
Abstract
BACKGROUND:
Proprioception, one’s sense of movement and position, is a common term used in back rehabilitation. Kinesthetic rehabilitation may be useful in managing lower back pain; however, reliable measures are required to quantify lumbar proprioception sense.
OBJECTIVE:
To investigate intrarater and interrater reliability of neutral lumbar positioning (NLP) and target lumbar positioning (TLP) tests and compare the position sense errors in subjects with non-specific low back pain and healthy controls.
METHODS:
Intrarater (between-day) and interrater (within-day) reliability of NLP and TLP tests were assessed in 30 subjects with low back pain and 30 healthy subjects using a digital inclinometer. NLP is evaluated when the subject is repositioned to neutral from flexion, while TLP is evaluated in lumbar flexion, by bending laterally left and right.
RESULTS:
Intrarater reliability for NLP tests had ICC values of 0.85 and 0.89 and TLP tests had 0.78 and 0.92. Likewise, interrater reliability for NLP had ICC values of 0.75 and 0.85, and for the TLP test, the interrater reliability had 0.78 and 0.93. Subjects with back pain had significantly larger neutral and target lumbar proprioceptive errors compared to healthy controls (
CONCLUSIONS:
Intrarater and interrater reliability showed good agreement for both NLP and TLP tests of lumbar proprioception. Subjects with nonspecific low back pain have impaired lumbar proprioceptive sense.
Introduction
Non-specific lower back pain (LBP) is common globally, affecting more than two out of three adults aged 40–80 years with a one-year prevalence of 22–65% [1, 2]. LBP is a leading cause of hospitalization and creates a substantial financial, community and personal burden [3, 4]. Recent research has focused on different mechanisms underlying LBP and findings indicate that lumbar neuromuscular or proprioceptive dysfunction are critical factors in the development and maintenance of LBP [5, 6]. Proprioception refers to one’s sense of afferent information originating from muscle, tendon and joint mechanoreceptors that are processed at spinal, brainstem, cerebellar and cortical levels, resulting in accurate movement and joint stability through appropriate neuromuscular output [7, 8, 9].
Research has shown sensory-motor impairment and poor proprioception in subjects with LBP, which can affect spinal stability leading to articular cartilage changes [10, 11, 12, 13]. Some studies involving subjects with LBP showed significant proprioceptive and motor control disturbances associated with the presence of acute pain, chronic pain, muscle fatigue and the number of prior injuries [14, 15, 16, 17, 18]. Other studies, however, failed to find differences in subjects with and without LBP [16, 19]. Osthoff et al. [11] conducted a systematic review and meta-analysis to see the accuracy of lumbar position sense in low back pain subjects and concluded that future studies should pay closer attention to the precision and reliability of the measurement approach.
In contemporary clinical practice, different evaluation methods of assessing lumbar proprioception have been considered, as it is essential for therapists to have access to an objective measuring tool. These include the appreciation of joint position during active movement [20], passive movement using an external device [21], or repositioning to neutral or target positioning [13, 22]. During neutral lumbar positioning (NLP), the subject re-positions to neutral lumbar position once they moved from flexion or extension. During target lumbar positioning (TLP), the subject re-positions to a predetermined target position. In NLP and TLP, objective test measures in alterations of proprioceptive awareness are expressed as errors in lumbar re-positioning.
Different studies have used analysis devices, such as 3space FastTrack, Lumbar Motion Monitor, electrogoniometer and a piezoresistive amplified and temperature compensated accelerometer [23, 24] and have reported good intra and intersession reliability (intraclass correlation coefficient (ICC) values
Subjects with non-specific LBP are often treated over periods lasting from days to weeks in rehabilitation clinics. Insight into the intra- and inter-rater reliability of digital inclinometer to measure lumbar reposition sense are essential for a better understanding of the device and its applications. We used healthy subjects to allow the characterization of any normal variation that may occur in the absence of the confounding effects of interpretation that may arise within an LBP population. This study aims 1) to assess the intra- and inter-rater reliability of NLP and TLP tests in subjects with and without LBP and 2) compare the magnitude of proprioceptive errors between subjects with and without non-specific LBP.
Methods
Study design
An intrarater (between-day) and interrater (within-day) cross-sectional study design was used with a three-phase reliability protocol that consisted of 1) preparation 2) training and 3) overall agreement. The reliability protocol used is recommended by the International Academy of Manual/Musculoskeletal Medicine (IAMMM) [26]. The preparation phase consisted of researcher agreement on study conditions and strategy. The training phase focused on replicating test procedures and examiner judgment. The focus of the third phase was to establish an overall agreement percentage (
Participants
The King Khalid University Ethical Committee granted permission for the recruitment of 30 healthy and 30 non-specific LBP subjects (REC#2018-06-17). In order to recruit healthy subjects, an advertisement in the form of posters and word of mouth was conducted on the University campus. Subjects were included if they agreed to participate voluntarily, had no any previous lower back injury ever and no other lower limb or trunk pathology, deformity, or condition that may alter motor control. Non-specific LBP subjects were recruited from the University’s physical therapy clinic following referral by an orthopedic surgeon and included if they had mechanical non-specific LBP [27], at least two episodes of pain within the past year. LBP subjects were excluded if the source of back pain was non-musculoskeletal, or if they had a history of neurologic involvement, or previous surgery to the back, abdomen, or chest. All subjects read an information sheet and signed a consent form prior to the study.
Examiners
Clinical data were collected by two physical therapists (examiners A and B) working in the University’s physical therapy clinic. Both have a minimum of ten years of experience. Two data recorders were employed; recorder 1 (with examiner A), and recorder 2 (with examiner B). The recorders collected data using standardized record sheets. The order of examinations was randomized so that no one examiner evaluated all LBP subjects first, and both examiners were blind to each other’s results and to whether the subjects had LBP.
Procedure of testing neutral and target lumbar positioning tests.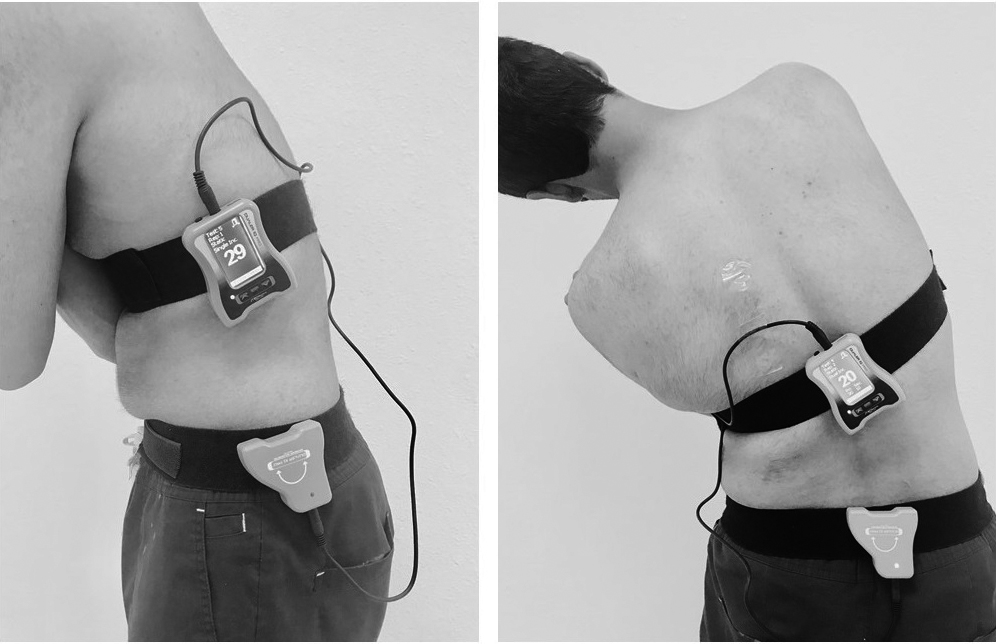
Dualer IQ digital inclinometers (DIs; J-Tech Medical, Midvale, UT, United States of America) were used to measure lumbar JPE (Fig. 1). Digital Inclinometers are reliable, fast, high in measurement precision [28, 29] and allow clinicians to evaluate ROM and proprioception using dynamic inclinometry similar to that used in other goniometric protocols [30]. The digital inclinometers have shown test-retest reliability for measuring spinal ROM [31, 32] and evaluation protocols are well established and endorsed by the American Medical Association (AMA) [31].
Sample size calculation
We used a formula developed by Walter et al. to estimate sample size for reliability [33]. The minimum acceptable intraclass correlation coefficient (ICC) (
Data collection
Prior to the study, all subjects were informed about the procedures in detail. Recruits who met the inclusion criteria became participants, and their first evaluation session was scheduled. Demographic variables (age, height, weight, education level) were recorded. Back pain intensity (subject experiencing at the moment of testing) was evaluated using the 100 mm visual analog scale (VAS), with 0 mm indicating “no pain” and 100 mm indicating “worst imaginable pain.” In addition, all subjects completed the Oswestry Disability Index (ODI), a self-reported questionnaire used to evaluate disability due to LBP. ODI is a 10-item questionnaire with six response categories for each item (range 0–5, a total score between 0–50); a lower score reflects better function. The score is converted to a percentage for analysis.
Upon completion of the questionnaire, subjects were asked to carry out lumbar repositioning to neutral and lumbar repositioning to target testing with examiner A, followed by a 15 minute break. Afterward, subjects continued repositioning tests with examiner B. Each session lasted approximately 20 minutes and for the test-retest, subjects were seen one day apart within
Demographic characteristics of patients with back pain and healthy subjects
Demographic characteristics of patients with back pain and healthy subjects
LBP: low back pain; Cm: centimeters; Kg: kilogram; mm: millimeters; BMI: body mass index; VAS: visual analog scale; ODI: Oswestry Disability Index. Elementary school
Subjects were instructed not to perform any strenuous physical activity for 24 hours prior to testing and not to drink or eat two hours prior to testing (in order to minimize cutaneous input from a distended abdomen). For testing, subjects were blindfolded to eliminate visual input and the room was kept quiet to limit auditory input. Subjects were asked to stand in a neutral position, with their knees straight and weight equally on both feet. The primary sensor digital inclinometer was placed over the lateral chest (T12 level) and secondary sensor over the hemipelvis (S1 level) in the sagittal plane to measure lumbar reposition errors in flexion. A primary sensor (T12) and secondary sensor (sacral midpoint) in the frontal plane were used to record lateral bending angle error (Fig. 1). Velcro straps were used to secure the digital inclinometer for testing.
For NLP, subjects were asked to maintain the lumbar spine in a neutral position with their eyes closed. The inclinometer was calibrated to a starting position (0 degrees) by the examiner. The subjects memorized this neutral position for a few seconds, performed active full flexion, and then relocated to a neutral position. Subjects were instructed to perform the test as accurately as possible and indicate verbally when they thought they had returned to the starting position. Relocation accuracy was measured in degrees. The NLP test was performed in one direction only (lumbar flexion).
For TLP, the examiner guided at a slow steady pace that subject’s lumbar spine reached a predetermined target, 50% of the maximum ROM. This range was chosen so that all subjects could achieve it. The spine was maintained in the target position for 5 seconds, subjects were asked to remember the position and the lumbar spine was guided to a neutral position Subjects were then asked to actively re-position by bending the spine to the target position. When the subjects reached the reference position, relocation accuracy was measured in degrees. Subjects performed a total of three trials for each movement direction (flexion, lateral bending). The average of three trials was used for analysis. The order in which movement directions were tested was randomized using a simple lottery method. Only the absolute error was taken as a measurement, which is the difference between the actual angle relative to the target angle and thus has no directional bias when compared to constant error or relative error.
Statistical analysis
Data were analyzed using SPSS software version 20 (IBM, SPSS Inc., Chicago, IL, USA), checked for normality using the Shapiro-Wilk test, and found to follow a normal distribution. Independent
For evaluating the agreement between rater scores, Bland-Altman’s Limits Of Agreements (LOA) was used [35]. Measurement errors were estimated by standard error of measurement (SEM) using the formula: SEM consistency
Results
A total of 60 subjects (30 with LBP, 30 healthy) participated and completed first and second assessment sessions. The demographic characteristics are summarized in Table 1.
Intra-rater reliability of NLP and TLP tests
Intra-rater reliability of NLP and TLP tests
NLP: neutral lumbar position; TLP: target lumbar position; SB: Side bending; 95% CI: 95% confidence interval; ICC agreement: intraclass correlation coefficients; Mean diff AB: mean difference between examiner A and B; SD diff AB: standard deviation of the mean difference between examiner A and B; SEM: standard error of measurement; SDC: smallest detectable change.
Inter-rater reliability of NLP and TLP tests
NLP: neutral lumbar position; TLP: target lumbar position; SB: side bending; 95% CI: 95% confidence interval; ICC agreement: intraclass correlation coefficients; Mean diff AB: mean difference between examiner A and B; SD diff AB: standard deviation of the mean difference between examiner A and B; SEM: standard error of measurement; SDC: smallest detectable change.
Difference in scores between patients with back pain and healthy controls
NLP: neutral lumbar position; TLP: target lumbar position; SBR: side bending right; SBL: side bending left;
Bland-Altman plots of intra-rater reliability NLP and TLP measurements by examiner A and B. The solid lines indicate the reference mean. The dotted lines indicate the upper and lower limits of agreement.
Bland-Altman plots of inter-rater reliability NLP and TLP measurements by examiner A and B. The solid lines indicate the reference mean. The dotted lines indicate the upper and lower limits of agreement.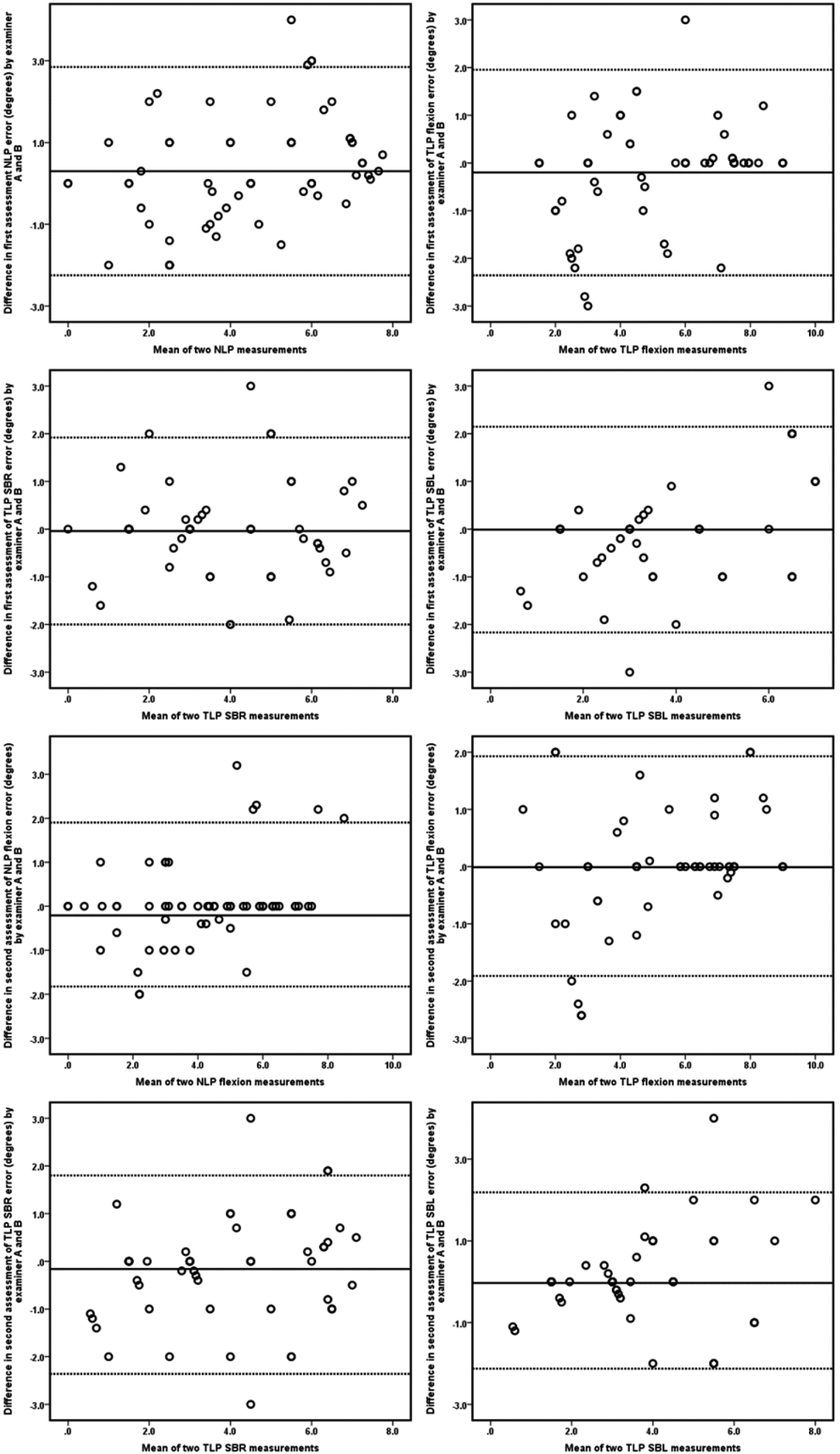
The intrarater reliability of NLP and TLP tests (examiner A and B) is summarized in Table 2. Intrarater reliability for the NLP test showed very good agreement with ICC values between 0.85 and 0.89. SDC ranged from 1.85
Interrater reliability
Interrater reliability results are summarized in Table 3. Overall, interrater reliability for NLP showed good to very good agreement (ICC values ranging between 0.75 and 0.85). For TLP, interrater reliability for the First Assessment showed good to very good agreement with ICC values of 0.78 (95% CI [0.64–0.87]) for lateral bending and 0.86 (95% CI [0.76–0.91]) for lumbar flexion. Likewise, interrater reliability for the Second assessment showed good to very good agreement with ICC values of 0.77 (95% CI [0.62–0.86]) for lateral bending and 0.88 (95% CI [0.80–0.93]) for lumbar flexion (Table 2). TLP tests showed very
good agreement with ICC values
Comparison of results between LBP and healthy controls
For NLP and TLP, statistically significant differences were found in all movement directions. Subjects with LBP showed significantly larger repositioning errors compared to healthy subjects (
Discussion
This study assessed two aspects of back proprioception; namely repositioning of the lumbar spine to neutral and target positions using an unsophisticated and inexpensive inclinometer device. Results show that both intra and interrater reliability was high using the inclinometer as a measuring device for NLP and TLP tests. We assessed proprioception acuity using active movement reproduction tasks, as performance under such testing conditions has been shown to be a good predictor of proprioceptive acuity.
Intra and interrater data showed good reliability determined by ICC, SEM and SDC values. An LOA plot between the two did not show any systematic bias, as expected Both examiners used the same instructions and the protocol was specific and rigorous; thus, examiners had little opportunity to influence subject performance. Both had considerable experience testing the lumbar position sense extensive discussion prior to investigation.
Few studies report data on ICC confidence intervals, statistical power, SEM, or SDC in order to establish intrarater reliability for lumbar proprioception in NLP and TLP tests. Many report a lack of reliable and valid tools to measure proprioception [37]. Our study results are in accordance with Koumantakis et al. [38] study; test-retest reliability was obtained from non-specific LBP subjects in a standing position using a lumbar motion monitor and showed an ICC of 0.76–0.80 and SEM: 0.91
Monitoring and observing the beneficial effects of treatment is of great importance and is the substance of modern evidencebased health care. SDC and minimal clinically important difference (MCID) can be used as benchmarks for the interpretability of a joint position error to determine whether the observed change is beneficial to the patients. To determine whether a change score on an individual patient level is clinically important and not just measurement error, the SDC score must not exceed the MCID change score [41]. In this study, SDCs for NLP tests were between 1.85
Koumantakis et al. [38] and Astfalck et al. [42] reported significantly larger errors in lumbar flexion in subjects with LBP compared to controls. The present study shows similar findings; subjects with LBP have significantly larger errors in lumbar flexion compared to healthy individuals. There are inconsistencies in the literature regarding the limits between physiological proprioceptive variation and proprioceptive deficits. Studies have reported a threshold value range of 1.3
Swinkels et al. [44] and Lin et al. [45] showed a higher mean proprioceptive threshold of 5.27
This study calculated ICC, SEM, and LOA values in order to provide a representation of different aspects of reproducibility (reliability and agreement), as failure to do so has been a criticism of previous studies [48, 25]. Unfortunately, our data collection procedure did not permit analysis of consistent over or undershooting of the target position as a part of the observed outcome variability. A tendency for LBP subjects to overshoot the target compared to healthy subjects was noticeable. Similar findings have been reported previously [49, 50, 48].
Limitations
NLP and TLP absolute errors were recorded in this study; constant and variable errors were not considered. Examiners had expertise in physical therapy and lumbar proprioception; thus, intra and interrater reliability should be reproducible by other professionals. Data collected by inexperienced physical therapists may differ in reliability.
Conclusion
This study investigated the reliability of NLP and TLP tests using time- and cost-effective methods similar to those used in physical therapy clinical practice. Intra- and inter-rater reliability ranged from good to very good agreement in both LBP and healthy subjects. Subjects with non-specific LBP seemed to produce larger lumbar joint position errors compared to healthy controls. Clinometric properties in this study are related to non-specific LBP only; in other lumbar pathologies, the quality of the performance of the actual measurements might differ.
Footnotes
Acknowledgments
We thank the Deanship of Scientific research, King Khalid University, Abha, Saudi Arabia, for providing support.
Conflict of interest
None to report.
Funding
This work was funded by a grant (GRP/59/42) from King Khalid University, Abha, Saudi Arabia.