
Abstract
BACKGROUND:
Problems related to ankle instability, decreased proprioceptive sensation, altered static and dynamic balance abilities are suggested as major representative factors that contribute to the recurrence of ankle sprains.
OBJECTIVE:
To assess the effect of a three-week intervention (intervention emphasizing diagonal eccentric contraction (IEDEC) and intervention of general exercise (IGE)) on static and dynamic balance abilities, ankle strength and joint position sense at pre- and post-intervention, and at two- and three-week post-intervention.
METHODS:
Twenty-five participants with ankle instability, including a history of ankle sprain and recurrent episodes of giving way, were enrolled in the study. They were randomly classified into the IEDEC group (
RESULTS:
The results revealed significant increases in ankle dynamic stability and strength at two and three weeks post-intervention (
CONCLUSION:
General balance training with IEDEC improved the position sense of the inversion. Combined therapeutic intervention, such as with the manual technique, could be a beneficial approach to maximize the treatment effects.
Keywords
Introduction
The lateral ankle sprain is one of the most common injuries associated with physical and sports activities [1, 2]. Of patients with latera ankle sprains, 20%–30% have recurrent ankle sprains, which can lead to chronic ankle instability [2, 3]. Kamiski and Hartsell [3] suggest to classify chronic ankle stability into mechanical and functional ankle instabilities. Mechanical ankle stability is defined as a ligamentous injury, which is identified with a positive sign of talar tilt and anterior draw examination. Functional ankle instability is characterized by subjective feeling of the ankle giving away and decreased functional performance. In addition, instability is also associated with sensorimotor deficits, altered kinematic patterns during gait, and neuromuscular control changes [3, 4].
Problems related to functional ankle instability, decreased proprioceptive sensation, altered static and dynamic balance abilities, and decreased neuromuscular control are suggested as major representative factors that contribute to the recurrence of ankle sprain [5]. Therefore, several previous studies have investigated variations of interventions for regaining the balance ability and proprioceptive sensation around the ankle joint, as well as strength of the para-ankle muscles [3, 5, 6]. Balance training with one leg stance could be a useful method to enhance the position sense of the ankle [7]. Ha et al. also reported that a strengthening exercise program on an unstable surface is effective for increasing the balance ability of subjects with ankle instability [6]. Because the previous literature mainly evaluated the utilization of exercise programs without manual contact, the effect of exercise with manual contact on recovery of the ankle instability should be investigated.
During therapeutic intervention, manual contract is used for various purposes. According to clinical literature, manual techniques are used for guiding diagonal motion of the targeted joint, and providing appropriate resistance which facilitates functional movement [8]. The induced diagonal motion and contraction of the muscles effectively improved muscle strength as well as proprioceptive sensation of the targeted joint. Because the deficits of patients with ankle instability are associated with impaired proprioceptive sensation and decreased muscle strength, these kinds of interventions might be appropriate for subjects with ankle instability [9].
The present study is not the first to investigate the effectiveness of the interventions that emphasize manual techniques. Hall et al. [6] already reported the positive effects of administering proprioceptive neuromuscular facilitation (PNF) strengthening techniques. However, the study only included reversal techniques inducing concentric contraction of the agonist and antagonist muscles. Because a recent finding emphasized the sensory-targeted exercise protocol [9] and eccentric contraction for subjects with ankle instability [10], the effect of manual techniques emphasizing eccentric contraction on subjects with ankle instability should be investigated. In addition, it is necessary to compare the effects of these interventions. Therefore, the present study aimed to explore the effect of interventions that emphasize eccentric contraction on the strength, proprioceptive sensation, and balance ability in subjects with ankle instability.
Materials and methods
Subjects
The present study included subjects with ankle instability who were recruited from a local hospital and sports center of a local university. The subjects had a history of ankle sprains within three months prior to participation. Inclusion criteria were: (1) history of at least one significant ankle sprain within three months, (2) score of
Demography of subjects (
25)
Demography of subjects (
IEDEC: Intervention Emphasizing Diagonal Eccentric Contraction. IGE: Intervention of General Exercise. CAIT: Cumberland Ankle Instability Tool. FAAM: Foot and Ankle Ability Measure.
The present study was performed as a repeated measure design to investigate the effects of a three-week exercise intervention on individual balance, position sense, and ankle strength in subjects with ankle instability. Identifying exercise effectiveness, the within-subject factor was set as times of follow up, and the intra-subject factor was set as two exercise variations.
Dynamic balance was examined using the Y Balance Test, and the static balance was evaluated using the total displacement of the center of pressure (COP) by using the plantar pressure measurement device (BT-4, HUR Labs, Finland). The Y Balance Test is a functional test that quantifies dynamic balance, which is summarized from the Star Excursion Balance Test. A previous study reported that the intra and interreliability for the normalized Y Balance Test was 0.99 to 1.00 for intra-rater reliability and 0.85 to 0.91 for inter-rater reliability [14, 15]. To measure dynamic balance, the participants were asked to reach as far as possible with their contralateral limb in the anterior, posterolateral, and posteromedial reach directions. The participants placed their big toe at the zero point of a tape measure, whereas the posterolateral and posteromedial directions required the participant to place their heel on the zero point [12]. The furthest point of the contralateral foot that touched the tape was recorded for further analysis. Each participant could practice the movement four times for each direction before measurements. Three trials were performed randomly, of which the mean in each direction was used for data analysis. A Y balance composite score was determined by calculating the mean of the three reach directions [12]. The reach distances were normalized to the limb length (anterior superior iliac spine to the ipsilateral distal medial malleolus) and represented as a ratio [15]. To measure static balance, each subject stood on the plate (BT-4, HUR Labs, Finland) in the one-leg stance with the eyes closed. Measurement was performed during an 11s period, and the data for the first and last three seconds of the period were eliminated [16]. The total displacement of COP was used for further analysis.
The measurement technique of the joint position error was based on previous research. The subjects were seated on the edge of a table with the ankle in an unsupported and relaxed position. For passive testing, the participant’s foot was first passively moved to maximal inversion or eversion, and then moved to 5
The four-way ankle strength was measured by a handheld dynamometer (Commander Muscle Tester, JTECH Medical Inc., USA), which includes dorsiflexion, plantarflexion, inversion, and eversion. Test procedures for measuring muscle strength ere in accordance with previous clinical literature [18]. The averaged value from the two trials were standardized by the weight of each subject, by a method used in previous studies [19]. A pilot study revealed that the intra-tester reliability was 0.84 (95%CI 0.61–0.95) for the dorsiflexion 74 (95%CI, 42.92) for plantarflexion, 0.77 (95%CI 0.48–0.93) for inversion, and 0.81 (0.56–0.95) for eversion.
In the present study a three weeks intervention was conducted emphasizing diagonal eccentric contraction (IEDEC) and intervention of general exercise (IGE). The evaluation of the static and dynamic balance abilities, ankle strength, and joint position sense were performed at pre-test, post-test and two and three-weeks post-intervention. The subjects in the IGE group trained the involved limb [20]. Specifically, the program consisted of a progressive form of exercise with the eyes open and closed conditions, including one-leg standing on a stable surface, one-leg standing on an unstable surface, maintaining normal posture, and maintaining posture while throwing a medicine ball. The program lasted for three sessions per week for three weeks (3*3). Each session lasted for 20 min, there were a total of nine sessions, and 180 min of general exercise were performed under supervision (Fig. 1).
Demonstration of the general balance training (A, B, C). A: Maintaining standing balance with and without eyes open. B: Maintaining standing balance on an unstable board with and without eyes open. C: Maintaining standing balance on an unstable board with throwing the ball.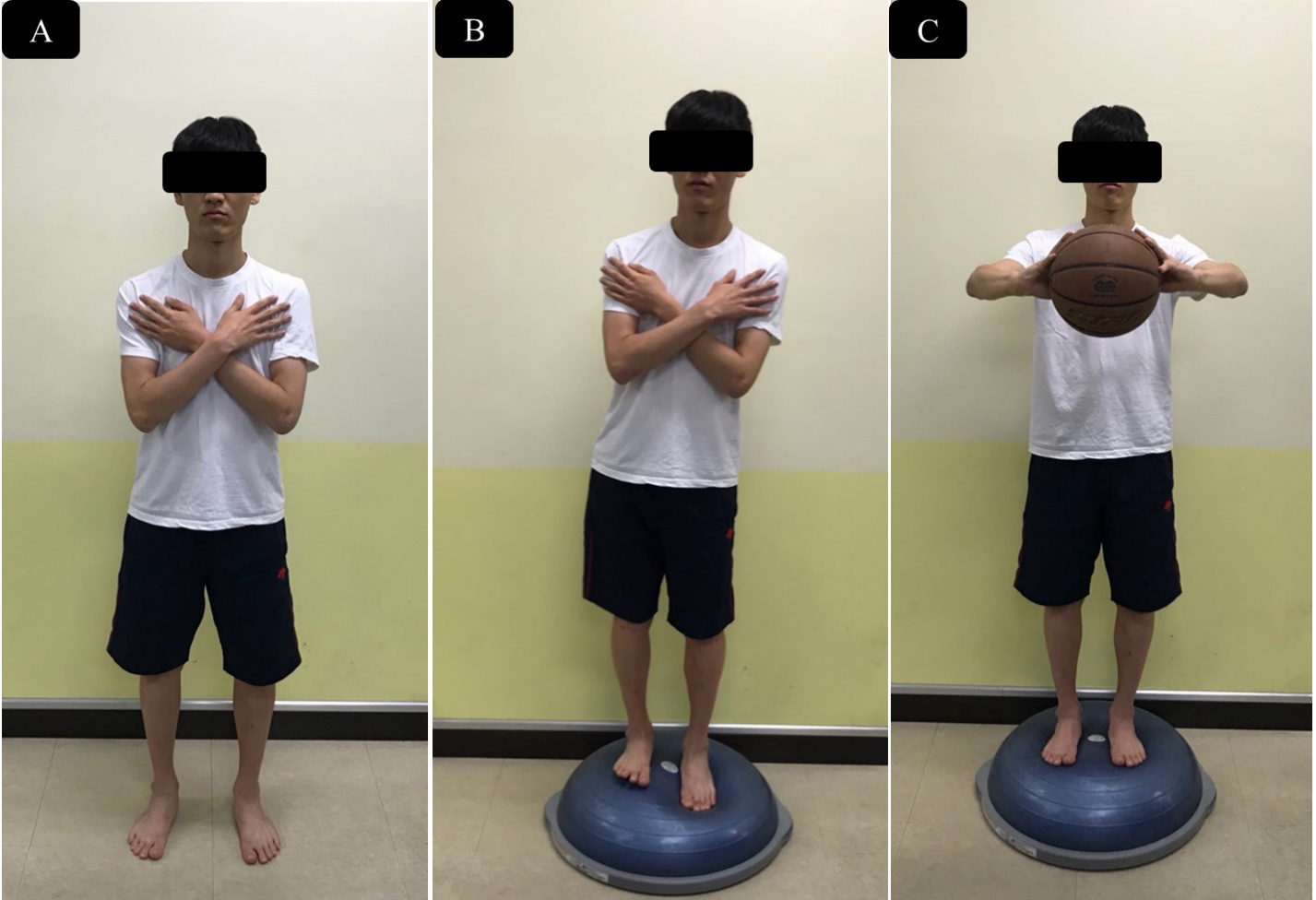
Demonstration of the PNF intervention (A, B). A: Application of the combination of isotonic contractions. The subject slowly moved to plantarflexion and inversion of the ankle resisting the therapist’s force. B: Application of rhythmic stabilization. The subject maintained the ankle position resisting the therapist’s unexpected diagonal force.
The subjects in the IEDEC group also performed three sessions per week for three weeks (3*3). Each session lasted for 20 min, there were a total of nine sessions, and 180 min of intervention was performed with the primary researcher. However, the component of the program was different than the general exercise group. Each subject performed 10 min of general exercise mentioned above and received 10 min of intervention provided by the therapist. Two manual techniques were administered in the intervention. One technique involved combinations of isotonic contraction, emphasizing the eccentric and concentric contractions of the targeted muscle. The other technique involved rhythmic stabilization, where the subject held the joint position against the resistance provided by the therapist [8].
The Y balance ratio, ankle strength, total displacement of the COP, and joint position error data were used for the statistical analysis. The PASW Statistics (version 18.0; SPSS, Chicago, IL, USA) was used to determine significant differences between measurement and exercise variations. Normal distribution data were evaluated using the Kolmogorov-Smirnov test. The two-way repeated analysis of variance was used to identify the significance of the factor of time and exercises. In all analyses,
Results
Regardless of the exercise variations, the Y balance ratio data showed significant differences as a factor of time, with it being higher at two and three weeks compared with the initial pre-test (
Both interventions significantly elevated ankle str-ength (
The joint position error of inversion showed a significant difference with the type of intervention and time (
Discussion
A previous study suggested that balance training can reduce ankle instability symptoms [5]. However, better exercise protocols are continuously being developed, particularly focusing on proprioceptive sensory stimulation [10]. The proprioceptive neuromuscular facil-
| Variables | IEDEC group | IGE group |
|
|||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Pre | Post | Two-week | Three-week | Pre | Post | Two-week | Three-week | Time | Exercise | |
| Y-BT (%) | 79.28 9.09 | 82.54 9.05 | 88.05 9.05 | 90.82 6.07 | 77.49 11.85 | 78.52 9.89 | 87.27 4.16 | 88.00 4.92 | 0.00* | 0.31 |
| Total COP | 421.81 91.91 | 380.66 78.18 | 334.37 71.22 | 284.06 54.65 | 389.64 93.06 | 367.44 102.35 | 317.28 79.36 | 306.09 73.53 | 0.00* | 0.68 |
| displacement | ||||||||||
| (mm) | ||||||||||
| JPE-Inv ( |
6.08 |
3.92 |
3.50 |
3.67 |
4.92 |
5.38 |
5.85 |
5.77 |
0.00* | 0.14 |
| JPE-Ever ( |
4.75 |
4.83 |
4.42 |
4.83 |
5.00 |
6.92 |
6.15 |
7.08 |
0.12 | 0.06 |
Descriptive statistics of 4-way ankle strength following time and exercise variations
itation approach is classically developed for patients with neurological diseases [8]. Therefore, manual techniques emphasize the sensory stimulation while considering functional movement. Despite the fact that this approach is appropriate for subjects with ankle instability, only a few studies have evaluated its efficacy in such cases [9, 21]. Hall et al. [9] suggested that the exercise protocol using the dynamic reversal technique was effective for increasing strength in subjects with ankle instability. Although dynamic reversal is known as a good technique for recruiting muscles surrounding the joint, the existing clinical literature introduced other stabilizing techniques for enhancing proprioceptive sense [8]. Therefore, the present study investigated the efficacy of the other techniques emphasizing eccentric contraction related to sensory stimulation.
An important finding of the present study was that the balance training with IEDEC improved joint position sense in inversion, compared to that with an isolated balance training protocol. Both interventions increased the static and dynamic balance abilities, but this difference may be significant. Based on a previous study, however, subjects with ankle instability frequently showed decreased position sense in inversion [22, 23]. In addition, impaired joint position sense of the inversion could contribute to decreased functional movement [24, 25]. Although it is difficult to affirm the effectiveness of the IEDEC for the recovery of overall joint position sense of the ankle joint, the intervention is advantageous for enhancing joint position sense of the ankle inversion.
The increased joint position sense in inversion could be explained by two mechanisms. The combination of isotonic contractions used in this study induced the eccentric contraction of the ankle muscles. Excessive ankle inversion and plantarflexion induces lateral ankle sprains; thus eccentric contraction of the dorsiflexor and evertor muscle can be helpful in preventing recurrent ankle sprain [26]. Hanci et al. [27] reported that the eccentric training of the ankle evertor could improve the proprioceptive sense and muscle strength of subjects with ankle instability. Therefore, one of the factors that reduces joint position error in ankle inversion is the eccentric contraction that is enhanced by the combination of isotonic contractions with proprioceptive neuromuscular facilitation techniques. Second, improved muscular co-activation might contribute to the present results. In a recent study related to ankle instability, Sousa [28] reported that patients with chronic ankle instability showed deregulation of ankle antagonist co-activation. This study generated alternating isometric contracting against the resistance provided by the therapist [8]. Rhythmic stabilization techniques have been reported to be effective for preventing ankle joint lesions in soccer athletes [21]. Although the application area is different in the present study, Dionisio et al. [29] also recently reported that the manual technique is effective for enhancing stability. We expected that the stabilizing effects induced by the co-contraction of the surrounding ankle joint muscles were contributors to the present results.
The present results do not suggest that the proprioceptive neuromuscular facilitation intervention must be performed before general balance training. General balance training was effective for increasing the static and dynamic balance abilities in the present study. However, this study simply suggests that the additional exercise protocol based on general balance training helps to maximize the treatment effects in subjects with ankle instability.
This study had several limitations. First, joint position sense was not tested in dorsiflexion and plantarflexion, as those movements are involved in the tested movements, inversion and eversion. Second, exercise intensity could not be corrected for all subjects. Further investigation is necessary to overcome these limitations and further validate our findings.
Both general balance training and general balance training with the addition of IEDEC intervention were effective in increasing static and dynamic balance abilities in subjects with ankle instability. Particularly, general balance training with IEDEC improved the position sense in inversion. Combined therapeutic intervention, such as those with the proprioceptive neuromuscular facilitation technique, could be a beneficial approach to maximize treatment effects.
Footnotes
Acknowledgments
This research was supported by the National Research Foundation of Korea (NRF) grant funded by the Ministry of Science and ICT (No. 2019R1G1A10078 09).
Conflict of interest
The authors have no conflict of interest to report.