
Abstract
BACKGROUND:
Although commonly utilized treatments, no study has directly compared the effectiveness of joint mobilization and stabilization exercise in individuals with forward head posture (FHP).
OBJECTIVE:
This study aimed to investigate the effects of upper cervical and upper thoracic spine mobilization versus deep cervical flexors exercise (DCFE) in individuals with FHP.
METHODS:
Thirty-one participants with FHP were randomized into the mobilization (
RESULTS:
Participants in the mobilization group demonstrated significant improvements (
CONCLUSIONS:
The combination of upper cervical and upper thoracic spine mobilization indicated better overall short-term outcomes in CVA, NPRS, respiratory function, and GRC compared with DCFE in individuals with FHP.
Introduction
The smartphone distribution rate is continually increasing due to the gradual progress of information technology in modern society, and the average time spent on using a smartphone of the overall U.S population is 5.1 hours a day [1]. When a smartphone is placed at the chest level, the neck is excessively bent because the eyes look down [2]; therefore, the load on the cervical erector spinae and upper trapezius is high in order to adjust the neck balance [3]. The continuous load on the cervical spine results in degenerative changes in the joints and forward head posture (FHP) [4, 5]. As a result, these can worsen and result in the herniation of cervical intervertebral discs [6].
FHP can be defined as an aberrant state in which the head position is in front of the gravity line around the sagittal plane, with increased flexion of the lower cervical spine and upper thoracic spine and relatively increased extension of the upper cervical spine [7, 8]. FHP is an important factor in the stability of the cervical spine joint and balance of muscles, and is involved in neck pain and respiration function [9, 10]. However, patients with neck pain due to FHP have decreased muscular force and shortening of the neck muscles that are related to respiration [11, 12]. A previous study indicated that smaller the craniovertebral angle (CVA) in FHP, lower was the respiratory circulation function; [13] 83% of the patients with neck pain also had respiratory dysfunction [10, 14]. Particularly, FHP causes weakness of the deep neck flexors and rhomboids, and tightness of the pectoralis, upper trapezius, and anterior scalene muscles, which result in neck pain [15, 16, 17]. The weakness and shortening of neck muscles have an effect not only on the pain and limitation of movements but also on the diameter of the thoracic cage and lung volumes [18], and consequently can result in dysfunction of respiratory muscles such as the diaphragm and intercostal muscles [19].
Manual therapy and therapeutic exercises are generally used in order to treat neck pain in patients with FHP. Although a previous study used stretching of the shortened muscles and deep cervical flexors exercises (DCFE), a review of the recent literature showed that studies covering manual therapy and active exercise are becoming popular [20, 21]; these studies suggest that manual therapy when also applied to the thoracic spine is more effective rather than applying only to cervical spine [22]. Even though the studies that there are neck pain and respiratory dysfunction have gradually been identified, there is insufficient evidence for the effectiveness the joint mobilization and therapeutic exercise in individuals with FHP. Although FHP can be basically considered as an abnormality of neck flexion, it possibly has correlation with the thorax as well. The purpose of this study was to compare the effects of upper cervical and upper thoracic segmental mobilization, and DCFE on posture, pain, and respiratory function in patients with neck pain due to FHP.
Methods
Participants
Flowchart of the study design including recruitment, randomization, and follow-up.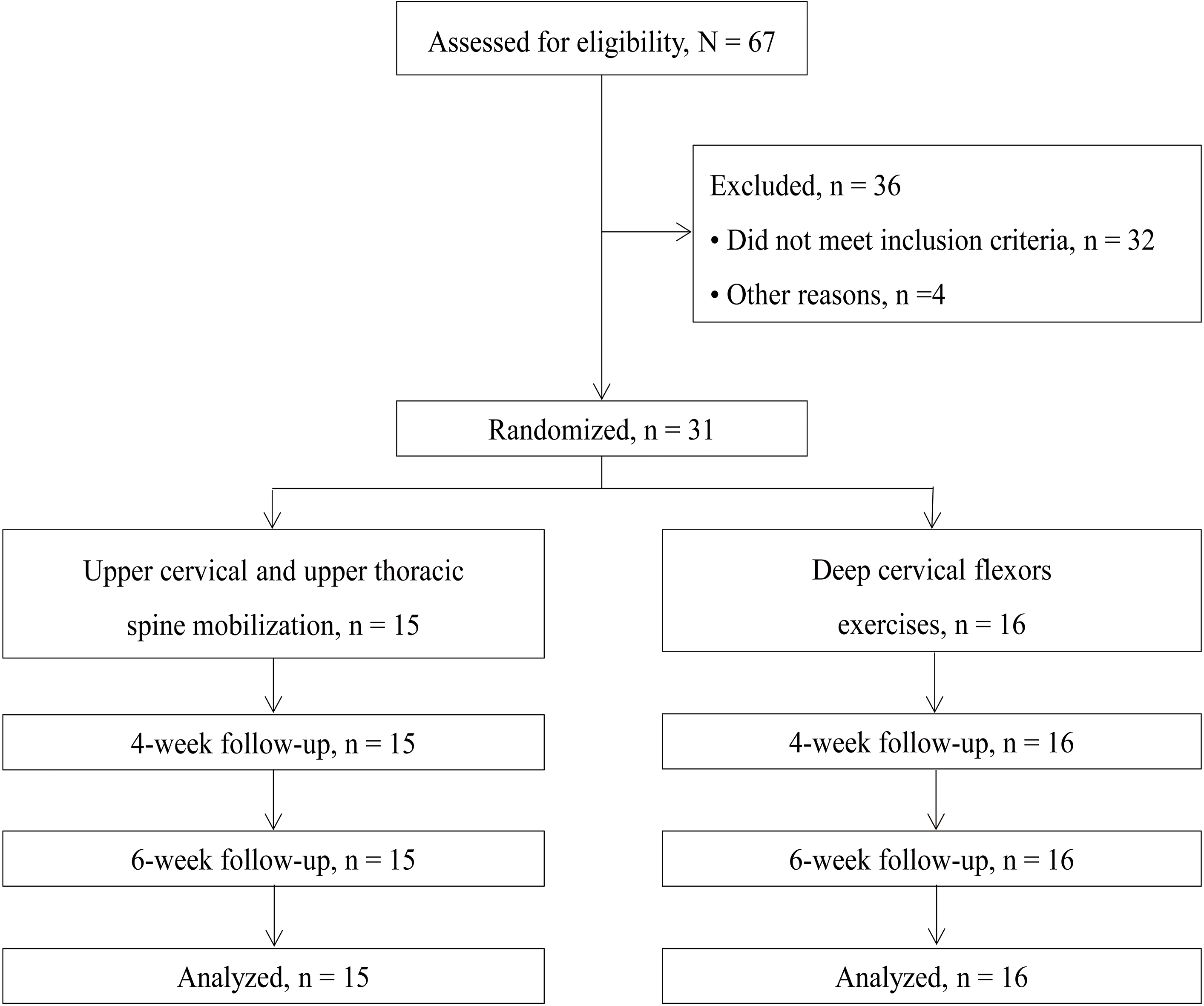
In this study, 31 participants with neck pain due to FHP were recruited by the Department of Rehabilitation Medicine in K-University Hospital from January to February 2017. The following inclusion criteria were applied: participants should have a primary complaint of mechanical neck pain, age from 20 to 29 years (age at which there is no degenerative change and deformation of the cervical vertebrae), and those who indicate the FHP symptom. For the diagnosis of FHP, the CVA was evaluated. Participants were excluded if they presented any serious pathology such as cancer, underwent prior surgery to the cervical or thoracic spine, and presented with positive neurologic signs consistent with nerve root compression. The number of required participants was calculated as G*Power 3.1 for the study [23]. This study was set according to the effect size f(V) 0.73 of the numeric pain rating scale (NPRS) in the previous study that compared the effect of manual therapy on the upper cervical and upper thoracic spine of neck pain patients [24]. Allowing for a conservative dropout rate of 20%, we planned to recruit at least 31 participants into the study. The participants were not informed of the research hypothesis, and the evaluator was blinded to the assignment of the treatment groups. All participants were instructed not to discuss any information related to the studied treatments with the other participants.
The period of this study was 6 weeks. The evaluations before and after the treatment were conducted after 10 sessions of interventions for 4 weeks, and follow-up revaluation was conducted after 2 weeks (Fig. 1). After the baseline examination, the 31 participants were randomly assigned to either the mobilization group (
Mobilization group
The participant sits in the right posture on a chair with back support and the therapist stands facing the left side of the trunk of the participant to improve the flexion of the upper cervical spine (C1-2) [25]. The therapist stabilizes the posterior cervical spine by covering with the right hand and placing the thumb and index fingers over the atlas. C1-2 segmental mobilization was performed to improve flexion according to the convex rule by moving the occipital condyle posteriorly using the left hand of the therapist (Fig. 2). That is, the therapist made the patient increase the motion of chin-in. After the joint mobilization was performed for one occipital condyle, the same was applied to the other side. The participant was in the prone position and the therapist stood facing the participant toward the joint that should be mobilized to improve the extension of the upper thoracic spine (T1-2) [25]. Index and middle fingers of the left hand were placed over the vertebral transverse process in the caudal targeted segment. After observing the movement by palpating the area between the spinous processes of the selected segments by using the index finger of the right hand, the lateral side of the right palm was placed on the index and middle fingers of the left hand and thoracic segmental mobilization was performed from the ventral to caudal parts (Fig. 3). An additional wedge was used to generate precise and strong local movements in the targeted segment. During the joint mobilization, the discomfort of the participant was checked and it was thrice per segment and a minute each time. A total of less than 10 minutes was spent with a break of 10 seconds per joint mobilization 30 seconds for intersegmental movements.
Upper cervical (C1 
Deep cervical flexors exercise used in this study.
DCFE was conducted in a manner similar to the cervical spine stabilization exercise [27]. Participants were asked to take up the crook lying position and then, inflatable air-filled pressure biofeedback sensor (Stabilizer; Chattanooga Group, Hixon, TX, USA) was placed over the suboccipital part on the back of the participant’s neck. Then, the participant was asked to perform light nodding for craniocervical flexion mobility. The performance started from 20 mmHg, the basis pressure was increased by 2 mmHg at every stage till 30 mmHg was reached in the final stage. When the performance was correctly conducted in each stage without reward mobility, the pressure was increased in the next stage [28]. A total of 3 sets were performed; one set consisted of repeating the motion 10 times for 10 seconds. The break time was 5 seconds per one movement and 30 seconds per one set; the total exercise time was less than 10 minutes. A previous study found intraexaminer reliability (ICC) of 0.78 and an interexaminer (ICC) of 0.54 for the performance pressure index, and an intraexaminer reliability of 0.78 and an interexaminer of 0.57 for the activation pressure score [29].
Measurements
Primary outcome measure used in this study was CVA as measured in the photograph of the profile of the participants. The participants maintained a natural head posture throughout the measurement method [30]. FHP evaluated CVA that was the angle that was made with the line that connected the 7th cervical spine with tragus and the horizontal line of the 7th cervical spine in standing position and less than 50 degrees was categorized into FHP in the previous study [31, 32]. The measurement process of two vertebral angles was reported to have high reliability in a previous study [33].
Characteristics of the participants in the study (
31)
Characteristics of the participants in the study (
Note. Values are indicated as mean
Secondary outcome measures included the NPRS, respiratory function, and global rating of change (GRC). To measure intensity of their current pain, we used an 11-point NPRS, and the NPRS has been shown to have high reliability and validity in previous studies [34, 35]. MDC of 2.1 points, with a minimal clinically important difference (MCID) of 1.3 points was indicated from neck pain patients [36]. In order to evaluate the respiratory function, the experiment was conducted with two devices; Desktop spirometer (Pony FX, COSMED Inc., Italy) and POWER breathe K5 (Hab direct, UK). The respiratory evaluation consisted five parameters, forced vital capacity (FVC), forced expiratory volume in one second (FEV1), peak inspiratory pressure (PIP), peak inspiratory flow (PIF) and peak inspiratory volume (PIV). Each parameter was measured thrice and the average value was used in the analysis.
GRC was used to assess self-perceived improvement at post intervention follow up only [37]. Clinically, GRC is being used to test the improvement in a patient’s symptoms objectively so as to identify the intervention effect and satisfaction after finishing the treatment, and this scale has demonstrated acceptable levels of reliability and validity. The MCID for GRC has been reported as a 3-point change from baseline [38].
The baseline characteristics of participants were compared between treatment groups, using independent
Results
The baseline characteristics between the groups were similar for all variables (
Outcomes of the craniovertebral angle, neck pain, and respiratory function (
31)
Outcomes of the craniovertebral angle, neck pain, and respiratory function (
Note:
The 2-way repeated-measures ANOVA for NPRS showed a significant group-by-time interaction (
In case of GRC after 4 weeks, the mobilization group demonstrated significantly (
A novel finding of this study is that FHP can be improved through a combination of upper cervical and upper thoracic spine mobilization, which results in the secondary benefit of reducing neck pain. The results of this study are in concordance with those of the studies that proved the effect of manual therapy in patients with neck pain [22, 39, 40].
For a long time, excessive smartphone use can cause health problems and syndrome such as FHP. Therefore, in this study the joint mobilization as treatment was conducted to enhance the flexion of the upper cervical spine and to improve the extension of the upper thoracic spine. According to the aim of the treatment, this study showed improvement of the CVA in mobilization group; there was a significant difference between groups through flow of time and there was an interaction. The previous study also reported that the limitation of mobility that was caused by pain was improved the most by progressing adhesion between joint hypo-mobility and soft tissues through joint mobilization [41, 42]. In addition, it was indicated that joint mobilization with the use of continuous passive stimulation could help improve the somatic sensory system and particularly, proprioception information [43, 44]. Accordingly it was considered that the improvement of spine alignment had an impact on the change in CVA between the groups through the benefit of the segmental mobilization. In this study, the average change in the NPRS score in the mobilization group exceeds, both, MDC and MCID values, and the gap between the groups was 1.4 over MCID. This suggests that there was a clinically significant difference due to the combination of upper cervical and upper thoracic spine mobilization.
In this study, respiratory function showed a significant difference between the groups over time, which is considered to be due to the improvement of joint hypo-mobility through segmental mobilization and posture by straightening the shortened abdominal wall. This posture and the improvement in mobility indirectly lead to improvements of respiratory function, and it is considered that there is a significant difference between groups. In particular, it seems that the improvement of respiratory function is due to the enlargement of thoracic diameter and improved lung volumes with normal spinal alignment. Maximum inspiration and expiration is generally accompanied by maximum contraction of the main respiratory muscles and expansion of the rib cage [45]. Therefore, enhancement of the five respiratory functions evaluated in this study implied an improvement of the thoracic cage by recovery of the normal posture. A previous study reported that there was a strong correlation between FHP and lung function [46]; therefore, the results of this study are in concordance with the result of a previous study that demonstrated improved respiratory function through joint mobilization and therapeutic exercises [47]. Although this study showed improvement of respiratory function after treatment for 4 weeks, there was no difference in the inspiratory force between the groups after 6 weeks. This is why joint mobilization is not the intervention that can directly help the reinforcement of inspiratory muscles; moreover, it does not have a sustained effect on inspiratory muscles like DCFE does, which is a low-intensity isometric exercise for the improvement of cervical instability in both groups. As a result, there is improvement in respiratory function through joint mobilization and therapeutic exercises in patients with neck pain due to FHP, but there is need for extra respiratory muscle training to sustain the improvements. Although this study reported GRC scores that suggest that improvement was seen after the intervention in every participant, the mobilization group showed higher GRC that was statistically significant different from that in the exercise group. In this study, 73.3% participants of the mobilization group received over
The results of this study show that the correct posture of the cervical spine and thoracic spine is important when using touchscreen smartphones; consequently, clinical treatments including the cervical spine and thoracic spine should be applied. The most important limitation of this study is the small sample size and the short-term follow up of only 6 weeks. Although the sample size was calculated by calculating the effective size based on a previous study, it is difficult to generalize the study results to all patients with neck pain from FHP. Moreover, there was no control group in this study, the natural change over time and the placebo effect could not be identified. Future studies should consider long-term follow up and a bigger sample size with a multicenter randomized clinical trial design.
Conclusion
This study demonstrated that individuals with FHP who received a combination of upper cervical and upper thoracic spine mobilization indicated better overall short-term outcomes, in terms of CVA, NPRS, respiratory function, and GRC, than individuals receiving DCFE. Future studies should investigate the effectiveness of different types and dosages of manual therapy and include long-term follow-up data collection.
Footnotes
Acknowledgments
The authors would like to thank DK Seo and WT Kim for their participation in the data collection process of this study.
Conflict of interest
The authors declare that they have no competing interests.