
Abstract
BACKGROUND:
There are currently no reports of biomechanical changes in patients with forward head posture (FHP) that result in altered muscle activation throughout various functions with muscle activation response during diverse sleep postures.
OBJECTIVE:
This study investigated neck and back muscle activity in individuals with and without FHP during a maintained side-sleeping position by incorporating various pillow designs.
METHODS:
Thirty-four participants (i.e., 17 in each group) were enrolled. The muscle activity was investigated via surface electromyography during the use of three trial pillows: orthopedic pillow, hollow pillow, and Thai neck support pillow.
RESULTS:
With the application of all three trial pillow, the FHP group demonstrated significantly greater middle-lower trapezius muscle activity than the normal head posture group (
CONCLUSIONS:
Feasibly, the ability to appropriately modify a pillow configuration without creating undesired muscle activation was limited to those exhibiting FHP. Therefore, specially designed pillows or mattresses should be investigated in terms of their relevance to muscle fatigue and potential musculoskeletal pain in FHP patients.
Introduction
Forward head posture (FHP) is a poor habitual cervical posture that constitutes one of the most common postural problems [1]. FHP is strongly associated with various musculoskeletal disorders such as neck pain, suboccipital trigger point, headache, poor neck mobility, and functional disability of the neck and thorax [1, 2, 3, 4, 5]. In the modern world, prolonged positioning while using computers, smartphones, or other media devices often exposes individuals to a possible increased prevalence of FHP [6]. This cervical misalignment in a sagittal plane refers to the head positioned anterior to the vertical line passing the lateral malleolus [7]. This postural deviation involves increased upper cervical extension and lower cervical flexion, which can result in compensatory action such as increased thoracic kyphosis and rounded shoulders [8]. These structural changes result in imbalances in muscle tension, altered muscle strength and morphology, reduced movement and function of the cervical spine and thorax, and altered muscle recruitment around the neck and back [9, 10, 11, 12, 13, 14]. It is feasible that these biomechanical changes alter the stresses on the musculoskeletal structure around the neck and back during both functional movement and various resting postures, including sleep postures
Musculoskeletal pain (i.e., cervical pain and stiffness, headache, or scapular pain) can cause an individual to awaken [15]. A good support pillow can reduce waking and pain, as well as improve sleep quality and comfort [16]. Previous studies have reported varying results in terms of symptomatic neck pain and headaches after the incorporation of standard pillows [17]. Additionally, many subjects who reported the use of uncomfortable pillows presented with symptoms of regular waking and poor sleep quality [18]. Gordon et al. [19] recommended that in addition to the investigation of the performance of neck pain pillows in specific groups, reduced pillow comfort, sleep quality, and musculoskeletal pain should also be evaluated. Therefore, recommendations regarding appropriate pillows for FHP should be examined to focus on the prevention of futher serious changes in spinal pathatogy or development of early degenerative spinal disease.
Individuals in the working-age to old-age population spend most of their sleep duration in the side-lying position [20]. Ideally, a proper pillow should be used to support and maintain normal spinal alignment while minimizing biological stress on the musculoskeletal structure throughout sleep. Consequently, horizontal alignment of the spine in the side position should be maintained while using the most appropriate pillow [21]. Furthermore, a good support pillow should minimize the activity of the neck and back muscles [22, 23], promote symmetrical activation of the bilateral muscle [24], and provide good perception of comfort [25]. Poor et al. [22] reported that the activity of the neck muscles was reduced when the cervical and lumbar spines were aligned horizontally with the use of an optimum pillow during side-lying. Sacco et al. [26] demonstrated that the middle trapezius (MT) muscle experienced the greatest activation during side-lying at the least comfortable pillow height.
Although several previous studies focused on developing and testing neck support pillows with the aim of reducing waking symptoms, providing relaxation, and ensuring a good resting position, there is no consensus on the most effective pillow [16, 19, 21, 23, 24, 25]. A wide variety of pillows exhibiting different shapes, fillings, and fabrics are available on the market. In order to select the optimum pillow, several important factors must be considered, including pillow designs (such as shapes and height) and the type of material used. To avoid unwanted physiological stress, a pillow should provide a good alignment position angle [21] and the least amount of muscle activation [24, 26, 27]. The slope of the cervico-thoracic spinal segment changes significantly when an individual changes from a foam, latex, or polyester pillow to a feather pillow and vice versa; however, there is currently insufficien evidence to support the suggestion of a foam contour pillow over a foam regular pillow to achieve a neutral posture in the cervico-thoracic spine in side sleepers [21]. Latex pillows have been reported to reduce the frequency of waking, headache, and scapular/arm pain [17]. In addition, foam pillows with a height of 10 cm were found by Sacco et al. to be superior to pillows with heights of 5 and 14 cm, which increased the activity of the MT muscle as well as cervical tension and morning pain. Second, the underlying characteristics of the pillow user are important, as individuals who reported waking during the night from poor cervical posture reported increased biomechanical stress on the cervical spine structures, which activated cervical pain and stiffness, headache, and arm or scapular pain [17]. In addition, Palazzi et al. found asymmetrical bilateral sternocleidomastoid (SCM) activity during lateral decubitus on two pillows (Sleep Easy and the standard pillow) in both healthy individuals and patients with myogenic cranio-cervical-mandibular dysfunction [24]. In addition, a recent study found that in young adults with FHP, the overactivation of the upper trapezius (UT) and lower trapezius (LT) in could be induced in the side-lying position using a self-selected pillow [28]. There is a scientific gap in the literature regarding the muscle activation response in FHP patients who use different pillow designs. Hence, this study investigated the activity of the neck and back muscles during a maintained side-sleeping position by incorporating various pillow designs in individuals with and without FHP.
The three trial pillows. A. Orthopedic pillow (OP); B. Hallow pillow (HP); C. Thai neck support pillow (TP).
Participants
We calculated the required sample size using a power analysis [29] based on the percentage of maximum voluntary contractions (%MVC) of the UT from the pilot study. A mean
The study included healthy men and women aged 18 to 35 years, with a body mass index (BMI) less than 25 kg/m
We evaluated the sagittal plane head postural readings of all participants from the lateral view imaging during relaxed standing with the participants’ arms by their sides. A digital camera (Sony model HDR-PJ440, Sony, USA) was set at the level of the participants’ shoulders at a distance of 1.5 m without rotation or tilt. A plumb line was suspended from the ceiling and used to verify the true vertical line. Head posture was recognized via two steps: plumb line assessment and craniovertebral angle (CVA) measurement [10]. The plumb line was set to pass anteriorly at the participants’ lateral malleolus. Participants’ ear tragus and C7 spinous process were palpated and marked with double-sided tape. CVA was measured using Adobe Acrobat software, which referred to the angle between the line joining the participants’ ear tragus and their C7 spinous process. The horizontal line was considered as passing through the C7 spinous process, as described in the guideline by Salahzadeh et al. in 2014 [7]. Participants were considered to have FHP if their ear tragus was in front of the plumb line with a CVA of less than 48
EMG evaluation protocol
In this study, we purchased the three pillow designs for evaluation based on the most commonly used and most available in the Thailand market: an orthopedic pillow (OP), hollow pillow (HP), and Thai traditional neck support pillow (TP) (Fig. 1).
The OP was rectangular in shape (51
The test position consisted of side-lying, which is the typical position the participants slept in. Participants laid on the physical therapy treatment table with their head resting on each trial pillow, their knees flexed together at 90
The sequence of the pillow evaluation was randomized for each participant. The pillow type was written and placed inside an envelope. The sequence was set as a result of the envelope placement order as per participants. To set the washout period, participants were asked to lie down from the sitting position at the beginning of each trial pillow.
Surface EMG (SEMG) activity of the SCM, UT, MT, and LT bilateral side were collected using TELEMyo DTS telemetry (Noraxon Inc., Scottsdale, AZ, USA) with a sampling rate of 1500 Hz. A video camera (Intel
The process of locating and placing the electrode was performed according to the Surface Electromyography for the Non-Invasive Assessment of Muscles (SENIAM) guidelines [31]. If the skin was covered with hair, the electrode sites were shaved before the electrodes were placed on the skin. The skin was subsequently cleaned with alcohol and allowed to dry before electrode placement [31]. Standard disposable AgAgCl electrodes (Blue-Sensor, Ambu A/S, Ballerup, Denmark) were attached over each muscle and secured using Transpore 3M adhesive tape (3M, São Paulo, Brazil) with an interelectrode distance of 20 mm. Electrode locations were as follows: SCM at one-third the distance from the sternal notch to the mastoid process; UT at the halfway point between the acromion process and the C7 vertebra; MT at the halfway point between the medial border of the scapula and the spine at the T3 level; LT at the two-thirds point of the line from the root of the spine of the scapula and vertebra T8 [31].
The MVC of each muscle were measured to yield the normalization process. For MVC, the maximum isometric exertion against a manual resistance for 5 s, with two repetitions and at least 2 min of rest between, was carried out in addition to verbal encouragement from the examiner [32]. The testing position was carried out in accordance with muscle and sensory testing guidelines by Reese [33]. The MVC of SCM was performed with the spine and neck laterally flexed to the ipsilateral side while maintaining the head rotation to the contralateral side against an opposite resistance applied to the lateral aspect of the head. For UT, the scapula was elevated toward the occiput against resistance simultaneously applied over the superior aspects of the acromion and posterior aspects of the occiput while the participants were seated with their arms by their sides. For MT, scapular adduction accompanied by shoulder horizontal adduction was performed against resistance applied over the dorsum of the distal forearm in the prone position along with a 90
EMG processing and normalization
A digital band-pass filter (Lancosh FIR) was set between 20 and 500 Hz. EMG signals were full-wave rectified and processed to obtain the root mean square (using a moving 50-ms window). For statistical purposes, muscle activity values during the use of a trial pillow were normalized via MVC value (%MVC). While each trial pillow was being used, the EMG signaled at 6-min intervals from the last 7 min of a total 12 min for subsequent analysis. For each muscle, the greatest root mean square value from two MVC trials was identified for use during the normalization process.
Statistical analyses
We applied independent
%MVC of neck and back muscles during normal head posture (NHP) group vs. forward head posture (FHP) group amid the application of the three trial pillows
%MVC of neck and back muscles during normal head posture (NHP) group vs. forward head posture (FHP) group amid the application of the three trial pillows
Values presented as mean
Comparison of neck and back muscle activity among normal head posture (NHP) and forward head posture (FHP) groups during application of the three trial pillows. SCM, sternocleidomastoid; UT, upper trapezius; MT, middle trapezius; LT, lower trapezius. Values are presented as mean 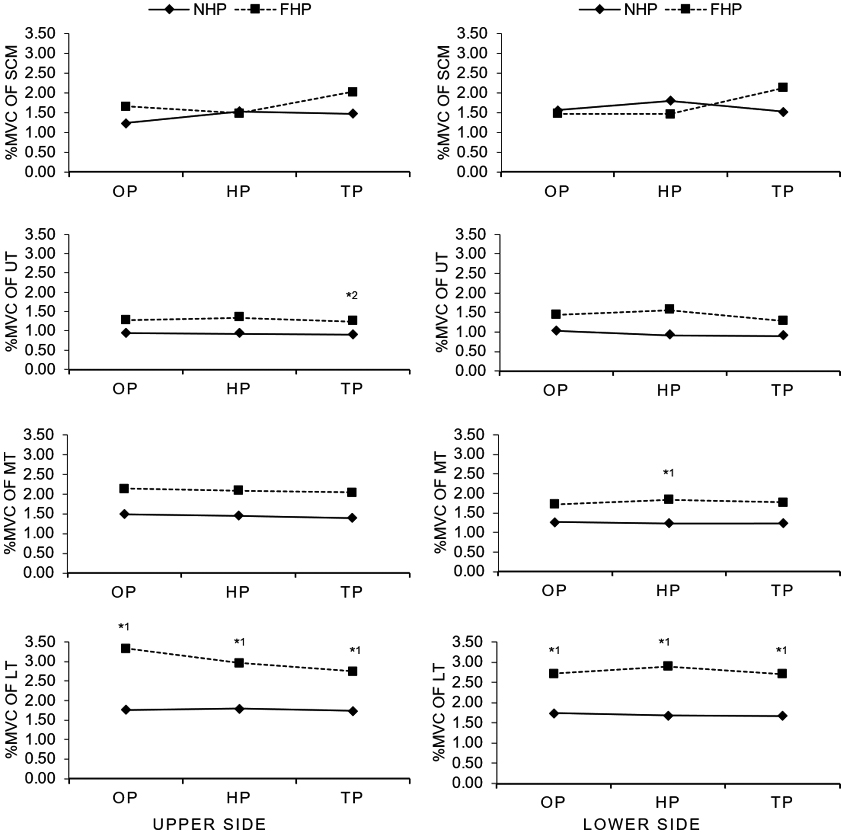
There was no statistically significant difference in participant demographic data, including age, weight, height, and BMI, between the NHP and FHP groups (
Discussion
A good support surface is a common strategy for reducing biological stress during sleep. An effective support pillow should reduce undesirable muscle activation [24, 26, 27]. Unfortunately, the influence of different pillow designs on the neck and back muscle activity in individuals with FHP remains unclear. Our study revealed four main findings. First, malalignment of FHP influences the increasing activation of the MT on the lower side and bilateral LT during rest in the side-sleeping position. Second, pillow designs, including OP, HP, and TP, cannot eliminate the overactivity of the LT in FHP. Third, the activation of the UT on the upper side was affected by differences in pillow design, with HP having the worst activation. Finally, all pillows helped participants with NHP to reach an optimum resting state without unnecessary SCM and trapezius muscle activation. Thus, we conclude, in accordance with our original finding, that an effective pillow for patients with FHP should be designed focusing on reducing the overactivity of the bilateral LT and MT on the lower side. HP might not be an effective pillow for FHP. TP was able to reduce unsatisfactory activity of the neck and back, similar to OP. However, all pillow designs could be recommended for individuals with NHP.
Our first finding was that the LT of both sides in FHP participants demonstrated a greater activity than that of NHP participants during side-lying using all three trial pillows. However, we found greater activity of the MT on the lower side when using the HP alone. This is in agreement with the findings of recent studies indicating that the activity of the UT and LT are higher in subjects with FHP than in those with NHP while in the side-lying position using a self-selected pillow [28]. Moreover, previous data showed overactivity of the UT, MT, and LT during shoulder movement in FHP as well as in the slouched position [13, 34]. This suggests a reaction response to unnecessary stress on the musculoskeletal structure around the neck, thoracic, and shoulder girdle in postural distortion.
Our second finding was that the trial pillows in this study were able to support and remove overactivity of the SCM and UT but not of LT in FHP. Congruent with previous studies, the activity of the SCM, UT and MT muscles was reduced if the cervical spine was aligned horizontally during sidelying by incorporating an optimum pillow height [22, 26]. Moreover, Sacco et al. [26] reported no increased muscle activity of SCM and UT while the participant was side-lying on pillow height of 5, 10 and 14 cm. This can be explained by the fact that the SCM and UT are inserted at the head and cervical spine, which are directly supported by a pillow. Although the attachment of the MT and LT were higher in relation to the lower cervical, thoracic, and shoulder girdle, which make up a part of the base during sidelying, the overactivation of MT on the upper side was eliminated via support from all trial pillows, which in turn may have resulted in the additional support of the testing position, in which the upper side of the arm was rested in front of the trunk along with a pillow support.
Our third finding was that pillow design did not result in a difference in the effect on the activity of all muscles, except for the upper side of the UT, whereby the use of the HP demonstrated a greater activity than the use of the TP. The specific design of each pillow should be considered when evaluating this finding. First, regarding the U-line at the centermost position of the HP, the cervical region is well supported by the edge of the pillow, but the head lacks support. Stress over the cranio-cervical junction was reinforced. The UT may react to these undesirable stresses by increasing its activation because of its attachment to the external occipital protuberance and cervical spinous process. Finally, for both the OP and TP, the cervical region was supported by the pillow edge, with the head completely at rest on the OP B-curve upper surface as well as the regular upper surface of the TP. Accordingly, the curvature angle was attenuated, resulting in an even distribution of pressure over the cervical disc. As mentioned in a previous study [23], support rendered from different pillows affects the center of the supporting force position as well as the load-bearing distribution around the cranial and cervical regions.
In addition, the pillow’s shape and filling material could cause variable muscle activity observed during the use of different pillow designs. First, in terms of shape, several previous studies [19, 21] have reported that there is no advantage in the use of a contour-shaped pillow over a regular-shaped pillow, which is comparable with the OP and TP shapes in this study. Gordon et al. [19] studied cervical pain, sleep quality, and pillow comfort while applying different pillow types. These authors reported no difference in the effectiveness of a foam contour pillow over a regular-shaped foam pillow. Furthermore, Gordon et al. [21] found that the horizontal alignment of the cervico-thoracic spine in the side-sleeping position was similarly induced by both contour and regular foam pillows. Second, in terms of stuffing material, Kim et al. [35] reported that pillows made from harder materials provided superior cervical spine support capacity, whereas light sleep might be caused by a pillow made of soft material. These authors explained that pillows made of soft material provide a minimal stable support surface, and they discovered that pillows made from polyurethane foam (as in the OP) had a capacity for cervical spine support similar to that of a polypropylene pillow (which resembles polyester in the HP). In this study, the TP had the greatest hardness because of its quantity of kapok stuffing [35]. This study provides initial evidence supporting the positive effect of the TP with regard to the prevention of undesired muscle activation in the resting position among individuals with FHP. This is possibly the consequence of the combination effect of the pillow’s material and structure [17, 35, 36].
Our last finding was that there was no difference in muscle activity associated with the use of various pillow types in the NHP group. This can be explained by the fact that individuals without abnormal alignment are able to reach an optimum resting state without musculoskeletal stress by using any of the three trial pillow types. This is in disagreement with the findings of a previous study [24] in which the asymmetrical muscle activity between the bilateral sides during side-lying with two pillow types was found in both the unaffected population and patients with myogenic cranio-cervical-mandibular dysfunction. However, this discrepancy could have been caused by a variation between the two studies in trial pillows and subject pathology.
Limitations
The 12-min study period for each trial pillow in this study was based on previous research that suggested minor creeping of the spine and distortion of the mattress and pillow over 10 min. Hence, no alteration to cervico-thoracic posture while in the side position among different pillow types was observed [21]. Moreover, previous studies indicated that the effects of various pillow types and pillow height on muscle activity while lying down could be recognized within a 5-min or 10-min study period [26, 27]. However, our test setting incorporated a fully relaxed resting state and not a sleep state. Thus, there was no accordance with actual sleep. Moreover, this study was conducted in asymptomatic young adult participants because it was focused on prevention and to avoid numerous confounding factors regarding the degenerative process [37, 34]. Consequently, the clinical implementation of these findings was limited to asymptomatic young adults.
Conclusion
During the application of all three trial pillows, those exhibiting FHP presented greater LT activation than individuals not exhibiting FHP. Greater MT activation was found while applying the HP alone. Nevertheless, SCM and UT muscle activity were comparable between the two groups. Only UT muscle activity was affected by the different pillow types in that the HP induced greater muscle activity than the TP in the FHP group. We found no difference in muscle activity between all three pillow types in the NHP group. It can be said that individuals without FHP can modify their configuration to fit all three pillow designs without the accompanying undesirable muscle activation, whereas this ability was limited in individuals with FHP. Although the HP appeared to be inferior to OP and TP, the TP seemed to be the superior pillow with regard to providing minimal muscle activity in individuals with FHP during rest in the side-sleeping position. However, the TP was unable to eliminate overactivity of the LT. Consequently, specific regimens, such as specially designed pillows or mattresses should be further investigated to focus on eliminating overactivity in these muscles. Indeed, this is relevant to muscle fatigue and the potential for musculoskeletal pain in individuals with FHP.
Footnotes
Acknowledgments
This work was supported by the Faculty of Allied Health Sciences, Burapha University, Thailand.
Conflict of interest
The authors have no conflicts of interest to declare regarding this study. This research was not supported by any of the pillow companies mentioned in the study.