40) groups. A significant difference was found between P100 and P10 immediately after and 12 and 15 min after stretching. Increased flexibility was maintained until the end in P100 and P70 but not P40 and P10.
CONCLUSIONS:
High-intensity and moderate-intensity stretching increases flexibility compared with low-intensity stretching. Furthermore, high-intensity stretching was superior to moderate-intensity stretching in terms of maintaining flexibility over time.
Introduction
Whether stretching can reduce the risk of injury during exercise remains controversial. Although some studies [1, 2, 3, 4] have verified this concept, others [5, 6, 7] have reported no effects of stretching on injury risk. Even among studies that have reported beneficial effects, it is unclear whether the effects were caused by stretching alone or by stretching and other factors. Nevertheless, accumulated evidence has shown that stretching reduces the risk of injury in general, and this finding has recently been accepted and supported by other studies. Accordingly, current clinicians and researchers consider flexibility to be important [1, 2, 4]. Flexibility is considered especially important in sports that involve short-duration, high-intensity work with a wide range of movements (e.g., soccer and basketball) compared with sports that involve low-intensity effort over a long duration (e.g., long-distance running) [8, 9]. Various methods for increasing flexibility have been tested, with stretching being the most widely used method not only in athletes but also in normal subjects.
Various stretching techniques have been attempted; they are generally broadly classified, according to how they are performed, into static, ballistic, and proprioceptive neuromuscular facilitation (PNF) techniques. Among these techniques, PNF stretching is usually preferred. This stretching technique consists of 3–10 s (usually 6 s) of isometric contraction followed by a 10-s break. The effectiveness of stretching is mainly affected by its duration and intensity. Although various studies have been conducted on stretching duration, research on stretching intensity has been limited. Relatively more studies have been conducted on the intensity of static stretching than on PNF stretching, possibly because static stretching is easier to perform and examine. The intensity of static stretching is determined according to the amount of pain felt during stretching. According to the literature, static stretching is most commonly performed until the point of discomfort (POD). It is also performed until just before discomfort [10] or until less than the POD [11]. The submaximal contraction intensity may also be categorized relative to 100% of POD during static stretching. Previously, the intensity of static stretching was determined on the basis of subjective assumptions [11], or 90% of the angle measured at POD during a pre-test was used as the 90% stretching condition [12]. However, because POD itself is significantly influenced by individual subjective factors, it could not be considered an objective measure of stretching intensity. In another study, a cable strain gauge system was used to classify intensities into 100%, 75%, and 50% of POD instead of relying on subjective factors [13]. Recently, intensities were set to 100%, 75%, and 50% of the maximum tolerated joint passive torque, as measured using a Biodex dynamometer [14, 15].
In a previous study, PNF stretching was performed using a FlexAbility machine until up to 50% of the maximum voluntary isometric contraction (MVIC); however, this study focused on hemodynamic effects rather than on the effects of PNF stretching [16]. Thereafter, Feland and Marin [17] divided stretching intensities into 100%, 60%, and 20% of the MVIC, and Khodayari and Dehghani [18] divided stretching into 100%, 80%, 60%, 40%, and 20% of the MVIC and verified the effects of PNF stretching. In both experiments, PNF stretching had significant effects on flexibility not only at 100% but also at 20%. Biodex is an excellent isokinetic dynamometer for categorizing the submaximal contraction intensities of PNF stretching. However, many clinics consider it a low-priority purchase because of its high cost. Moreover, it is a complicated machine that has a learning curve and requires additional time for experimental preparation and data analysis. Furthermore, Biodex is difficult to use in the supine straight leg raise (SLR) position, which is the usual position used for PNF stretching in the clinical setting. Previously, PNF was performed in the sit upright at 90
The aims of this study were to 1) assess the effect of different intensities of PNF stretching on the flexibility of the hamstring, which is most commonly injured during exercise, by measuring the stretching intensities in a setting similar to real clinical settings, 2) observe longitudinal changes in flexibility over time at each intensity, and 3) examine the correlation between the individual target intensities and flexibility gains.
Methods
Subjects
Fifty-three young and healthy adults participated in the study (23 men, 30 women; age 22.19
Procedures
The participants were randomly divided into the following four groups according to intensity: 100% (P100), 70% (P70), 40% (P40), and 10% (P10) of MVIC. They started with the knee fully extended, then flexed to 90
Hold-relax PNF stretching using a sling system with a wireless tension dynamometer.
The subjects performed hold-relax PNF stretching using a sling system (Marpe Inc., Jeonju, Korea). First, the ankle of the dominant leg was placed in the sling ankle strap, and then the subject assumed the supine SLR position. The sling was positioned such that the lower limb was perpendicular to the sling rope attached to the ceiling. The other leg was secured on the treatment table with a belt during the PNF stretching. Additionally, a wireless tension dynamometer (Re-live Inc., Kimhae, Korea) was connected between the sling rope and ankle strap for real-time monitoring of the intensities of isometric contraction on an LCD display (Fig. 1). Maximum isometric contraction of the hamstrings was performed three times (10-s hold, 5-s rest between contractions) for the 100% MVIC measurement. After a sufficient break, isometric contraction, only up to the assigned intensity by group, was performed six times (10-s hold, 5-s rest between contractions). The AKE values immediately after stretching were recorded as post-stretching measurements. AKE values were additionally obtained at 3, 6, 9, 12, and 15 min after stretching. A practitioner helped prevent the subject’s suspended leg from moving side to side during PNF stretching.
One-way analysis of variance (ANOVA) was used to compare the MVIC values and target intensities among groups. A paired t-test was used to compare the MVIC and target intensity within groups. One-way repeated-measures ANOVA and the Bonferroni post-hoc test were used to analyze differences in AKE at identical time points between groups and the changes in AKE over time in each group. The Pearson correlation test was used to examine the correlation between each subject’s target intensity and flexibility gain at each time point. Data analysis was performed using IBM SPSS Statistics 23 (IBM Corp., Armonk, NY, USA). Statistical significance was set at
Maximum voluntary isometric contraction (MVIC) and target intensity calculated at assigned percentages.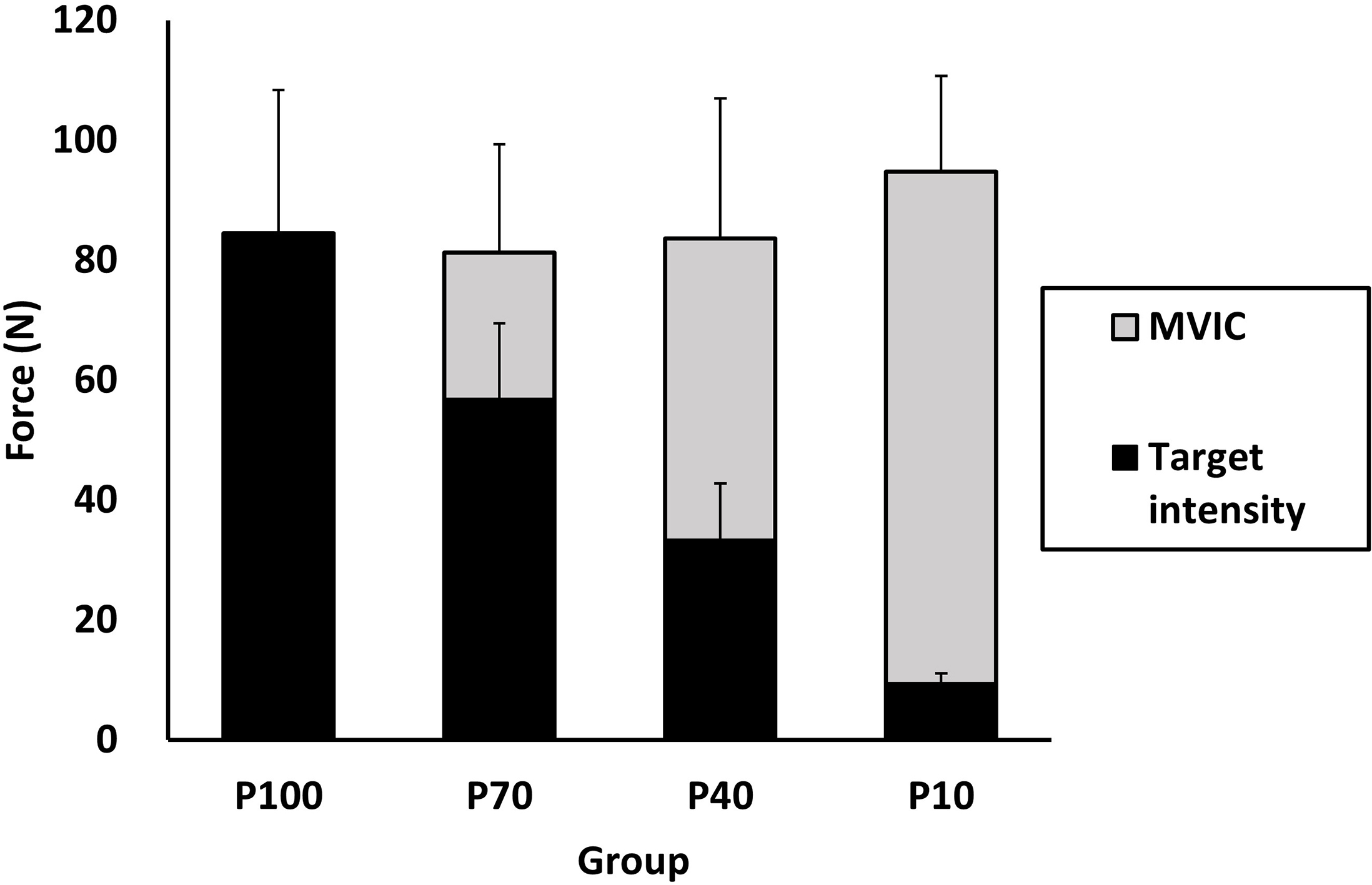
The MVIC range of the four groups was 83.65–94.77 N, with no significant difference in MVIC among groups (Fig. 2). Significant differences in target intensity were found among the groups (
Longitudinal change in active knee extension (AKE) by group.
Correlation between individual target intensity and active knee extension (AKE) measured immediately after stretching (post) and at 15 min post-stretching.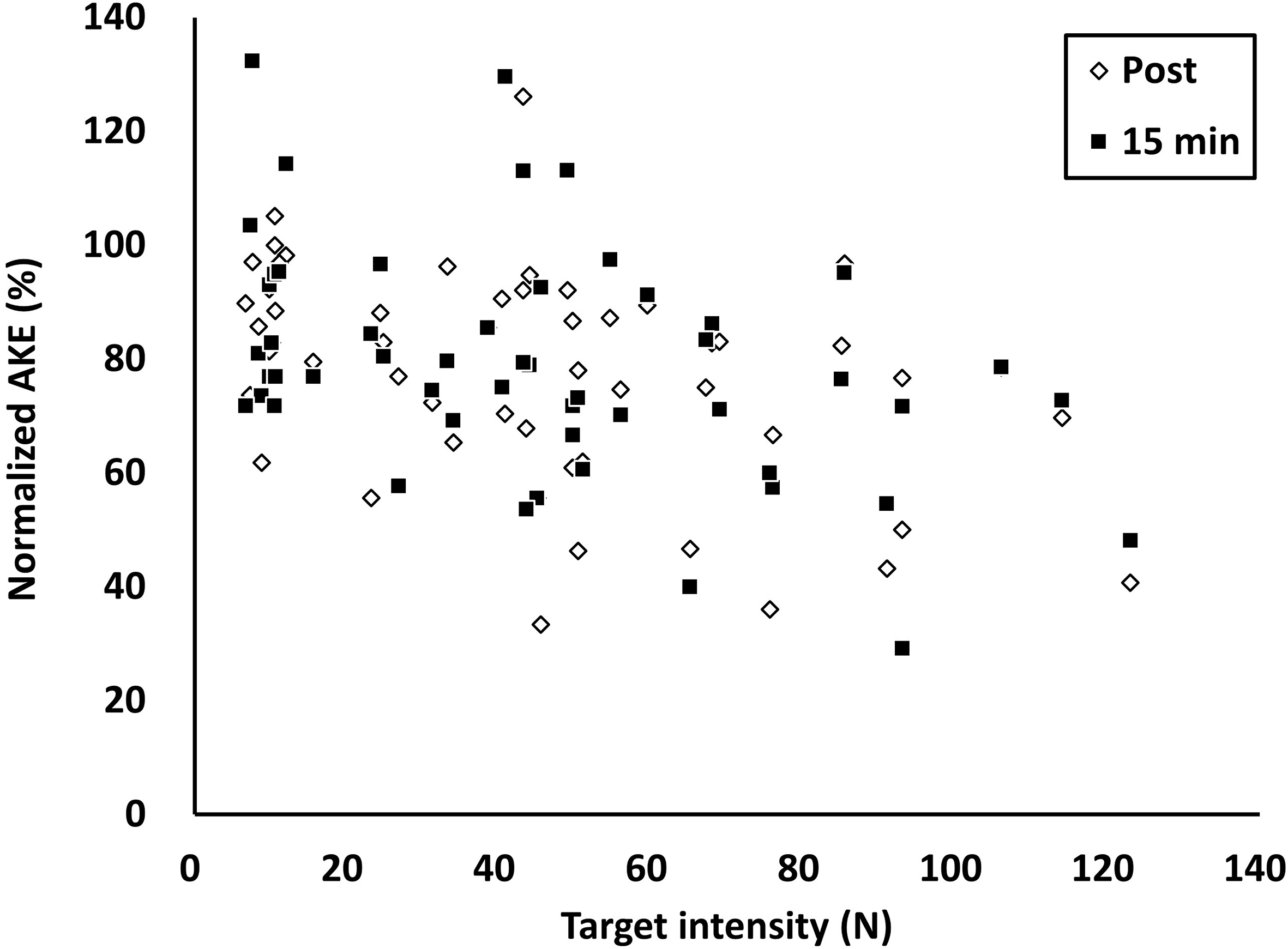
The importance of lower-extremity flexibility has been emphasized, and various stretching techniques have been suggested for increasing flexibility. Duration and intensity are the two main factors known to influence the effects of stretching. Studies on stretching intensity are relatively fewer than those on stretching duration. This study observed longitudinal changes in hamstring flexibility over time in subjects who performed stretching at different intensities to investigate how different stretching intensities affect the changes in the flexibility of the hamstring muscle. The correlation between individually assigned stretching intensities and flexibility gains at different time points was also analyzed. Unlike that in previous studies, stretching intensities were calculated using measurements obtained with a digital tension dynamometer and were quantitatively assigned to individual subjects in this study. All participants performed PNF stretching in the supine SLR position on a treatment table rather than on laboratory equipment as in the real clinical setting. Stretching had significant effects not only on the high-intensity group (P100) but also on the moderate-intensity groups (P70 and P40). However, when changes in flexibility over time were analyzed for each group, the effects of stretching on the maintenance of flexibility were more stable in the high-intensity group than in the moderate-intensity group. A significant correlation was observed between individual stretching intensities and flexibility gains at most time points, indicating that the higher the intensity, the higher the flexibility increase, and this increase is maintained for a certain amount of time after stretching.
There were clear differences in the assigned stretching intensities among the four groups. Determining the stretching intensity according to personal intuition or assumption, to analyze the effects of stretching at different intensities, can lead to a large error between the target intensity and the actual intensity applied [21]. In the previous study, two groups (50% and 20% of MVIC) were formed according to the submaximal contraction intensity, in addition to the 100% of MVIC group. The subjects were blinded to the contraction intensity that would be measured during PNF stretching and had to guess the intensity according to their subjective judgment. The results showed a large difference between the actual and target contraction intensities. The actual contraction intensities were widely distributed throughout half of the MVIC range, rather than the target intensity range, indicating a large overlap between the groups despite the fact that the groups were assigned with different intensities. Given that the stretch tolerance, sensory threshold, and their reintegration vary among individuals [22], stretching intensity must be determined objectively rather than subjectively. In the present study, a tension dynamometer with a sling system was used to measure the hold-relax PNF stretching intensities. After the MVIC measurements, the subjects controlled their PNF stretching intensities in the form of visual bio-feedbacks according to their assigned target intensities while monitoring the intensity values on the LCD screen of the tension dynamometer. The subjects easily maintained their assigned intensities during stretching. Unlike Biodex, which has been used in previous studies, a tension dynamometer does not require much space, does not have a learning curve, and is more clinically friendly because stretching is performed in the supine position.
The results of this study suggest that the flexibility differences according to the PNF stretching intensity may be explained by categorizing the stretching intensity into high, moderate, and low levels. First, on comparing the flexibility between groups at identical time points, only the low-intensity P10 group showed significant flexibility differences relative to the maximal intensity P100 group. The moderate-intensity groups, P70 and P40, showed no significant differences relative to P100 at all time points. However, in the analysis of flexibility maintenance at the assigned intensities (i.e., flexibility changes within each group over time) rather than flexibility differences according to stretching intensity (i.e., comparison between groups at identical time points), there was no significant flexibility change after 6 min relative to the pre-stretching value in P40. This means that the flexibility increase resulting from stretching was maintained for longer in P100 than in P40. Flexibility increase according to stretching intensity cannot simply be explained by changes in the length of the musculotendinous unit (MTU) and may require a neurological and physiological understanding of muscles. The effects of stretching can largely be explained by viscoelastic adaptation of the MTU and neural effects. An increase in ROM due to viscoelastic properties of tissues, such as stress relaxation and creep that occur after stretching, leads to decreased muscle stiffness, which represents a resistance against movement within the ROM or increased muscle compliance. It has also been reported that PNF stretching inhibits tonic reflex activities to increase ROM [23]. Owing to these neurological properties, some studies claim that submaximal and progressive PNF stretching is more effective. In a study that involved knee contraction, low-load prolonged stretching was more effective than high-load brief stretching [24]. It has also been claimed that moderate-intensity PNF stretching is optimal for inducing viscoelastic changes, as it reduces the inhibition on flexibility increase by the stretch reflex, which is a property of the muscle spindles, and enhances the flexibility increase by autogenic inhibition of the Golgi tendon organ [21]. However, some studies argued that high-intensity stretching is more effective than long-duration stretching [24, 25, 26]. As the effects of stretching are affected by both duration and intensity [27], to investigate the effects of stretching at different intensities independently, all factors that can affect the result must be controlled, and under this condition, high intensities can lead to the achievement of higher flexibility [21].
The minimum intensity that can lead to an improvement in flexibility might be 10% or 20% of MVIC. Whereas stretching intensities of 20% of MVIC led to flexibility increase in previous studies, there was no ROM increase in the 10% of MVIC group in this study [17, 18]. In this experiment, the torque loaded on the sling is the sum of the hip extension torque that arises from the hamstring muscle (i.e., distance from the hip joint axis of rotation to the sling strap attached to the ankle multiplied by the tension force on the sling cable) and the torque due to the effect of gravity on the lower extremity (i.e., distance from the hip joint axis of rotation to the center of mass of the lower extremity multiplied by the gravitational force on the lower extremity) [28]. Therefore, as the two factors (lower-extremity mass and SLR angle) affect the force loaded on the string, there can be a difference between the measured and actual loads on the MTU of the hamstring. Overall, it is estimated that the hip extension torque that arises purely from the hamstring might be lower than the intended intensity in this study for the moderate- and low-intensity groups (P70, P40, and P10).
In the analysis of the correlation between individual target intensity and flexibility gains at different time points, normalized AKE values were significantly correlated with the target intensity at all time points, except at 3 min after stretching. To explain in more detail, the coefficient value decreased from post-stretching to 3 min, and gradually increased thereafter, resulting in a high value at 15 min as that at post-stretching. Overall, a significant ROM increase was observed at higher intensities, and the increased ROM was stably maintained not only immediately after stretching but also until the last time point (15 min after stretching). This may partially explain the differences between the low- and high-intensity groups shown in Fig. 3, and how the acquired flexibility was stably maintained in the high-intensity group. Tissue with higher stiffness has less capacity for energy storage during stretching [29]. Thus, higher-intensity stretching may increase the energy storage and reduce the injury risk. However, stretching at excessively high intensities can increase the potential risk of contraction-induced injuries [30]. In Fig. 4 showing the acute stretching effects, a large distribution of AKE values close to 100% of the pre-stretching values can be seen in the low-target-intensity ranges at post-stretching. This might indicate the importance of the minimum stretching intensity threshold for inducing physiological changes in tissue length. At 15 min, AKE values exceeding 100% of the pre-stretching values can be seen in the low-target-intensity ranges but not in the high-intensity ranges. It seems that the six repetitions of AKE performed as warm-up before stretching caused a temporary increase in ROM, and this increase was reflected in the pre-stretching AKE values [31]. It also seemed that the increased ROM after warm-up gradually decreased over time in the participants who performed low-intensity stretching. In a previous study on the effects of stretching intensity, warm-up was not performed [15]. In this case, the increase in flexibility after stretching may have been exaggerated even at low intensities.
This study has several limitations. The participants in this study were in their early 20s, and the number of participants in each group was quite small. Hence, the findings of this study may not apply to the general population. Additional studies involving a larger population with varying ages are required in the future to reflect the characteristics of the general adult population.
In conclusion, stretching intensities were easily measured using the method in this study, which can also be easily applied in the clinical settings. I found that high- and moderate-intensity stretching are superior to low-intensity stretching in terms of improving flexibility, and that high-intensity stretching is superior to moderate-intensity stretching in terms of maintaining flexibility.
Footnotes
Acknowledgments
This research was supported by 2018 Woosong University Academic Research Funding and a Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Education (NRF-2017R1C1B5076885).
Conflict of interest
The author has no conflict of interest to disclose.