
Abstract
BACKGROUND:
Sorensen Test time-to-task-failure (TTF) predicts several low back pain (LBP) clinical outcomes, including recurrence. Because the test is described as a measure of trunk extensor (TE) muscle endurance, LBP rehabilitation programs often emphasize endurance training, but the direct role of TE muscle function on Sorensen Test-TTF remains unclear.
OBJECTIVE:
To assess the discriminative and associative properties of multiple markers of isolated TE performance with regard to Sorensen Test-TTF in individuals with recurrent LBP.
METHOD:
Secondary analysis of baseline measures from participants in a registered (NCT02308189) trial (10 men; 20 women) was performed. Participants were classified by Sorensen Test-TTF as high, moderate or low risk for subsequent LBP episodes, and compared to determine if classification could discriminate differences in TE function. Correlations between Sorensen Test-TTF and isolated TE performance, anthropometrics and disability were investigated.
RESULTS:
Individuals at risk of subsequent LBP episodes had greater perceived disability and fat mass/TE strength ratios (
CONCLUSIONS:
Isolated TE muscle endurance is only one of several factors with similar influence on Sorensen Test-TFF, thus LBP rehabilitation strategies should consider other factors, including TE strength, anthropometrics and perceived disability.
Introduction
Low back pain (LBP) was recently recognized as the number one cause of disability worldwide [1, 2]. Although self-limiting in most cases, LBP is the most common reason for medically-certified sick leave and lost workdays in many countries, with a small fraction of affected individuals experiencing severe, persistent disability [2]. Further complicating this significant health problem is the fact that the vast majority of LBP cannot be attributed to any patho-anatomic cause, and is thus “non-specific,” limiting rational targets for treatment [3]. However, the Sorensen Test has been found to discriminate between those with and without current or previous LBP, and to predict disability 12 months following a subacute episode of LBP [4, 5, 6], suggesting a potential mechanistic link between the Sorensen Test and LBP.
The Sorensen Test [7] is a prone, isometric, position-holding task. Because the test involves maintaining a position until failure (i.e., time-to-task-failure (TTF)), it has been suggested that it is an index of endurance of the trunk extensor (TE) muscles [8, 9, 10]. Thus, the discriminative power of the Sorensen Test is interpreted to indicate that poor TE muscle endurance contributes to the onset, duration, recurrence and associated impairments of LBP [4, 5, 9, 11, 12]. As exercise is one of the most recommended interventions for LBP prevention and rehabilitation [13], categorizing the Sorensen Test as a measure of endurance may influence the design of exercise programs for LBP, which frequently emphasize muscle endurance over strength [11, 14]. Even “core strengthening” or stabilization exercises typically involve high-repetition, sub-maximal activation that is more in line with endurance vs. strength training [15, 16, 17].
However, the demands of the Sorensen Test on an individual may vary widely. For example, for individuals with high trunk mass and weak TE muscles it represents a much more difficult task (greater percentage of maximum capacity) than for those with low trunk mass and strong TE muscles. Indeed, trunk mass has been identified as a negative predictor of Sorensen Test-TTF [18, 19]. Thus, the Sorensen Test might be as much a test of strength as of endurance. Identifying the factors (i.e., strength, fatigability, body mass) contributing to Sorensen Test performance is of clinical interest, as this information could aid in developing interventions aimed at improving test performance. Presumably such programs could also reduce negative sequelae of LBP such as disability, recurrence and, most significantly, the development of chronic LBP. For example, if the Sorensen Test is truly a test of endurance, and this poor endurance contributes to LBP severity, duration, first-time occurrence or recurrence, then strengthening interventions might be of limited use. Supporting this view, one study of exercise in a LBP cohort suggests that high intensity TE muscle training improves strength, but not clinical outcomes, more than low-intensity exercise [20]. On the other hand, a later trial indicates that general aerobic and lumbar-specific exercise programs produce similar improvements in Sorensen Test performance in individuals with chronic LBP [21]. Thus, strength and endurance may both contribute to Sorensen Test performance.
Accordingly, the purpose of this study was to explore the potential contributions of isolated TE strength and endurance to Sorensen Test performance in individuals with a history of LBP via secondary analysis of baseline data from a recently published clinical trial [22]. Because the load on the TE muscles during the test is a function of trunk mass, we also assessed anthropometric factors (e.g., trunk mass, body composition). Finally, psychological variables such as self-efficacy have been found to influence Sorensen Test-TTF [18, 19], so we also measured self-reported disability, which has been shown to be elevated when self-efficacy is low in LBP populations [23, 24]. We used two approaches to evaluate the role of these factors: First, we examined group differences after classifying subjects as being at high, moderate and low risk for subsequent episodes of LBP based on Sorensen Test-TTF to determine if any of the TE muscle or anthropometric parameters could discriminate among groups with clinically-meaningful differences in Sorensen Test-TTF. Second, we directly assessed bivariate correlations between Sorensen Test TTF and these factors to determine the strength of association between them. Although the overall sample was not large, the variety of types of data available were greater than what is available in most studies of Sorensen Test performance in clinical populations. Consistent with an exploratory study, this allowed us to use a broad, if not deep, approach to evaluation. Finally, because of the well-known differences in muscle fatigue between men and women [25], we also conducted exploratory evaluations of sex-associated differences in the data.
Method
Subjects
Thirty-two total participants, ages 18–50 (20 women (W) and 12 men (M)), were recruited for a registered randomized controlled trial (RCT; NCT02308189 [26]) examining the effectiveness of blood-flow restricted exercise for improving trunk muscle function in individuals with LBP. Patients were recruited over a two-year, rolling enrollment period, via methods detailed in the published study protocol [26]. Two participants (both M) were removed from the study after randomization (For CONSORT diagram, see [22]) giving a final study
Participant eligibility is detailed in the published study protocol [26]. Briefly, all participants had recurrent LBP, defined as at least two episodes of LBP in the past year, at least one of which caused restriction of work or leisure activity and were sedentary, per the International Physical Activity Questionnaire [27]. To minimize the effect of pain on testing procedures, subjects were excluded for a current report of
Data collection
Subjects participated in two separate sessions, separated by
Anthropometrics and body composition
Whole body and regional lean and fat mass were assessed by DXA per manufacturer (Hologic Discovery QDR model Series, Waltham, MA, USA) guidelines. For purposes of this study, we examined both total and upper body (UB) fat and lean mass. Total mass was calculated by adding fat and lean mass. Muscle cross-sectional area (CSA) was determined by MRI for the TE and KE. Transverse T-1 weighted spin echo images were acquired on a 0.25 Tesla Esaote G-Scan Brio System (Genoa, Italy) as 10 mm slices between L2 and L5. Separate CSA was calculated for the quadratus lumborum, iliocostalis lumborum/longissimus thoracis and multifidus muscles from an average of three slices obtained from the center of the respective muscles, and then added for total TE CSA. Similar methods were used to determine KE cross-sectional area from MRI of the quadriceps femoris muscle group. For both muscle groups, intramuscular fat (IMF) was measured and subtracted from to give muscle CSA [30].
Pain and disability
Participants completed a series of self-report instruments on pain (a Numeric Pain Rating Scale (NPRS) of 0–10), disability (24-item Roland-Morris Disability Questionnaire (RMDQ)) and movement-related fear (Tampa Scale for Kinesiophobia (TSK)).
Muscle testing
Maximum isometric torque of the KE and TE muscle groups was determined by subjects performing maximum voluntary contractions (MVCs) of the TE and KE (bilateral and unilateral) muscles on MedX Dynamometers (Ocala, FL, USA), designed for the back and knee, respectively. The extensive restraint system of the MedX back extension makes it well suited to isolating the TE muscles and has been found to be reliable for both strength and endurance testing [31]. Analysis of the KE data allowed us to evaluate a potential generalized, systemic impairment of muscle function in the participants. The MedX systems were custom-instrumented with load cells and interfaced with BioPac software, allowing collection of raw torque signal at 500 Hz. Muscle quality for the TE group was calculated by dividing the TE MVC by the fat-corrected TE CSA, as described above. In addition, we use regional lean, total and fat mass data from the DXA measurements to determine the ratios of regional mass to TE strength (MVC).
Participant characteristics
Participant characteristics
The same MedX and BioPac equipment was used to determine isolated muscle TTF for the trunk (TE-TTF) and knee extensors (KE-TTF). The fatigue task involved maintaining a sustained isometric contraction at a target of 20% MVC, a common submaximal fatigue task [25, 32, 33]. As with testing MVC of the TE, the TE-TTF was tested in sitting with the trunk midway between the full flexion and extension range of motion available on the MedX [34]. For KE-TTF, subjects were seated with the knee flexed to 60
Descriptive statistics for subject characteristics are presented as means and standard deviations, unless noted otherwise. Comparisons between women (W) and men (M) were made with unpaired
Results
Participant characteristics and sex differences are presented in Table 1. Generally, the only differences were those related to body and muscle size and muscle strength, which are typically different between W and M.
Sorting participants by Sorensen Test-TTF into groups with high, moderate and low risk for subsequent episodes of LBP resulted in group sizes of 9, 11 and 10, respectively. Analysis of the risk groups by ANOVA revealed trends (
A) RMDQ, B) UB fat mass: TE MVC, C) UB fat mass and D) UB mass (all means 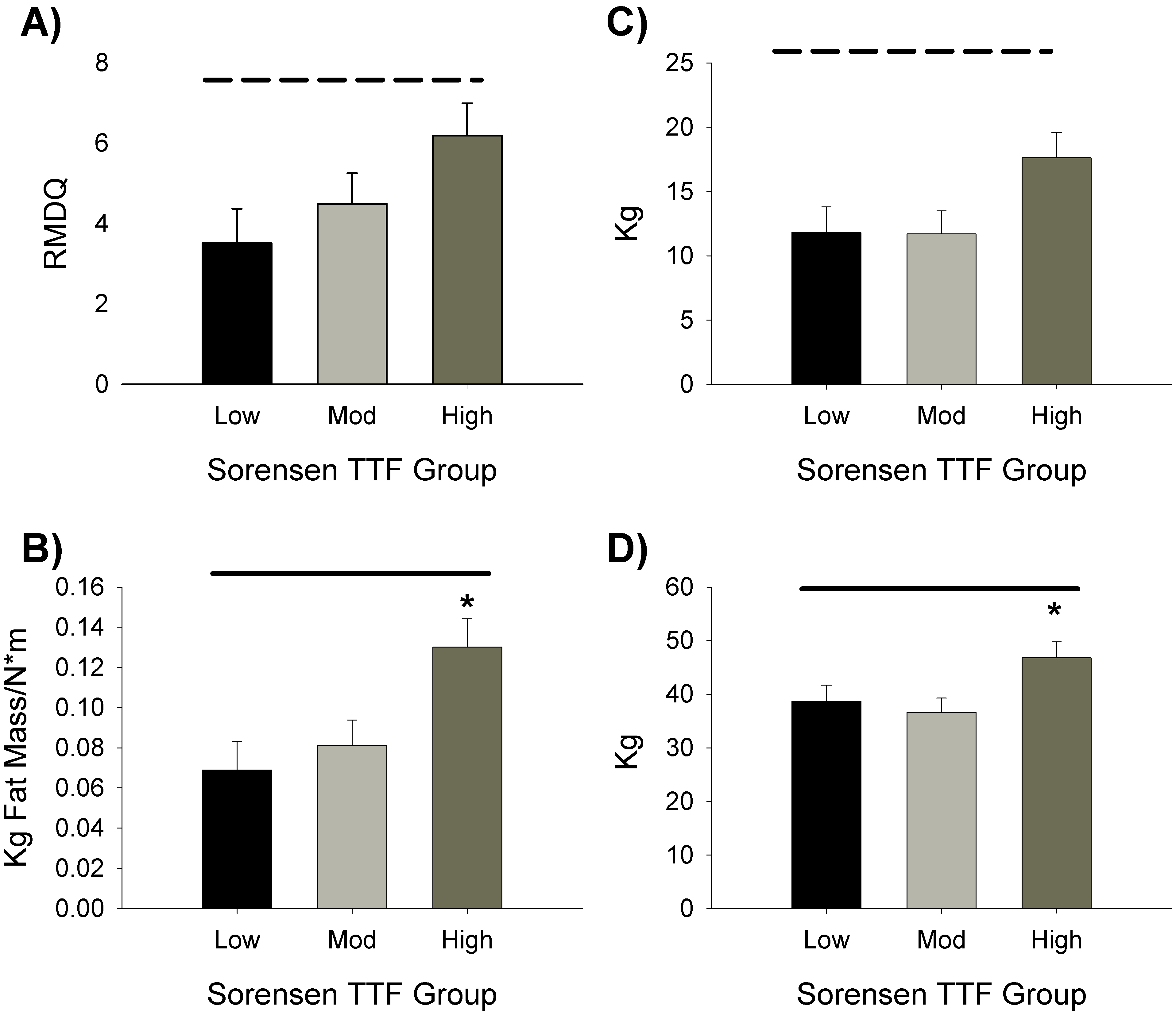
Associations between Sorensen Test-TTF and the muscle, anthropometric, and pain and disability measures are presented in Table 2. Consistent with the description of the Sorensen Test as a measure of TE endurance, TE-TTF was showed a trend for association with Sorensen-TTF, but TE MVC and TE CSA did not. A somewhat more robust, and significant, association between the ratio of upper body fat mass to TE MVC (UB fat mass: TE MVC) and Sorensen Test-TTF was found. Sorensen Test-TTF was also significantly negatively associated with RMDQ, indicating that low Sorensen Test-TTF was associated with greater report of disability. Associations with Sorensen Test-TTF were also somewhat different when W and M were considered separately. Specifically, the ratios of UB total and fat mass to TE MVC were more strongly (negatively) associated with Sorensen Test-TTF in women. In contrast, the negative association between Sorensen Test-TTF and disability was stronger in men, as was the association with KE-TTF. In addition, the association between TSK and Sorensen Test-TTF was qualitatively quite different (i.e., negative in M, but not W), though neither was statistically significant.
Associations with Sorensen Test-TTF
While bivariate correlations did identify significant associations between several parameters and Sorensen Test-TTF, the strength of these associations was only moderate. To determine if a combination of factors could show a more robust relationship, we used stepwise multiple linear regression modeling. Five factors were tested in the model; those found to exhibit at least a trend for an association (Table 2) with Sorensen Test-TTF and sex. All of the factors were retained in the model (
Regression for factors related to Sorensen Test TTF
Weighted for sex. Abbreviations are the same as for Table 1.
Consistent with the description of the Sorensen Test as a test of trunk muscle endurance, isolated TE-TTF, but not isolated TE MVC, exhibited a trend for association with Sorensen Test-TTF [8]. Others have also reported associations between TE endurance, but not strength, and Sorensen Test-TTF in healthy individuals, though these involved isokinetic TE testing [35, 36]. The present study builds upon these earlier works by evaluating a LBP population and by addressing body composition and anthropometrics. Indeed, while isolated TE MVC was not associated with Sorensen Test-TTF, a significant association was present for the UB fat mass: TE MVC ratio. This finding is consistent with our recent studies reporting that trunk mass is a significant contributor to Sorensen Test-TTF in individuals with recurrent LBP [18, 19]. Moreover, the strength of association between Sorensen Test-TTF and UB fat mass: TE MVC was greater than that seen for TE-TTF, and achieved the threshold of statistical significance. These findings indicate that the Sorensen Test is at least as much of a test of TE strength (or relative strength) as one of endurance. Thus, TE exercise programs for prevention or rehabilitation of LBP should ideally target both muscle endurance and strength and possibly be weight. We base this on the observations that ratio of TE strength to upper body fat mass and TE-TTF were independent contributors to Sorensen Test-TTF (Table 3) and were not correlated with each other. These associative findings were confirmed when testing for differences among groups of individuals classified by Sorensen-TTF as being at different levels of risk for subsequent episodes of LBP (Fig. 1). Again, the effect of UB fat mass: TE MVC ratio, but not TE-TTF, was significant. In addition, several other measures of upper body mass and relative strength also discriminated among the groups. This could indicate that, while isolated trunk endurance contributes to Sorensen Test-TTF, TE strength relative to upper body composition and mass is a more important factor in the risk for LBP. Further studies designed to specifically test this hypothesis are warranted, as they could direct the focus of interventions aimed at rehabilitation and prevention of LBP. In particular, larger studies targeting the muscle performance parameters related to Sorensen Test-TTF are needed to determine if improvements in these factors can reduce disability and improve clinical outcomes in different LBP populations.
The RMDQ has been found to be an important predictor of long term outcomes, including return to work, in individuals with LBP [37, 38]. We observed a significant negative association between Sorensen Test-TTF and self-reported disability per the RMDQ, consistent with that reported for other measures of disability [12]. Although our study group did not have high ratings of disability or current pain, there was also significant main effect of Sorensen Test-TTF classification on RMDQ score. Moreover, the difference between the high- and low-risk groups was within the range of minimal clinically important differences for RMDQ [39, 40]. We have recently found that self-efficacy contributes significantly to Sorensen Test-TFF [18, 19]. Our finding that RMDQ predicted Sorensen Test TTF is consistent with these findings, as it has been reported that greater disability is associated with both pain- and exercise-related self-efficacy [23, 24]. Interestingly, Sorensen Test-TTF was significantly associated with RMDQ, neither TE-TTF nor strength were. It might be that Sorensen Test-TTF is driven by perceived disability, directly or mediated via self-efficacy, rather than low Sorensen Test-TTF reflecting physical impairments that contribute to perceived disability. Nevertheless, the present findings do support the reported discriminative and prognostic properties of the Sorensen Test related to LBP [4, 5, 6].
Finally, because W frequently exhibit less muscle fatigue than M (for review, c.f., [25]), including during the Sorensen Test [41], we explored the data for sex-specific differences, though the study was not specifically designed for this. No significant differences between W and M for either Sorensen Test- or TE-TTF were observed, though slightly greater (
These sex-related differences should be viewed cautiously, as this study was not specifically powered to assess sex-related differences and the sample contained twice as many W as M. These data support no definitive conclusions regarding sex-specific mechanisms contributing to Sorensen Test-TTF performance. However, the observed differences are intriguing enough to warrant further specific investigation. If confirmed, such differences could suggest that interventions for LBP may need to vary depending on sex of the patient. For example, a rehabilitation program involving a general increase in activity might be sufficient for men, whereas programs for women might benefit from the inclusion of TE-specific exercises.
In addition to the limitations related to sex-specific analyses, other limitations of the study must be acknowledged. First, this was a secondary analysis of an RCT. Sample sizes were not optimized for the specific analyses of this study; thus results should be viewed as preliminary. The patient population was narrowly defined and may not reflect other LBP groups (e.g., chronic or acute LBP), with differing levels of pain or disability. Methodologically, the similar relationship between MVC and CSA in the KE muscle group (
Conclusions
The expected association between Sorensen Test-TTF and isolated TE-TTF was observed, but other factors exhibited comparable associations with Sorensen Test-TTF, suggesting the test represents a more global assessment of TE muscle performance than a simple index of endurance. Consistent with this view, a regression model incorporating TE-TTF, TE strength relative to fat mass and RMDQ score explained 56% of the variance in Sorensen Test-TTF. Intriguing differences in M and W that could potentially direct sex-specific intervention strategies were suggested by exploratory analyses.
Footnotes
Acknowledgments
The authors thank Rachel Clift for providing study coordination and management and Kwasi Ampomah for assistance with data processing. Portions of these data have been presented in abstract form at the 2019 Combined Sections Meeting of the American Physical Therapy Association. This work was supported, in part, by a grant from the National Institutes of Health (NIAMS R21AR063909 to Brian Clark).
Conflict of interest
Brian Clark has received research funding from the National Institutes of Health, Regeneron Pharmaceuticals, Astellas Pharma Global Development, Inc., RTI Health Solutions, Ohio Department of Higher Education, and the Osteopathic Heritage Foundations. In the past 5 years Brian Clark has received consulting fees from Regeneron Pharmaceuticals, Abbott Laboratories, and the Gerson Lehrman Group. Additionally, Brian Clark is co-founder with equity and scientific director of AEIOU Scientific, LLC. In the past five years, David Russ has received research funding and consulting fees from Abbott Nutrition. The other authors declare no conflicts of interest.