
Abstract
BACKGROUND:
The STarT Back Screening Tool (SBT) is a multidimensional questionnaire consisting of physical and psychological factors which categorizes the patients in the low, medium or high risk subgroups.
OBJECTIVE:
To investigate the relationship between SBT-based subgrouping and clustering of patients with LBP using uni-dimensional psychological, clinical and physical examination measures.
METHODS:
One hundred and fifty-seven patients with chronic LBP completed the SBT and uni-dimensional psychological, disability and pain questionnaires. Physical impairments were evaluated through the Physical Impairment Index (PII). Hierarchical and K-means methods were used for cluster analysis. Between-clusters differences and the association between the clusters and SBT-based subgrouping were investigated.
RESULTS:
Three clusters were identified. The derived clusters were labeled severe, moderate and mild physical-psychological-distress clusters, because pain intensity, disability, psychological and physical factors were relatively high, moderate or low, respectively. Most of the patients in moderate and mild physical-psychological distress clusters were categorized as medium risk based on SBT. The mean difference for the PII was higher than that of psychological factors between moderate and mild physical-psychological-distress clusters.
CONCLUSIONS:
Patients in low and high risk subgroups of SBT were sufficiently differentiated, but patients in a medium risk subgroup had a different profile based on PII. Including additional physical factors in the SBT may be required to better differentiate among patients.
Introduction
Low back pain (LBP) is one of the most prevalent musculoskeletal disorders and is strongly associated with disability, low quality of life, emotional stress and absenteeism [1, 2, 3]. Most LBP episodes resolve quickly, but about 50–75% of the cases become chronic [4, 5]. There is an increasing acceptance that psychosocial factors play a crucial role in a transition from acute to a chronic LBP [6]. Early screening of psychological factors is proposed for improving the quality of care by identifying patients who are at risk of developing chronic LBP [7, 8, 9, 10, 11]. There are two types of psychological screening tools; uni-dimensional and multidimensional questionnaires [12, 13]. While uni-dimensional questionnaires include several items that are all related to one psychological factor, multidimensional questionnaires include several items that are related to one specific psychological factor [14]. The STarT Back Screening Tool (SBT) is a multi-dimensional questionnaire which includes some physical factors in addition to psychological factors [15]. Based on SBT, patients are categorized to be at a low, medium, or high risk of developing chronic LBP [15]. Psychometric properties of SBT were evaluated and confirmed in several studies [1, 2, 12, 14, 16, 17, 18, 19, 20, 21, 22]. Previous studies used uni-dimensional psychological and disability questionnaires as reference standards to validate the SBT [1, 12, 13, 15, 19]. For instance, Beneciuk et al. clustered the patients based on uni-dimensional psychological and disability questionnaires, and found 2 subgroups of patients with high and low intensity of clinical and psychological profile [12]. Based on this finding, Beneciuk et al. concluded that SBT cutoff scores in a physical therapy setting may need to be reevaluated [12].
Physical impairment measures are described as an important part of clinical examination in patients with LBP [23] and there are valid and reliable assessment tools for physical examination of patients with LBP, e.g. the Physical Impairment Index (PII) [24, 25]. Studies revealed an association between physical impairments, psychological factors, and disability in chronic LBP [26, 27, 28]. However, physical examination measures were not included in the SBT development [15], and there is no study that investigated the relationship between SBT-based subgrouping and physical impairment measures. Therefore, the primary purpose of the current study was to evaluate the relationship between SBT-based categorization and physical examination measures. The second purpose was to evaluate the association between SBT-based subgrouping of patients with LBP and clustering using PII, clinical and psychological measurement tools. We assumed that adding physical impairment examination to the cluster analysis, in addition to a uni-dimensional psychological and disability questionnaires used in the study by Beneciuk et al. [12], may result in a more accurate clustering of patients with LBP. The results of this study can be used by physiotherapists for better screening of patients with LBP.
Methods
This was an analytic cross-sectional study. Data was collected between November 2016 and January 2018 from four private and three educational outpatient Physical Therapy (PT) clinics of the university, located in Ahvaz city.
Participants
Patients diagnosed with chronic LBP, referred by specialized physicians to PTs, participated in the study. Chronic LBP is defined as back pain symptoms from the 12
Patients’ demographic, clinical, psychological measures and PII mean (sd)
Patients’ demographic, clinical, psychological measures and PII mean (sd)
SD, Standard Deviation; BSc, Bachelor of Science; SBT, STarT Back Screening Tool; NPRS, Numerical Pain Rating Scale; RMDQ, Roland-Maoris Disability Questionnaire; ODI, Oswestry Disability Index; TSK, Tampa Scale of Kinesiophobia; BDI, Beck Depression Inventory; PCS, Pain Catastrophizing Scale; FABQ-PA, Fear Avoidance Beliefs Questionnaire-Physical Activity subscale; FABQ-W, Fear Avoidance Beliefs Questionnaire-Work subscale; PII, Physical Impairment Index.
All data were collected by an 8-years experienced physiotherapist. Participant’s age, gender, height (m), weight (kg) and level of education were recorded. LBP history, including previous surgery, symptoms onset and duration, and previous treatments were also recorded. Various questionnaires, including SBT and uni-dimensional psychological questionnaires, were completed by the participants. Uni-dimensional psychological questionnaires including the Tampa Scale of Kinesiophobia (TSK), the Beck Depression Inventory (BDI), Pain Catastrophizing Scale (PCS), Fear Avoidance Beliefs Questionnaire-Physical Activity subscale (FABQ-PA), and Fear Avoidance Beliefs Questionnaire-Work subscale (FABQ-W) were used for evaluation of psychological factors [29, 30, 31, 32, 33, 34]. Clinical measures, including pain severity and disability were also evaluated. An 11-point Numerical Pain Rating Scale (NPRS) was used to evaluate pain severity. The subject’s present, minimal and maximal pain severity during the last 24 hours was recorded, and the mean of these three scores was considered as the pain severity [1, 12]. Two questionnaires were used for disability evaluation; the Oswestry Disability Index (ODI) and the Roland-Maoris Disability Questionnaire (RMDQ) [35]. The validity and reliability of the Persian version of the used questionnaires were previously reported [1, 2, 29, 30, 34, 35, 36]. Objective evaluation of LBP related physical impairments was performed through PII [24, 25, 26]. This index is a valid and reliable index, which consists of seven movement impairment tests for pain, range of motion, and strength assessment [25].
Between-group differences for physical-psychological clusters in demographic, clinical, physical and uni-dimensional psychological measures
Between-group differences for physical-psychological clusters in demographic, clinical, physical and uni-dimensional psychological measures
SD, Standard Deviation; NPRS, Numerical Pain Rating Scale; RMDQ, Roland-Maoris Disability Questionnaire; ODI, Oswestry Disability Index; TSK, Tampa Scale of Kinesiophobia; BDI, Beck Depression Inventory; PCS, Pain Catastrophizing Scale; FABQ-PA, Fear Avoidance Beliefs Questionnaire-Physical Activity subscale; FABQ-W, Fear Avoidance Beliefs Questionnaire-Work subscale; PII, Physical Impairment Index. **
All data analyses were performed using SPSS (version 16). Descriptive statistics were calculated for demographic, psychological and clinical measures. Differences between the SBT subgroups for the variables of interest were evaluated using an Analysis of Variances (ANOVA). Raw scores for TSK, BDI, PCS, FABQ-PA, FABQ-W, ODI and PII were transformed to Z-scores for cluster analyses; however, raw scores are reported for descriptive purposes [12, 37]. Cluster analysis was utilized to investigate whether there are distinct subgroups within the sample based on physical and psychological factors. First an exploratory hierarchical agglomerative cluster analysis with Ward’s method and squared Euclidean distances as the similarity measures was performed [12, 37, 38, 39, 40]. The optimal number of cluster solutions was determined using the dendrogram inspection, and the K-means cluster analysis (elbow method). K-means clustering was performed in 2–10 cluster solutions, and then a percentage of between group’s variances was plotted against the number of solutions. The elbow method looks at the percentage of variance explained as a function of the number of clusters; one should choose a number of clusters so that adding another cluster does not increase the percentage of variance extremely [40]. Cluster differences in demographics, clinical and psychological measures were evaluated through ANOVA. A 3
Results
During the data collection, 369 patients with LBP were referred to the examiner. 68 were excluded due to acute symptoms, and 144 were excluded because their age was above 65 (
Visual inspection of the dendrogram and the elbow method indicated that 3 cluster solutions are optimal. The differences of demographic, clinical, and psychological measures between the clusters are summarized in Table 2. The 3 identified clusters were labeled based on their characteristics. As the level of NPRS, TSK, BDI, FABQ, PCS, ODI and PII measures were relatively high, moderate and low in cluster 1 (
The results of the Pairwise comparisons of the clusters for NPRS, RMDQ, ODI, TSK, BDI, PCS, FABQ-PA, FABQ-W, and PII are summarized in Table 3.
Pairwise comparison of severe, moderate, and mild physical-psychological distress clusters
Pairwise comparison of severe, moderate, and mild physical-psychological distress clusters
CI, Confidence Interval; NPRS, Numerical Pain Rating Scale; RMDQ, Roland-Maoris Disability Questionnaire; ODI, Oswestry Disability Index; TSK, Tampa Scale of Kinesiophobia; BDI, Beck Depression Inventory; PCS, Pain Catastrophizing Scale; FABQ-PA, Fear Avoidance Beliefs Questionnaire-Physical Activity subscale; FABQ-W, Fear Avoidance Beliefs Questionnaire-Work subscale; PII, Physical Impairment Index.
Based on the SBT score, 36% of the patients in the severe physical-psychological distress cluster, 81% of the patients in moderate physical-psychological distress cluster, and 71% of the patients in mild physical-psychological distress cluster were categorized as medium risk (MR). The percentage of high risk (HR) patients in severe, moderate, and mild physical-psychological distress clusters were 63%, 14%, and 0%, and low risk (LR) patients with severe, moderate, and mild physical-psychological distress clusters were 0%, 3% and 29%, respectively (Fig. 1) (
Distribution of SBT-based subgroups by mild, moderate and severe physical-psychological distress.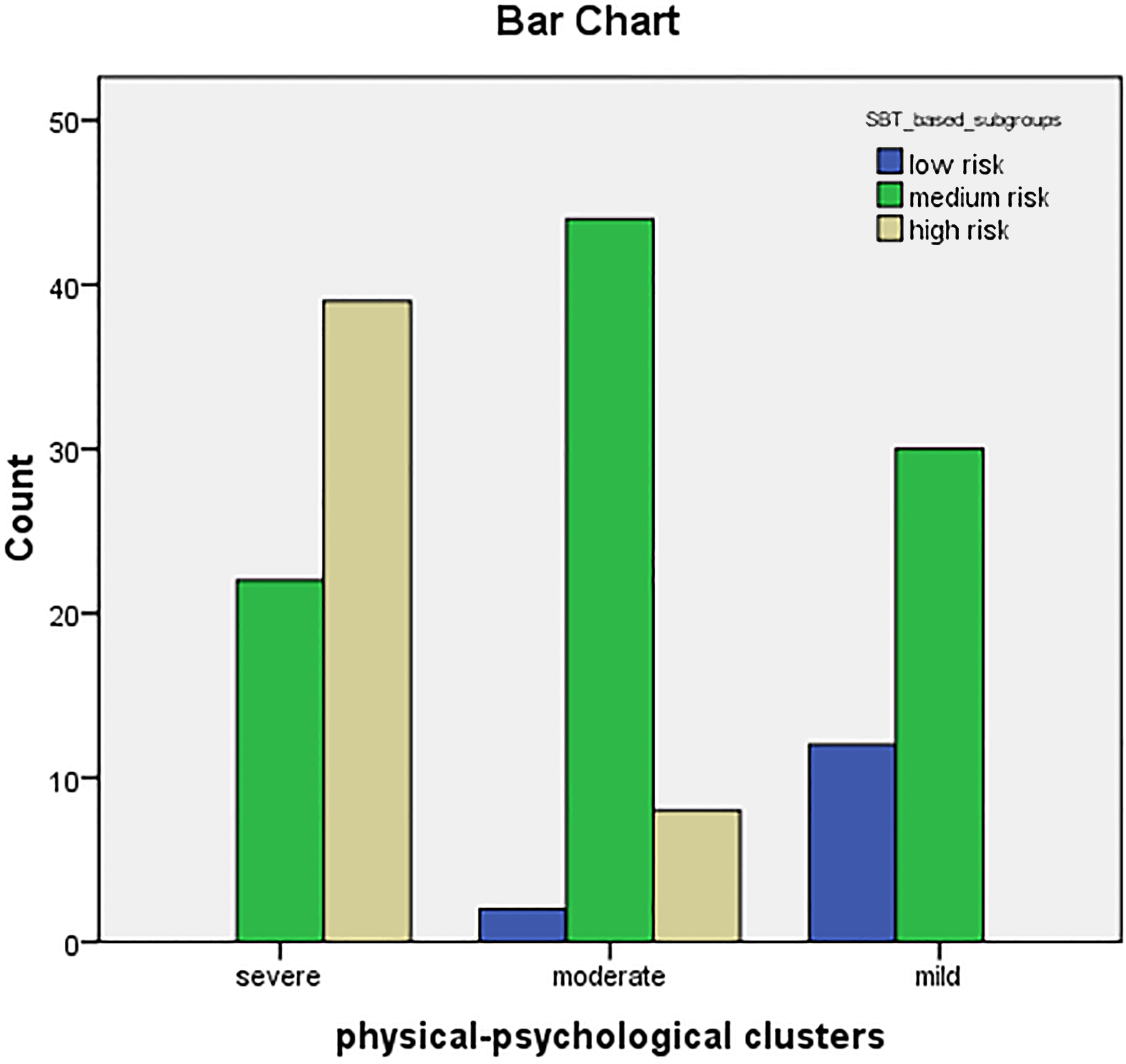
The aim of our study was to evaluate the relationship between the SBT-based categorization and physical examination measures and to make a comparison between the clustering of patients with LBP based on uni-dimensional psychological, physical and clinical assessment tools to SBT-based subgrouping in physical therapy settings. Our findings showed that MR patients based on the SBT classification might be categorized in different subgroups when clustered based on uni-dimensional psychological, clinical and physical factors.
Based on SBT most of the patients in our sample were categorized as MR (above 60%), only 9% as LR, and 30% as HR subgroups (Table 1). SBT risk-dependent relationship (LR
In our study, cluster analysis using uni-dimensional questionnaires identified 3 clusters. This is consistent with the results of Beneciuk et al. who found 3 clusters in patients with acute or sub-acute LBP [37] and inconsistent with the results of another study by the same group in which 2 clusters of patients with chronic LBP have been identified [12]. These conflicts regarding the number of clusters in patients with LBP may be due to the difference in the studied populations or the variables that were used for cluster analysis.
A high proportion of the patients in moderate and mild physical-psychological distress clusters were categorized as MR (approximately 81% and 71%, respectively) and in severe physical-psychological distress cluster as HR (63%) based on SBT classification. Despite significant differences in almost all uni-dimensional psychological, clinical and physical factors, the mean difference of the physical factors, i.e. PII, was relatively higher than those of the psychological measures (TSK, BDI, FABQ, and PCS) when comparing moderate and mild physical-psychological distress clusters. These findings suggest that patients who are categorized as MR, based on SBT subgrouping, may show a different profile when including physical factors in cluster analysis. It may reveal that the prognostic factors included in SBT cannot sufficiently differentiate among patients with chronic LBP at physical therapy settings and including additional physical factors in the SBT questionnaire may results in better differentiating. This may be due to the fact that SBT was initially developed for a primary care clinic setting and its application by physical therapists may require some modification. Including some additional physical construct in the SBT may be required.
In general, the patients who are categorized as LR based on SBT were minimal in each physical-psychological cluster. This may be due to the unequal distribution of the patients in the 3 SBT-based subgroups in our sample.
Some limitations of our study should be considered. First, in cluster analysis, each uni-dimensional questionnaire and the PII were considered as one score, although they consist of several items. Previous research revealed that considering each item of the questionnaires as a single item resulted in more distinguishing characteristics [42]. We suggest that future research considers each item of the assessment tools as a single item. The other limitation was related to the objective nature of the dendrogram and elbow method. Other types of cluster analysis, i.e., a two-step cluster analysis, which determines the number of clusters automatically, with a larger sample of patients can be used in future studies [43].
Conclusion
The results of our study indicate that SBT-based subgrouping of patients with LBP into 3 clusters is consistent with clustering based on psychological and physical factors. However, it seems that adding physical factors to the cluster analysis may differentiate among the patients in the MR subgroup based on SBT categorization. Further studies are required to evaluate this finding in populations with an equal number of patients in the 3 SBT-based subgroups.
Footnotes
Acknowledgments
This study is part of the PhD thesis of Nava Yadollahpour. Special thanks to Ahvaz Jundishapur University of Medical Sciences for the financial support of the research project.
Conflict of interest
None of the authors have any financial or other interests relating to the manuscript to be submitted for publication in the Journal.