
Abstract
BACKGROUND:
Pain relief is important both for the movement of patients suffering from low back pain and the quality of life. Dry needling is effective on myofascial trigger points but its effect on the area of pain and the functional balance is not fully known.
OBJECTIVE:
To examine the immediate effect of dry needling on pain and functional balance of patients suffering from low back pain.
METHODS:
Twenty five patients with sub-chronic low back pain were randomly divided into two groups: the intervention or control group. Needles were used for the participants of the intervention group, bilaterally at the spinus level, one and a half finger breath from the midline in levels L2–L5 of the lumbar spine. A third line of needles was inserted in the interspinosus spaces, except L5-S1 level. Bipedal stance, lateral loading and mediolateral body sway were assessed using a pair of force plates. Pain tolerance was assessed using an algometer.
RESULTS:
The pain tolerance significantly increased in the intervention group from (M
CONCLUSIONS:
Dry needling in painful areas and penetrating all the muscle groups seems to improve pain and functional balance, yet its effect on specific muscles needs to be studied further.
Introduction
Good functional balance is a key element for the quality of daily living [1]. Pain relief and improvement in functional balance is a primary goal in the rehabilitation of patients suffering from reported low back pain (LBP). Patients with LBP frequently report poor balance [2] and greater postural sway in comparison to healthy controls in upright standing [3]. They also demonstrate decreased body perception, diversified proprioceptive postural control [4] and greater weight-bearing asymmetry, associated with increased levels of pain, compared to healthy people [5]. It is found that measurements in the mediolateral plane can reliably describe balance problems of patients with LBP [6]. Alterations in postural sway of patients with LBP are reported in the majority of papers. An increase of postural sway is the most common finding but the literature is not conclusive. There is a minority of papers that show a decrease of postural sway in patients with low back pain [7]. The effect of different kinds of treatments of LBP in static and dynamic balance is frequently investigated [8]. An important issue, related to the duration of pain, is the change of the “mechanical” behavior of the patient [9]. They may serve as a protection strategy in the short term, yet the long term motor changes may be well established and remain even if the actual cause is resolved [10], requiring more effort to be reversed.
Pressure algometry, which is defined as the pressure that produces minimum pain perceptible by a person, is reported to be reliable in the pathological mechanisms involved in muscle pain syndromes [11]. Pressure pain threshold (PPT) is measured in various musculoskeletal conditions. According to Fischer’s definition, a difference of more than 2 kgr/cm
Dry needling (DN) is used to treat a variety of pain syndromes [15, 16, 17] and there is a growing body of literature that investigates its clinical effectiveness in the treatment of musculoskeletal pain [18]. DN is reported to be an important supplement of conservative treatment in the management of LBP [19]. DN causes alterations of blood flow to the muscles. Disturbances of blood flow following DN are found in patients suffering from fibromyalgia, work-related trapezius myalgia and low back pain [20].
Dry needling is reported to improve pain. Yet little is known about the result of DN on balance and functionality [21]. The purpose of the present study was to investigate the immediate effects of dry needling on sub-chronic low back pain patients upon the lumbar paravertebral muscles considering pain relief, and its effect on balance.
Methods
Participants
Twenty-five patients of both sexes with chronic LBP voluntarily participated in the present study. Patients were chosen from a larger group according to the following inclusion criteria: Patients were asked to draw their pain on a diagram of pain according to the study by Simons et al. [22]. The drawing of pain had to be located from the lower rib to the lumbar and sacral area and the reported pain had to be present from 6 weeks up to 3 months. Patients had no sign of sciatica, neurological deficit, spine trauma or surgery, pregnancy or pelvic pain. They were also free of rheumatic or infectious diseases, psychiatric or cancer history, metabolic (diabetes or thyroid diseases), coagulopathies or use of anticoagulants and neuromuscular degenerative diseases. They were randomly assigned to a control or intervention group. The control group (CG) consisted of 8 women, 39.2 (SD: 17.4) years, 81.3 (SD: 18.6) kg, 5 men 32.7 (SD: 21.1) years, 96 (SD: 24.6) kg. The intervention group (DNG) consisted of 8 women, 48.8 (SD: 16.2) years, 74.6 (SD: 17.8) kg, 4 men, 54.6 (SD: 24.4) years, 80.4 (SD: 6.7) kg. Experiments were performed with the approval of the local ethics committee on human research in accordance with the Declaration of Helsinki. Patients were analytically informed about the procedures and signed a consent form prior to their participation.
Patients were assessed for pain and balance before and after the intervention. The DNG was treated with a specific dry needling protocol (10–15 min), while the CG was re-measured after 15 min and was not subjected to any kind of intervention.
Pain evaluation
The level of pressure pain threshold (PPT) was recorded with an algometer device (FDN100, Wagner Instruments, USA) in kg/cm
Pressure pain threshold measurements were taken from the spinous processes of L2, L3, L4, L5, S1 and also bilaterally one and a half fingerbreadth lateral of the paravertebra muscles at the same level. Measurements were also bilaterally made on posterior superior iliac spines. Data of algometer values were obtained before and after the intervention. All PPT measurements were performed by the same examiner.
Balance evaluation
Kapa-Delta force plates (Kapa-Invent, France) (Fig. 1) were used to register postural behavior of the participants in the following tasks.
Kapa-Delta force plates.
Patients stood over the force platforms, putting each foot on a platform. They were asked to maintain a normal upright stance position for 5 sec. The mean percentage of body weight distribution at each foot was recorded. The absolute difference from 50% regardless of direction (left or right) was used for further analysis.
Lateral loading
Patients were asked to perform a maximum lateral weight shift in each foot while maintaining their other foot on the force plate. The weight loading distribution between their feet as a percentage of their body weight was recorded.
Mediolateral body sway
Patients were asked to perform consecutive weight transfers from one leg to the other in the mediolateral direction lasting 30 sec, while keeping each foot on a force plate. The ability to transfer weight (mean maximum vertical force) at each foot and the power spectrum of the force trajectories of each foot were calculated. From the power spectrums the percentage of the signal in the dominant frequency was calculated to imprint the structure of the signal. The acquisition frequency of the force platforms was set at 200 Hz. Force signals were smoothed with a second order low pass Butterworth filter with 7 Hz cut-off frequency.
Dry needling protocol
After balance and pain baseline measurements, DNG received dry needling by a trained physiatrist. The technique included insertion of a sterile disposable, solid filament needle (Energy Havian Monash Electronic EURL) (needles with tube) at lumbar paravertebra muscles in the relevant spinous process at segments L2, L3, L4, L5 bilateraly. Eight needles were inserted 2 cm lateral to the spinous processes perpendicular to the lamina [25]. A third line of four needles was inserted in the interspinous space of every segment from L1-2, L2-3, L3-4 and L4-5 affecting the supraspinous and interspinous ligaments. No needle was inserted on L5-S1. The deep insertion technique was used, which affects the skin, muscle fascia, ligaments and muscles [26, 27]. Each needle was individually packed. Inserting a needle to the paravertebral spot leads to insertion into multifundus and all the paravertebral muscles, erectorspinae and iliocostalislumborum as well as the thoracolumbar fascia [22]. The size of the needles was 0.30
Data analysis
All analyses were conducted in Matlab (Mathsoft, Natick, MA, USA). A preliminary analysis (chi-square test) was conducted for the anthropometric characteristics of the groups, separately for men and women. The anthropometric characteristics did not differ between groups. As a next step a normal sample distribution was verified for each variable. Correlation analysis between NPS and algometer values during the initial pain evaluation was used to assess the resemblance of the two methods. A repeated, within subjects, two-way ANOVA (2 groups
Force evolution of a representative participant of each group (left foot – right foot).
Pain evaluation
Pain threshold algometer measurements are listed in Table 1. A significant group x measure interaction was noted F (
Descriptive statistics of pain evaluation. Correlation analysis between NPS and algometer initial values showed a significant negative correlation (
0.511
0.05)
Descriptive statistics of pain evaluation. Correlation analysis between NPS and algometer initial values showed a significant negative correlation (
There were no differences between or within groups for both bipedal stance and lateral loading.
Percentage of the signal under the dominant frequency from a representative participant of each group.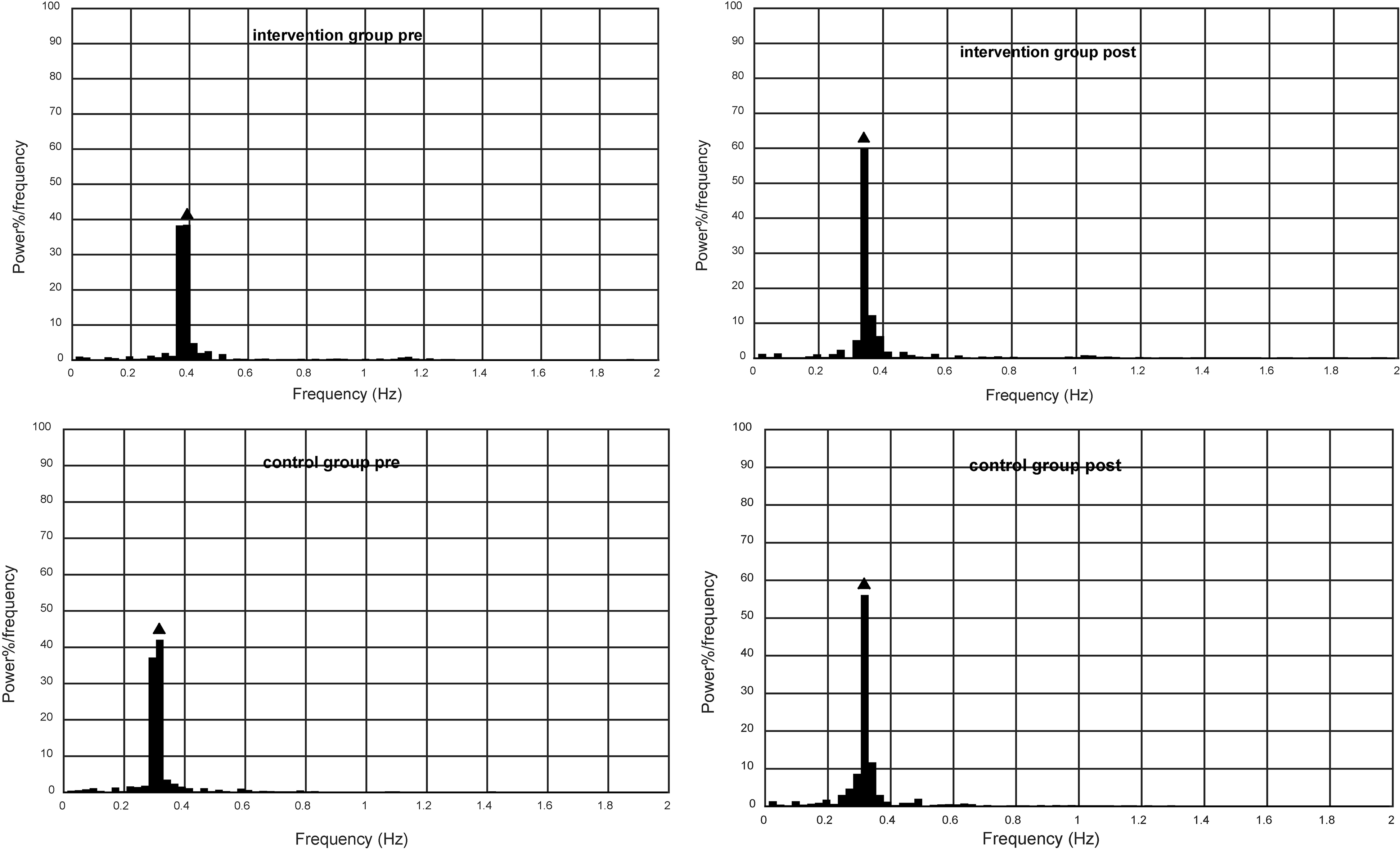
The evolution of force signal for one participant of each group is presented in Fig. 2. The percentage of the signal underneath the dominant frequency is given in Fig. 3. The analysis revealed a significant group
Discussion
Dry needling intervention increased pressure tolerance at the area of pain in the present study. Healthy individuals had higher PPT values than patients with sub-chronic LBP on the same areas [29]. An increase in the PPT after needling was also found in other research [30, 31]. Furthermore, the effect of DN on back muscles in healthy individuals has shown an improvement of back muscle function, implicating that DN stimulates motor nerves and facilitates muscle activity [32]. In a study applying lidocaine injections into paravertebral muscles, an immediate analgesic effect was shown on the muscles, suggesting that the intervention reduces central sensitization [33]. These results may be linked to the release of myofascial trigger points (TrPs) and hence the improved ability for lateral bending. Although there is little evidence that direct deep needling on TrPs has an overall treatment effect when compared with standardized care [34], the method is generally performed in areas of muscles with TrPs in an attempt to reduce muscle tension, restore muscle function and relieve pain [26].
However, in the present study patients were selected depending on the location of pain and not on the presence of TrPs. The improvement in PPT might suggest the presence of TrPs in this area but it is not clear what muscles should be considered for this purpose. Deep needling is chosen since it is found to have better results on pain [35]. As chronic muscle spasms can affect ligaments [36], it is possible that DN affected the ligaments in the present study as well. However, this cannot be proved. Nevertheless since no other intervention has been used, the decrease of the patients’ PPT is probably due to the effect of DN [37]. The point of needling was at the area of multifidus but in the same area there are also longissimus lumborum, erector spinae, rotators longus and brevis. The thoracolumbar fascia, which might be related with pain and mobility, is also located in this area.
Dry needling improved the quality of the muscle function of the patients at the mediolateral level, at least during the dynamic balance task. The manner in which patients perform the oscillation of their weight after needling signifies that the influence of pain is decreased and more harmonic movement is performed. Although it was not measured in the present study, an improvement of the range of motion of the spine due to the relaxation of the muscles as well as an improvement of pain that allows a more comfortable movement is reported in the literature [38]. Also, muscle dysfunction is associated with LBP [39]. Hence, it is reasonable for the muscles that work to control adjustments in position, contraction or relaxation to be better tuned at a lower level of perceived pain. The present finding is related with previous research [40] where LBP patients exhibited less tight and more variable coordination in the frontal plane compared to control participants. Hence, at lower levels of pain agonist and antagonist muscles may be better coordinated, at least this could be implied from the results of the specific dynamic balance task.
On the other hand the discrete ability of the patients to shift their weight laterally to one foot while maintaining contact with their other foot did not change. Since there was no observed asymmetry during bipedal stance as well as pre- and post-treatment, both results verify that there was no deficit in the limb loading of the patients. This could be related to the fact that the pain was sub-chronic and the patients may have not yet evolved strongly established compensation strategies.
It is expected that the ‘release’ of lumbar muscles would benefit the sensorimotor system. Although DN may benefit the muscles and give a ‘window’ to the motor system for testing, training and establishing new motor patterns, the present study did not examine this perspective. Thus, the limited changes in the mechanical behavior could imply the need to provide time for the patient’s sensorimotor system to train and adapt. Despite the fact that the patient’s movements on the mediolateral plane seem to have been ‘released’, further research is needed to establish the effect of pain on creating new movement patterns, considering the long term effects of dry needling, especially in relation to the facilitation it may offer for re-training the system [41].
The present study was limited in the assessment of balance considering only the center of pressure and the ground reaction force, but not the trunk movement. The study design focused on sub-chronic LBP and the acute effect of DN. Hence, considering these limitations and the need of the patients to improve their daily living, future research should focus on long term effects of dry needling in specific tasks of daily living using more holistic methods that will also consider kinematic information.
Footnotes
Conflict of interest
The authors do not have any conflict of interest to report.