
Abstract
BACKGROUND:
Illness perceptions predict chronic low back pain (CLBP) disability. This study cross-culturally adapted and validated the Igbo Brief Illness Perceptions Questionnaire (Igbo-BIPQ) in people with CLBP in rural/urban Nigeria.
METHODS:
A cross-cultural adaptation and validation of the Igbo-BIPQ was undertaken. The BIPQ was forward/back-translated by clinical/non-clinical translators. An expert review committee appraised the translations. The questionnaire was pre-tested on twelve rural Nigerian dwellers with CLBP. Internal consistency using Cronbach’s alpha; test-retest reliability using intra-class correlation coefficient and Bland-Altman plot; and minimal detectable change were investigated amongst 50 people with CLBP in rural and urban Nigeria. Construct validity was determined by correlating the Igbo-BIPQ score with those of eleven-point box scale and Igbo Roland Morris Disability Questionnaire (Igbo-RMDQ) using Pearson’s correlation analyses in 200 adults with CLBP in rural Nigeria. Ceiling and floor effects were investigated in both samples.
RESULTS:
Good face/content validity, internal consistency (
CONCLUSION:
This study provides evidence of some aspects of validity and reliability of the Igbo-BIPQ.
Introduction
Illness perceptions are the personal ideas and beliefs people have about a sickness [1]. Patients’ beliefs such as the meaning of symptoms, ability to control pain, the impact of pain on patients’ lives, and worry about the future are believed to play a crucial role in chronic pain because they influence psychological and physical functioning. These beliefs and perceptions are posited to usually influence CLBP coping strategies which impact on clinical outcomes as explained in the Leventhal’s self-regulatory model of illness cognitions. This model proposes that symptoms and social messages generate cognitive and emotional representations of a potential illness through three stages of interpretation, coping and appraisal [2]. According to this model, illness perceptions include the following dimensions: perceived illness identity (individual’s understanding and label of the illness and the associated symptoms), perceived causes (personal beliefs about the causes of the illness), perceived consequences (individual’s beliefs about the outcomes and effects of the condition on their life). Others include perceived timeline (how long the individual believes the illness will last) and perceived illness controllability (the extent to which the individual believes they can control or recover from the illness) [2]. Patients’ beliefs such as the meaning of symptoms, ability to control pain, the impact of pain on patients’ lives, and worry about the future are believed to play a crucial role in chronic pain because they influence psychological and physical functioning. For instance, illness perceptions are posited to influence chronic low back pain (CLBP) coping strategies which impact on clinical outcomes [2].
A comprehensive review of studies conducted in high income countries found strong evidence to support the role of pain perceptions, in addition to depression, fear avoidance beliefs and catastrophising in the maintenance of pain and disability among individuals with CLBP [3]. A meta-analysis of cross-sectional studies that investigated the influence of illness perceptions in physical health conditions in high income countries found that illness perceptions explained between 25% and 30% of the variance in emotional health outcomes [4]. Perceptions of illness consequences and emotional representations had the strongest relationship with emotional health outcomes. Another systematic review of general health conditions including musculoskeletal conditions, confirms the predictive power of illness perceptions on depression, anxiety and quality of life [1]. However, this review did not assess test-retest reliability, and the coherence item predicted the fewest outcomes (least predictive validity).
No systematic review exists that examines the role of illness perceptions on pain persistence and CLBP disability. Several prospective cohort studies in high income countries have shown that illness perceptions influence clinical outcomes following CLBP treatment [5, 6]. Of twenty psychological factors related to CLBP recovery, illness perceptions and pain self-efficacy were the most predictive of disability in patients treated for low back pain in UK primary care, above fear avoidance beliefs, catastrophising and depression [5]. A prospective cohort study of primary care patients with CLBP in the UK found that reductions in perceived consequences, emotional representations and illness identity (number of symptoms patients felt were related to their back pain) and increases in treatment and personal control were the specific back pain perceptions associated with reduced CLBP disability [6]. Improvements in illness coherence and timeline (acute or chronic) were found in the CLBP patients that reported improvements in global rating of change [6]. Two randomised controlled trials in the Netherlands and Norway respectively, found that interventions targeting illness perceptions improved functioning, and reduced maladaptive illness perceptions such as perceived consequences of CLBP [7, 8]. The relationship between pain and emotional dysfunction is known to be mediated by representations of pain as a highly emotive experience (emotional representations), and by catastrophising [9]. In contrast, the relationship between pain and physical dysfunction has been shown to be mediated by representations of the high consequences of chronic pain (consequences), but not by catastrophising [9].
Limited studies have investigated the impact of illness perceptions on CLBP in rural Africa, probably due to lack of measures for non-English speaking populations. One of such is a qualitative study in rural Nigeria which suggested that maladaptive back pain perceptions may encourage maladaptive coping strategies such as pain medication dependence including opioids and cure seeking which increase disability and emotional distress in people living with chronic LBP [10]. Another study, a population-based cross-sectional study among people living with CLBP in rural Nigeria found that illness perceptions were the strongest predictors of both self-reported and performance-based disability, above pain intensity, occupational biomechanical factors, catastrophizing, fear avoidance beliefs and anxiety [11]. Furthermore, a novel community-based self-management programme that targeted maladaptive illness perceptions associated with CLBP disability in a rural Nigerian community showed promising outcomes in reducing disability, pain intensity and pain medication use [12]. The Brief Illness Perceptions Questionnaire (BIPQ) was found useful in that study.
The BIPQ is a valid and reliable measure of illness perceptions; measures cognitive and emotional representations; and is the shortest of all the available illness perception questionnaires [13]. Its brevity implies potential usefulness for studies incorporating several other outcome measures and in busy clinical settings. Pooled evidence of 188 studies of varied health conditions demonstrated that the BIPQ has good concurrent, predictive and discriminant validity, and sensitivity to change at item and scale level [1]. The health conditions were cancer; endocrine, nutritional and metabolic diseases; mental and behavioural disorders; diseases of the nervous system; eye diseases; diseases of the circulatory system; respiratory diseases; diseases of the digestive system; skin diseases; diseases of the musculoskeletal system and connective tissue; diseases of the genitourinary system; infectious diseases; accidents, injuries and burns; organ transplantation; and allergies and sensitivities [1]. The languages the BIPQ has been adapted to include Chinese, Croatian, Czechoslovakian, Danish, Dutch, French, German, Greek, Gujurati, Hebrew, Hindi, Indonesian, Italian, Japanese, Kannada, Norwegian, Persian-Farsi, Polish, Portuguese, Samoan, Slovene, Spanish, Telegu, Tongan and Urdu [1]. However, the BIPQ and other measures of illness perceptions have never been adapted for use in Nigeria. In view of the importance of illness perceptions in influencing CLBP outcomes in rural Nigeria, and the utility of the BIPQ, this study aimed to cross-culturally adapt the BIPQ into Igbo and investigate its psychometric properties in rural and urban Nigerian populations.
Method
Study designs
Cross-cultural adaptation, test-retest measurements and cross-sectional study of psychometric properties of the Igbo-BIPQ were conducted.
Ethical considerations
Ethical approval was obtained from King’s College London (No. BDM/13/14-99) and University of Nigeria Teaching Hospital (No. UNTH/CSA/329/Vol.5). Written permission was obtained from the original developers of the measure. Informed consent was sought and obtained from all the participants involved in this study.
Outcome measures
Brief Illness Perceptions Questionnaire (BIPQ)
The BIPQ is a nine-item self-report measure of illness perceptions [13]. Each item, measured on a Likert scale ranging from 0 to 10, assesses one dimension of illness perceptions. Eight items (consequences, timeline, personal control, treatment control, identity, illness concern, coherence and emotional representation), comprising cognitive and emotional illness perceptions, may be combined as one total score, or each item may be assessed separately to give eight dimensions of illness perceptions [13]. Each item is measured on an incremental ten-point scale, anchored at 0 and 10 depicting minimal and maximal level of the assessed dimension respectively. The total score requires that items 3, 4, and 7 are reverse scored and then added to items 1, 2, 5, 6, and 8. The maximum total BIPQ score is 80 and the minimum total score is 0 with a higher score reflecting a more threatening view of an illness [13]. The ninth item is the causal item which is open, and can be analysed by grouping participants’ responses into relevant categories depending on the research question [13]. Using the total score of the BIPQ was shown to have better validity and reliability than scoring at the item level in a cross-sectional study of patients with sub-acute and chronic LBP [14]. However, a meta-analysis of 188 studies of diverse health conditions demonstrated good concurrent, predictive and discriminant validity, and sensitivity to change at both the item and scale level [1]. Item-level test-retest reliability of the original BIPQ ranged between 0.42–0.75 [13].
Eleven-point box scale (BS-11)
The BS-11 is a single eleven-point numeric scale for pain intensity [15]. It consists of eleven numbers (0 through 10) surrounded by boxes. Zero represents ‘no pain’ and 10 represents ‘pain as bad as you can imagine’ or ‘worst pain imaginable’. It was chosen for this paper due to its easy comprehensibility and ease of administration. It is probably the measure of choice for research involving illiterate people in rural Nigeria as it was shown that the simple VAS was not easily understood in this population [10]. The BS-11 has high test-retest reliability in both literate and illiterate patients with rheumatoid arthritis (ICC
Igbo Roland Morris Disability Questionnaire (Igbo-RMDQ)
The RMDQ [16] is the most commonly used valid measure of LBP disability. RMDQ conceptualises disability at the three levels of the ICF: body structures and function, activities and participation, and environmental factors, although with less emphasis on participation, and no work-related outcomes. It is recommended as a core outcome measure for the standardisation of outcome measurement in LBP clinical trials, meta-analyses, cost-effectiveness analyses and multi-centre studies [17]. The RMDQ is simple to administer, easily understood, and is the best measure for population or primary care-based studies [18].
The Igbo-RMDQ [19] was adapted from the original English RMDQ [16], a 24-item back specific self-report measure with each item having possible scores of 0 or 1. A total maximum score of 24 signifies the highest possible disability level and 0 means that there is no disability. The Igbo-RMDQ has good face and content validity, construct validity (moderately high correlations [
Cross-cultural adaptation
Participants
Translators included one clinical musculoskeletal physiotherapist with 12 years of experience practising in Nigeria (native Igbo speaker but bilingual in English and Igbo); and three non-clinical translators. The non-clinical translators comprised two native English speakers and one native Igbo speaker who were bilingual in English and Igbo. Two of the non-clinical translators (one native English speaker and one native Igbo speaker were linguistic experts who were professional translators experienced in patient reported outcomes. The expert review committee included two English experts (health psychologist and academic physiotherapist) in the United Kingdom, and two Igbo experts (clinical psychologist and clinical physiotherapist) in Nigeria. All four translators and the external expert review committee members met on several occasions during the cross-cultural adaptation process.
Pre-testing/piloting of the adapted measure was done with a convenience sample of 12 adults who had participated in a different study [10]. They were from Akegbugwu, a rural agrarian population in Enugu State.
All participants were invited to participate in this study via telephone, but data were collected face-to-face. They were informed about the study, and those who wished to participate were then recruited. Informed consent was subsequently obtained. Their CLBP was not due to malignancy, spinal fracture, infection, inflammation, or cauda equina syndrome.
Procedure
The original BIPQ [13] was cross-culturally adapted following evidence-based guidelines for cross-cultural adaptation of patient-reported outcome measures [20, 21] (Fig. 1).
Steps used in cross-cultural adaptation.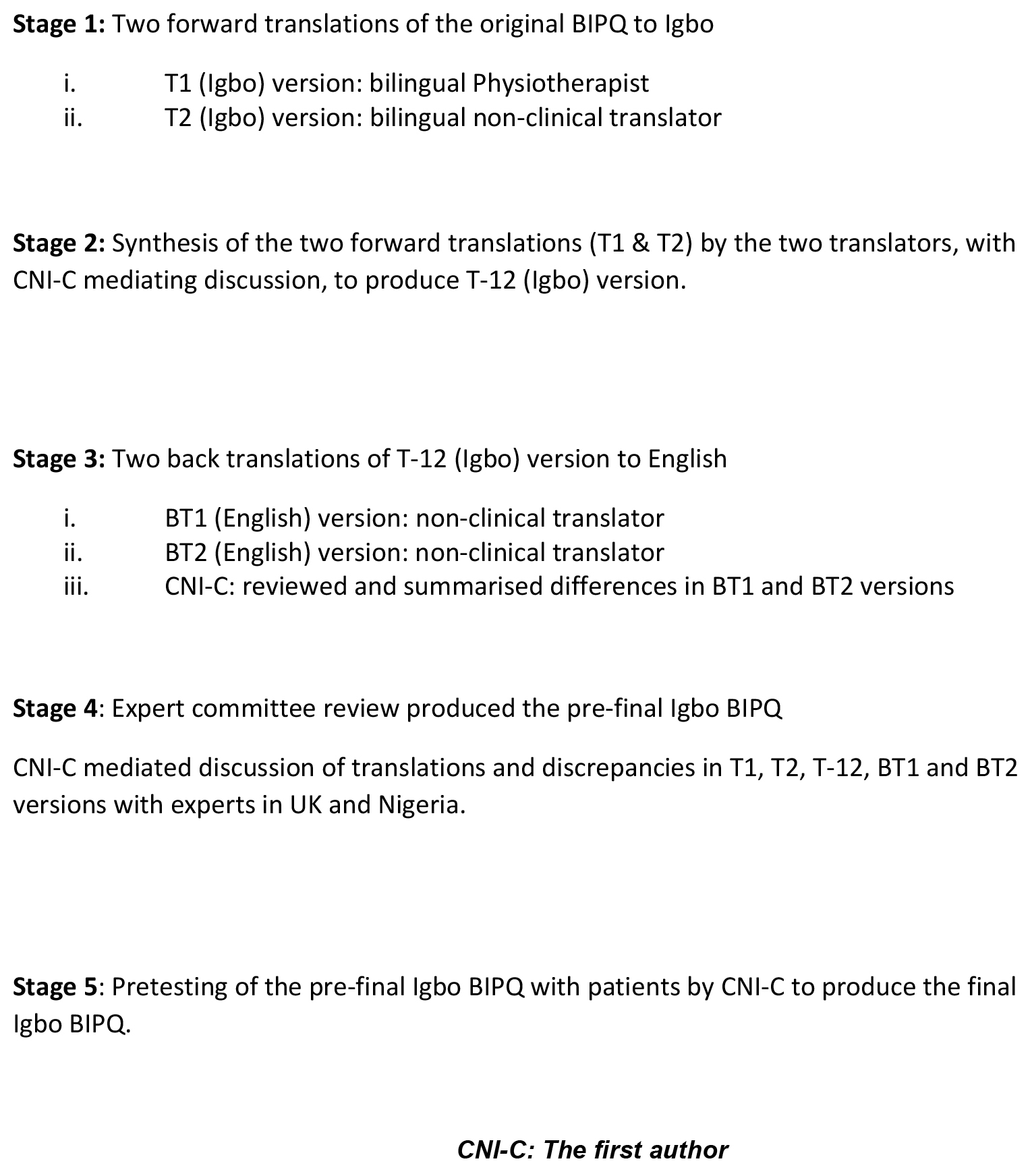
Firstly, the BIPQ was forward translated from English to Igbo by one bilingual clinical musculoskeletal physiotherapist and one bilingual non-clinical professional translator (both were native Igbo speakers, bilingual in Igbo and English). Item definitions were provided for the clinical translator to ensure familiarity with the assessed construct and provide greater psychometric equivalence with the original RMDQ. Item definitions were not provided for the non-clinical translator to ensure that the translation reflected the language used by lay people in Igbo culture. This produced two Igbo versions: T1 and T2 respectively.
Secondly, T1 and T2 were synthesized via discussion between the two forward translators, mediated by the first author who is bilingual in English and Igbo. This produced one Igbo BIPQ version: T-12. Translations were compared and discrepancies were noted.
Thirdly, the Igbo (T-12) BIPQ version was back translated from Igbo to English by two back translators who were native English speakers from non-clinical backgrounds and blinded to the original measure. One of the back translators was an Igbo/English linguistic expert/professional translator.
This produced two back-translated English versions: BT1 and BT2. This was a validation process ensuring that translation was consistent, and that the translated version of the BIPQ (T-12) was reflecting the meaning in the original measure.
Fourthly, T1, T2, T-12, BT1 and BT2 versions were discussed by the external expert review committee together with the four translators to produce the pre-final Igbo-BIPQ.
The main purpose of this committee was to achieve cross-cultural equivalence in terms of semantic, idiomatic, experiential and conceptual equivalence [20]. For semantic equivalence, the expert committee explored Igbo and English words to assess if they meant the same thing, if there were multiple meanings to an item, and if there were any grammatical difficulties in the translations. Idiomatic equivalence was assured by the committee formulating alternative Igbo idioms/colloquialisms, where English versions were difficult to translate. Experiential equivalence was achieved by the committee ensuring that questionnaire items were experienced similarly in English and Igbo cultures. For conceptual equivalence, the committee determined that words in the items, instructions, and response options had similar conceptual meanings in Igbo and English cultures. The expert committee also ensured that Igbo wordings were simple and could be easily understood regardless of age and educational levels.
Finally, the pre-final Igbo BIPQ was field tested in rural Nigeria among the twelve participants as previously stated. The first author interviewer-administered the Igbo BIPQ using the ‘think-aloud’ cognitive interviewing procedure to assess comprehensibility, acceptability of items and cultural equivalence. Each item was read out, and participants were requested to actively verbalise their thoughts as they attempted to answer each question. Participants were asked if they encountered difficulty comprehending the questionnaire, what was understood by each item, the meaning of the chosen response, and if they found any item offensive. They were encouraged to keep talking while their responses were recorded by the first author. Items that were offensive, irrelevant, or unclear were reviewed and modified by the external review committee and the translators at a meeting. This stage ensured that equivalence was maintained in the target setting to produce the final Igbo-BIPQ, confirming face and content validity. Technical equivalence (methods of data collection) was assured through data collection using the same format (interviewer-administration) with all participants.
Clarifications were sought from the original developers of the BIPQ and all linguistic changes made to the measure were discussed with them.
Sample size estimation
Test-retest reliability sample
A minimum sample size of 27 was required per language group to detect an intra-class correlation coefficient of 0.9 and a maximum width of 0.23 for the 95% confidence interval [22]. Hence the test-retest reliability assessment was conducted with a convenience sample of 50 participants with CLBP, between the ages of 18 and 69 years, recruited from rural and urban communities in Enugu State, South-eastern Nigeria. Their chronic low back pain was not due to malignancy, spinal fracture, infection, inflammation, or cauda equina syndrome.
Construct validity assessment sample
Sample size calculation showed that a sample of 194 would give an 80% power to detect a very small correlation coefficient of 0.2 at
Participants were recruited via village announcements facilitated by the traditional heads of the communities. CHWs then screened potential participants by asking all participants the same set of simple questions to rule out the ‘red flags’ for LBP by excluding any back pain associated with underlying serious pathology, radiculopathy or spinal stenosis [23, 24]. Informed consent was subsequently obtained. Included participants were aged 18 to 69 years. Pregnant women were excluded, as chronic LBP due to pregnancy is not regarded as non-specific.
Procedure for psychometric testing
Training community health workers for data collection
CHWs were trained for two weeks, for interviewer-administration of the Igbo-BIPQ, pain scale (BS-11) and the Igbo-RMDQ.
A training manual was developed which was daily, face-to-face and group-based in a classroom at the University of Nigeria Teaching Hospital Enugu, Nigeria. Training was done to minimise coverage, sampling, measurement and non-response errors. Measurement error was reduced by using validated measures and tailoring community health workers’ training to avoid asking questions in ways that could bias participants’ responses or inaccurate objective disability measurements such as guessing measurements rather than using a tape measure. Non-response error was prevented by training the CHWs to assess all recruited participants whilst ensuring that no items or scales were unanswered. Training ended with question and answer sessions and a classroom clinical examination. Examination questions assessed survey rationale, purpose and protocol, and practical administration of outcome measures. The lead author was responsible for the training and examination sessions.
Fidelity results
Fidelity checks carried out in the field by the first author during data collection showed that data collection was per protocol. CHWs adhered to the recommended interviewing styles emphasized during the training. Examples include maintaining neutrality during interview, not reacting by gesture or word, either positively or negatively to any responses; discouragement of digression, distraction and inappropriate enquiries, and not changing the wording and sequence of questions in the measures. Data recording was adequate as this was planned a priori. CHWs provided only one answer to each item, marked in the space provided for each item in each measure.
Data collection procedure
A booklet containing screening and demographic questions, the Igbo-BIPQ, the BS-11, and the Igbo-RMDQ was used by each CHW to collect data. Prior to being assessed and interviewed, participants were requested to describe their pain location with a body chart, and screened (via the simple questions) to confirm non-specific chronic LBP by ruling out back pain due to malignancy, spinal fracture, infection, inflammation or cauda equina syndrome, in line with evidence-based guidelines for diagnosing non-specific LBP. Likert scales were presented to participants as ‘flash cards’ as the corresponding item was read out. Items were made back pain-specific by reading out ‘back pain’ in place of ‘illness’.
To assess test-retest reliability, the Igbo-BIPQ was completed at baseline on August 11, 2014 among the convenience sample of urban and rural Nigerian dwellers. Measurements were repeated seven days after the first measurement among 45 participants. The remaining 5 participants were reassessed after ten days when they were available. The same CHW collected data from each participant on the two occasions.
For validity assessment, the three outcome measures were completed at one time-point in a cross-sectional design on August 22, 2014 among the random sample of 200 rural dwellers.
The two samples were similar in characteristics except that the test-retest sample also included urban dwellers who routinely have higher literacy levels in Nigeria. Importantly, recruiting different samples of rural and urban dwellers enabled a wider applicability of the Igbo-BIPQ in rural and urban Nigeria, as well as across all levels of literacy or illiteracy.
Fidelity assessment
Fidelity checks were done to avoid systematic differences in data collection by the CHWs. Involving workers that passed the post-training examinations facilitated adherence to data collection protocols. Additionally, the first author visited each worker during data collection without prior arrangement, and assessed their interviewing styles, and data recording.
Data analyses
IBM SPSS version 22 was used for data analyses. Data were assessed for normality using visual, and statistical methods. No missing data were recorded.
Reliability
Reliability assesses the ability of an instrument to measure consistently [25]. Test-retest reliability evaluated how consistently the Igbo-BIPQ measured illness perceptions over time, and this was investigated using intra-class correlation coefficient (ICC). ICC was calculated using a two-way random effects model (which assumes that measurement errors could arise from either raters or subjects), using an absolute agreement definition between test-retest scores. 0.7, 0.8 and 0.9 represented good, very good and excellent ICCs [26]. Internal consistency (Cronbach’s alpha), which portrays the extent to which all items in a test measure the same construct, was calculated and was rated as low/weak (0–0.2), moderate (0.3–0.6) and strong (0.7–1.0) [25]. Bland-Altman plots were used to visually assess the level of agreement between test-retest measurements by plotting mean Igbo-BIPQ scores against difference in total Igbo-BIPQ scores, and accounted for the weakness of ICC, which might indicate strong correlations between two measurements with minimal agreement [27].
Reliability was also evaluated using the standard error of measurement (SEM) and minimal detectable change (MDC). MDC is a statistical estimate of the smallest change detected by a measure that corresponds to a noticeable change in ability which is not due to measurement error; and should be sufficiently small to detect minimal clinically important difference [28]. MDC was calculated using the standard error of measurement (SEM) which is based on the distribution method, and the reliability of the measure which takes precision into account [28]. SEM was based on the standard deviation (SD) of the sample and the test-retest reliability (R) of the Igbo-BIPQ, and was calculated with Eq. (1) below [28]:
Equation (1) Standard Error of Measurement.
MDC was subsequently calculated with Eq. (2) below:
Equation (2) Minimal Detectable Change, where 1.96 derives from the 95% confidence interval of no change, and
Construct validity assesses the extent to which an instrument measures the construct it was intended to measure [29]. As there are no “gold standard” Igbo measures for illness perceptions, construct validity of the Igbo-BIPQ was investigated. The domain of construct validity assessed was convergent validity using Pearson’s correlation coefficient (parametric data), and was rated as weak (0–0.2), moderate (0.3–0.6), or strong (0.7–1.0). Convergent validity assesses whether two measures that are assumed to be theoretically related, are in fact related. Due to the lack of any validated Igbo illness perceptions measure, the BS-11, a self-reported one-item numeric pain intensity scale, and the Igbo-RMDQ, a self-reported back pain specific disability measure were used, and the established relationships between illness perceptions, pain intensity and self-reported disability were used for validity assessment underpinned by a priori set hypotheses of assumed relationships from the established literature. Illness perceptions have moderate positive correlations with pain intensity [9], therefore the Igbo-BIPQ is expected to also have at least a moderate correlation with the BS-11. Illness perceptions have been shown to have moderate correlations with self-reported disability measured with the RMDQ [5], therefore the Igbo-BIPQ was expected to also have a moderate correlation with the Igbo-RMDQ.
Floor and ceiling effects
Ceiling or floor effect occurs when a high proportion of participants score the highest or lowest score respectively, implying that a measure is unable to discriminate between participants at either extreme of the scale. A ceiling or floor effect was defined as 15% or more of the total sample of 250 participants scoring 0 or 80 on the Igbo-BIPQ [30].
Results
Cross-cultural adaptation findings
Participants for cross-cultural adaptation
Table 1 shows that seven of the twelve participants were males and manual workers, including farmers, panel beaters and welders. Non-manual workers were civil servants and traders. Ten of the twelve participants were from the Pentecostal Christian religion. Eleven were married. Four had secondary education. Half of them (6) were literate in English only, meaning they could read and write English only.
Demographic characteristics of the participants that pre-tested the measure
Demographic characteristics of the participants that pre-tested the measure
Demographic characteristics of participants for test-retest reliability testing
The BIPQ was straightforward to cross-culturally adapt. The committee and the translators added ‘waist pain/lower back pain’ to ‘illness’ to make the measure back pain-specific for this study whilst allowing the measure to be used for other conditions in future studies. ‘Waist pain/lower back pain’ was read out to participants in this study. Forward translations were similar but back-translations revealed minor discrepancies in items 1, 3 and 5. The initial translation of ‘how does your illness (back/waist pain) affect your life?’ was modified to ‘to what extent does your illness (back/waist pain) affect your life?’ (Kedu oke ole oria gi (ukwu mgbu gi) si emetuta ndu gi?). This better reflects the original item 1 ‘how much does your illness affect your life?’ as ‘how’ and ‘how much’ are Igbo homographs. Similarly, for item 3, back translation showed that the item was translated as ‘what kind of control do you have over your back pain?’. The team corrected the item to ‘what extent of control do you feel you have over your back/waist pain?’ (Kedu oke njikwa i chere na i nwere ebe oria gi (ukwu mgbu gi) no?) to reflect the original item. In item 5, ‘how many’ was used in place of ‘how much’ in the translations as ‘how’ and ‘how much’ are homographs in Igbo. Therefore, the expert review committee used the Igbo equivalent of ‘to what extent’ to better reflect the original item (Kedu oke ole i na e nweta mgbaama (symptoms) na ihe gbasara oria gi (ukwu mgbu gi)?). In item 8, ‘…affect your heart or spirit’ was used as there is no Igbo word for ‘…emotionally’ (Kedu oke ole oria gi (ukwu mgbu gi) ji emetuta gi na uche ma o bu obi?). During verbal pre-testing, the Igbo word for ‘symptoms’ in item 5 was confusing to younger participants, hence the English word was included in bracket and both were read out which facilitated understanding.
Bland-Altman plot showing the test-retest agreement of the Igbo-BIPQ (Brief Illness Perceptions Questionnaire).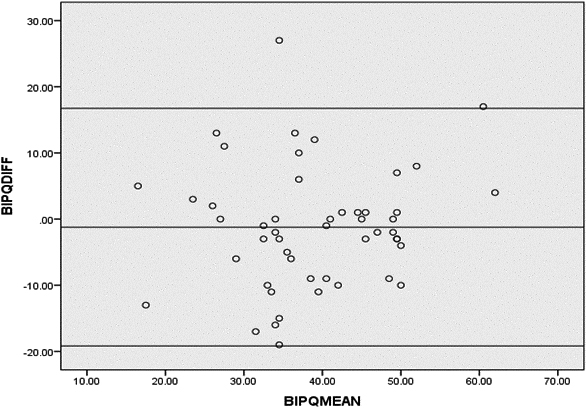
Test-retest reliability and cross-sectional validity testing sample characteristics
The sociodemographic characteristics of the two samples are presented in Tables 2 (test-retest sample) and 3 (cross-sectional validity sample).
Demographic characteristics of participants for cross-sectional validity testing
Demographic characteristics of participants for cross-sectional validity testing
Reliability and construct validity of the Igbo-BIPQ
BIPQ: Brief Illness Perceptions Questionnaire;
Table 4 below shows that internal consistency (
Figure 2 below shows that the agreement was acceptable between test-retest values of the Igbo-BIPQ as mean difference was close to zero and most points were within the 95% limits of agreement of the mean difference.
Construct validity
Table 4 below illustrates that the Igbo-BIPQ had significant moderate positive correlations with pain intensity (
Ceiling and floor effects
None of the participants scored 0 or 80 on the Igbo-BIPQ.
Discussion
This study enabled the cross-cultural adaptation of the first Igbo measure of illness perceptions. The adaptation of the Igbo-BIPQ was straight forward. Minor issues were related to ‘how’ and ‘how much’ being Igbo homographs depending on the context. Therefore, ‘to what extent’ was used in place of ‘how much’ to retain conceptual equivalence. ‘Affect your heart/spirit’ was used to echo the emotional concept in item 8 due to lack of an Igbo word for emotion. This finding was reflected in a qualitative study conducted in this population which suggested that the lack of an equivalent Igbo word for depression encouraged the use of bodily symptoms for the expression of emotional state [10]. The expression of emotional states through somatisation, common in non-western settings [31], has been shown to reinforce physical symptoms in West Africans [32].
The fact that younger participants understood ‘symptoms’ but not its Igbo equivalent in item 5, may be because younger people mix Igbo and English words in their daily communications in Nigeria to such an extent that they are likely no longer familiar with some Igbo words as opposed to older people. Moreover, English is the official written and spoken language of instruction in Nigeria. Problems with quantifying symptoms in item 5 of the BIPQ have been similarly observed in the Netherlands [33].
The internal consistency (
This study enabled the development of a valid and reliable measure of illness perceptions, which may be especially useful for rural dwellers in Nigeria often neglected clinically and during research despite being the most vulnerable. Despite acceptable validity and reliability of the Igbo-BIPQ, high sample variability and measurement error suggested by the values of the SEM and MDC may have been partly introduced by low literacy rates, interviewer-administration in place of self-administration, and data collection by several raters. This is important considering that MDC not only depends on the inherent measurement error of an instrument but varies across populations and contexts. For instance, interviewer-administration in place of self-administration might have introduced an external bias due to the possibility of interviewers’ style of communication at each time point stimulating different participant responses. Interviewer-administration by several raters could have produced different responses among participants if interviewers’ style of communication were significantly different. To the authors’ knowledge, minimal clinically important difference has not been established for the BIPQ. Therefore, a limitation of this study is the lack of responsiveness data which makes it unclear whether the MDC of the Igbo-BIPQ is sufficiently small to detect minimal clinically important difference. Therefore, future sensitivity-to-change studies are required with single raters, and using more rigorous analysis such as receiver operating characteristic curves, which includes patients’ own global impression of change. These studies need to determine the minimal clinically important difference and confirm the MDC of the Igbo-BIPQ.
Lack of bilingual testing of the Igbo-BIPQ incorporating item by item agreement between the original English BIPQ and the Igbo-BIPQ and comparing self-administration with interviewer-administration are limitations of this study. These should be done in future studies in populations with high literacy to enable comprehension of and literacy in English and Igbo. The validation of the Igbo-BIPQ with only pain intensity and self-report disability measures due to lack of an Igbo illness perceptions measure is another weakness. However, validity of the Igbo-BIPQ is supported by correlations with pain intensity and self-reported disability which are in line with the established literature. The Igbo-BIPQ can subsequently be used to validate other illness perceptions measures in this population.
Conclusion
The Igbo-BIPQ (Appendix) appears to be a valid and reliable measure of illness perceptions and can be used for clinical and research purposes in Igbo speaking populations. The measure requires further testing to confirm its validity, reliability and utility.
Compliance with ethical standards
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional research committee and with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards.
Funding
Data collection was funded by the Tertiary Education Trust Fund, Nigeria and the Schlumberger Faculty for the future fellowship grant, The Netherlands.
Informed consent
Informed consent was obtained from all participants included in the study.
Footnotes
Conflict of interest
The authors declare that they have no conflict of interest.
Appendix
The Igbo Brief Illness Perceptions Questionnaire (IGBO-BIPQ).
1. Kedu oke ole ọrịa gị (ukwu mgbu gị) si emetụta ndụ gị?
0
1
2
3
4
5
6
7
8
9
10
o metụtaghị
o meuụtara ndụ m nke
m ma ọlị
ukwuu
2. Ogologo oge ole ka ọ dị gị ka ọrịa gị (ukwu mgbu gị) ga anọgide?
0
1
2
3
4
5
6
7
8
9
10
obere
ebighi ebi
oge
3. Kedu oke njikwa i chere na i nwere ebe ọria gị (ukwu mgbu gị) nọ?
0
1
2
3
4
5
6
7
8
9
10
Njikwa
adịghị ma
ọlị
njikwa nke ukwuu
4. Kedu oke ole ọ dị gị ka ọgwugwọ ị naanata ga enyere ọria gị (ukwu mgbu gị) aka?
0
1
2
3
4
5
6
7
8
9
10
ọ naghị
enyere m
ọ na enyere m aka
aka ma ọlị
nke ukwuu
5. Kedu oke ole ị naenweta mgbaama (symptoms) na ihe gbasara ọrịa gị (ukwu mgbu gị)?
0
1
2
3
4
5
6
7
8
9
10
ọ dịghị ịhe
mgbaama
ọtụtụ ịhe mgbaama
ma ọlị
na enye oke nsogbu
6. Kedu oke nchegbu i nwere maka ọrịa gị (ukwu mgbu gị)?
0
1
2
3
4
5
6
7
8
9
10
ọ naghị
eche m uche
ọ na-eche m uche
ma ọlị
nke ukwuu
7. Kedu oke ole i chere na ị ghotara ọrịa gị (ukwu mgbu gị)?
0
1
2
3
4
5
6
7
8
9
10
Aghọtaghị m
aghọtara m ya, o doo
ya ma ọli
m anya nke ọma
8. Kedu oke ole ọrịa gị (ukwu mgbu gị) ji emetụta gị na uche ma ọ bụ obi? (dịka, ọ na-eme gị iwe, ụjọ, obi ọjọọ ma ọ bụ obi ị da mba/iweda mmụọ gị?)
0
1
2
3
4
5
6
7
8
9
10
ọ naghị
ọ na-emetụta uche
emetụta uche
ma ọ bụ obi m nke
ma ọ bụ obi m ma oli
ukwuu
9. Biko depụta ma ọ bụ kwuo n’usoro ihe atọ kacha mkpa i kwere na ọ bụ ha butere ọrịa gị (ukwu mgbu gị). ihe ndị kacha mkpa butere m ya bụ:
____________________ ____________________ ____________________