
Abstract
BACKGROUND and OBJECTIVE:
Caring for a child with a disability affects musculoskeletal system pain, fatigue, sleep quality, and anxiety of the mothers. The purpose of the study was to determine the effectiveness of breathing exercises in mothers with chronic non-specific low back pain (NLBP).
METHODS:
Forty-three mothers with chronic NLBP were randomly assigned to the experimental group (
RESULTS:
After the treatment programs, significant differences were observed in pain, fatigue, and sleep quality in both groups (
CONCLUSIONS:
The improvements in pain, fatigue and sleep quality were seen in both groups after treatment programs. It is recommended breathing exercises are added to core stabilization programs to provide greater improvements in anxiety level and sleep quality for mothers of children with disabilities, who have NLBP.
Introduction
Children with special healthcare needs (SHCN) are defined as those “who have or are at increased risk for a chronic physical, developmental, behavioral, or emotional condition and who also require health and related services of a type or amount beyond that required by children generally” [1]. Children with SHCN may have physical, intellectual, and developmental disabilities that require lifelong health-related services to improve and maintain the quality of their health. One of these services is the family support service provided by the parents of children with SHCN. The care of children with SHCN is a difficult and lifelong process for the parents.
The well-being of the parents, including physical, emotional, and behavioral aspects is essential for them to be able to provide continuity of care for children with SHCN [2]. The mothers of children with SHCN, who play a major role in their children’s life, have significant roles in the management of their children’s health. The provision of long-term childcare can affect both the physical health and the psychological well-being of mothers of children with SHCN. These mothers have been found to be more anxious than other members of the family, experiencing problems such as physical problems, insomnia, anxiety, fatigue, and disruption of their personal care [2, 3, 4]. Sleep problems, including poor quality of sleep, have been reported to be common among mothers with children with SHCN, including those with physical disabilities [4, 5]. In addition, mothers of children with developmental disabilities have higher anxiety levels [6]. Prolonged fatigue, poor sleep quality and anxiety affect the physical health of the mothers. Musculoskeletal disorders, most commonly LBP, are more common in the mothers of children with SHCN, as a result of repetitive lumbar flexion movements of mothers and incorrect posture while carrying the child [7, 8, 9].
Studies have shown differences in breathing during a lifting task in individuals with LBP and healthy individuals [10]. Changes in breathing patterns and diaphragm mechanics have been reported in individuals with chronic LBP [11]. Previous studies have also shown the relationship between poor core stability and back pain and have emphasized the need to strengthen the core muscles. Core stabilization exercises prevent degenerative problems by minimizing the load on the structures in the active and passive subsystems. Furthermore, they are effective in reducing pain and fatigue, thereby enabling better coping with anxiety and improved sleep quality [12, 13, 14].
Breathing exercises, such as diaphragmatic and pursed-lip focusing on awareness of breathing patterns, rate, and volume, have been shown to have the same effect as traditional physiotherapy for LBP patients [15]. These exercises have advantages over the conventional therapies currently used to treat anxiety problems [16]. Diaphragmatic breathing is particularly effective in reducing anxiety, perception and symptoms, and pursed-lip breathing controls the respiratory rate and depth, resulting in relaxation and a reduction in feelings of panic [16, 17]. Diaphragmatic breathing exercises provide maximum benefit to individuals, and can be used as an effective relaxation technique if they are applied together with pursed lip respiration [17, 18, 19].
To the best of our knowledge, no studies in the literature have examined the effects of rehabilitation and supportive stabilization and breathing exercises on problems such as fatigue, anxiety, poor sleep quality, and musculoskeletal disorders of mothers of children with SHCN. The hypothesis of this study was that core stabilization exercises combined with diaphragmatic and pursed-lip breathing exercises might have a positive effect on the physical health and psychological well-being of mothers of children with SHCN. Therefore, the aim of the study was to evaluate the effects of core stabilization exercises combined with diaphragmatic breathing and pursed-lip exercises on pain, fatigue, anxiety level, and sleep quality of mothers of children with SHCN.
Materials and methods
Subjects
This study was a randomized controlled trial. The mothers of the children with SHCN were recruited from the pediatric rehabilitation center in Batman, south-east Turkey. This is a major rehabilitation center in this region providing rehabilitation services for children aged 3–14 years. A total of 60 mothers attending the center for childcare rehabilitation services and who also had chronic, non-specific low back pain (NLBP) were invited to participate in the study.
The inclusion criteria for the mothers of the children with SHCN were defined as: primary caregiver of the child; suffering from LBP for at least three months; positive in
CONSORT flowchart.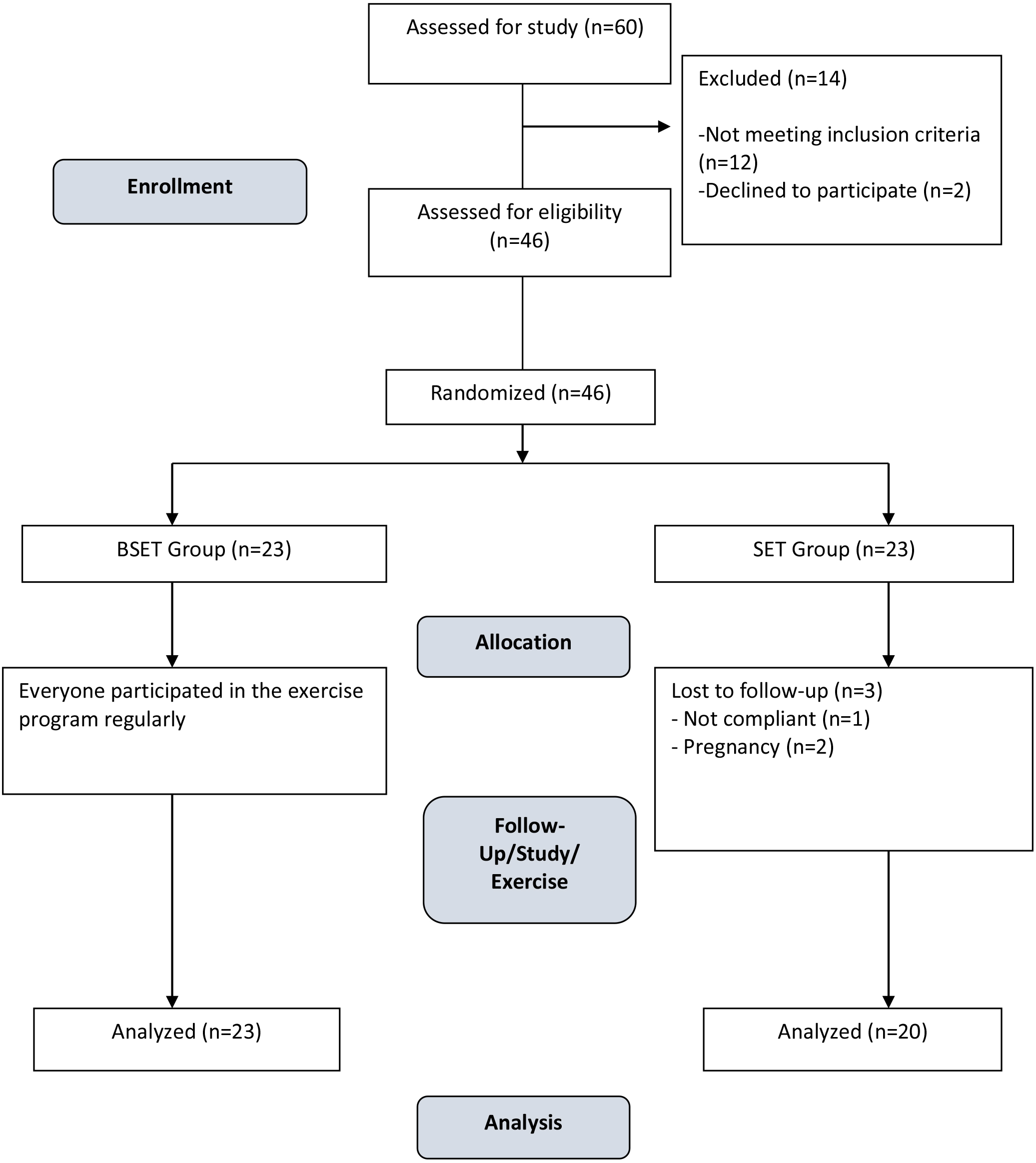
Core stabilization exercises.
In this randomized control trial, selection screening of the mothers was applied with lumbar instability testing consisting of: 1. Positive prone instability test, in which the subject lies prone on a table with the feet on the floor. Posterior-to-anterior pressure (P/A) is applied to the spinous processes of the lumbar spine, and any painful provocation is recorded. Then the subject actively raises both legs from the floor and P/A pressure is again applied to the spine. If pain is present in the resting position but subsides in the second position, the test is positive; 2. Lumbar P/A mobility test: with the subject in prone position, pain and/or excessive or hypermobile movements when pressure is applied is accepted as positive; 3. Passive straight leg raise test exceeding 90
Of the 60 mothers of children with SHCN who were initially enrolled, 14 were excluded because they did not meet the inclusion criteria for the following reasons: The results of the instability test were negative in 12, insufficient time to commit to a regular exercise program in 1 case, and pregnancy in 1 case. Thus, a total of 46 mothers met the inclusion criteria and were separated into two groups using the simple randomization method based on a computer-generated table of random numbers.
Exercise protocol
A total of 46 mothers were enrolled in the study and randomly assigned to one of the two groups; the Breathing Exercises plus Stabilization Exercises Therapy (BSET) (
The mothers in the experimental group received stabilization exercises with breathing exercises 3 times a week for 8 weeks, while the mothers in the control group received only stabilization exercises for the same period of time. Both groups were informed before the program and encouraged not to make changes to their regular exercise and activities.
The 8-week stabilization exercise program was completed without any incident. Each exercise session lasted approximately 60 minutes and was performed 3 days per week, for 8 weeks. All mothers in both groups performed 15 minutes warm-up stretching exercises prior to the core exercises and 10 minutes cool-down exercises at the end of each session. All exercises were performed under the supervision of the qualified and experienced physical therapist (E.D.A).
Breathing exercises
The BSET group received breathing exercises before the stabilization exercise program. At the beginning of the study, a one-hour theoretical training session was provided about the techniques of diaphragmatic and pursed-lip breathing. Almost all mothers were observed to have chest breathing prior to theoretical training about diaphragmatic and pursed-lip breathing. During the diaphragmatic breathing, attention is focused on correct abdominal breathing, keeping the shoulders and shoulder girdles, neck and face muscles relaxed while breathing deeply without movement in the chest. Pursed-lip breathing is one step further than diaphragmatic breathing. After inhalation through the nose and moving the air to the abdomen, the breath is held for two or three seconds, then exhaled slowly and deliberately through the lips, which are contracting as if blowing out a candle. Pursed-lip breathing is a technique designed to provide control over the time and volume of breathing [17, 18, 19].
The patients were instructed to do the breathing exercises while they performed the stabilization exercises, so that the patients focused on their breathing cycle, time and movement, while doing the stabilization exercises.
Stabilization exercises
The first stage of treatment was patient education. All the mothers in both groups were given a one-hour training session about the concepts of stabilization and abdominal bracing before starting the study. The motor control tests for the local muscles, the transversus abdominus (TA) and multifidi, were performed after the training session. The abdominal bracing test was performed in the quadruped position, prone, and in the hook lying position with the patient’s supine, and hips and knees flexed, with feet flat in contact with the surface [13, 21, 22]. Activation of the muscles was assessed using the Stabilizer Pressure Biofeedback Unit (PBU, Chattanooga Group, Australia). The PBU consists of a combined gauge/inflation bulb connected to a pressure cell. It is a simple device that registers changing pressure in an air-filled pressure cell, allowing body movement, especially spinal movement, to be detected during exercise [23, 24]. When patients can demonstrate proper activation of the TA and multifidi during the initial exercises for the improvement of neuromuscular control of the local muscles and joint stabilization, they can then progress to second stage exercises. The second stage consists of closed-chain segmental control exercises. This is a series of weight-bearing exercises performed on stable then unstable surfaces. The last stage of the stabilization program is an open kinetic-chain exercise to promote distal stability [25, 26]. The physical therapist made the decisions for progression to the next stage based on continual assessment of the motor control tests.
The sociodemographic data of the participants (age, height, weight, income, and education level) were recorded together with the number of children and the diagnosis which necessitated SHCN. The outcome measures for both groups were assessed before and after the 8-week exercise training program. The physical therapist who assessed the mothers of children with SHCN was not blinded.
Evolution tools
Visual Analog Scale (VAS)
The pain level was assessed with VAS. The VAS is a 10 cm-long horizontal line with verbal descriptors (word anchors) at each end to express the extremes of the feeling. Complaints of pain developing in 5 regions of the body (back, neck, shoulders, elbows, and wrist-hands) were questioned and marked by mapping on the scale and thus the presence of pain was recorded. The patients were asked whether pain that had developed within the last year had prevented them from doing normal work in daily life or whether hospitalization had been required due to this pain [27].
Fatigue Severity Scale (FSS)
This scale is a 9-item self-administered instrument which was developed in 1998. The FSS was applied to determine the fatigue levels of the mothers included in the study during the last 1 month. A score of
Spielberger’s State-Trait Anxiety Inventory (STAI)
The anxiety level of the mothers in the study was assessed using the State-Trait Anxiety Inventory (STAI), developed in 1970 by Spielberger, Gorsuch and Lushene [30]. The inventory consists of two scales, state anxiety and trait anxiety, both of which include 20 items with responses on a 1–4 scale, in the areas of worry, tension, apprehension, and nervousness. The range of possible total scores is 20–80, with higher scores indicating higher levels of anxiety. The Turkish version of STAI was used in this study [31].
Pittsburgh Sleep Quality Index (PSQI)
The sleep quality of the mothers was evaluated using the PSQI, which consists of a total of 24 items, 19 of which are self-rated and 5 of which are answered by the partner or room-mate of the subject. The total score ranges between 0 and 21 points with higher values representing worse sleep quality. Based on the total score, sleep quality is rated as good (0–5 points) or poor (6–21 points) [32]. In this study, a total of 24 questions were answered by the mothers of children with SHCN. The Turkish version of PSQI was used for the evaluation of sleep quality of the mothers [33].
Approval for this randomized controlled trial was granted by the Human Research Ethics Committee of Hasan Kalyoncu University (decision no. 2018-05). All study procedures conform to the provisions of the Declaration of Helsinki. Written informed consent was obtained from all participants.
Statistical analysis
Power analysis to calculate the sample size, was applied using G-power 3.19 software. A moderate effect size (effect size
Results
Evaluation was made of a total of 43 mothers who completed the study in the BSET or the SET group. At baseline, no statistically significant differences were found between the groups for all dependent variables. For the sociodemographic variables, with the exception of age, the groups were similar. The age of the mothers in the BSET group was slightly younger than that of the mothers in the control group. The sample baseline characteristics of both groups are shown in Table 1.
The baseline characteristics
The baseline characteristics
Diagnosis of children with physical disabilities
The diagnoses of the children requiring SHCN in both groups were determined as mostly cerebral palsy (CP), followed by Down’s syndrome, developmental retardation, and spina bifida (Table 2). The vast majority of the children had been diagnosed and started rehabilitation within the first year of life and had been receiving rehabilitation for a period of 3 years or longer. In both groups, the vast majority of the mothers had been actively involved in the care and rehabilitation of the child for 3 years or longer. More than half of the mothers in both groups spent 12 hours or more per day caring for the child (Table 3). All of the mothers had complaints of musculoskeletal system pain, followed by fatigue, sleeplessness, and lack of time for themselves (Table 4).
Time spent in rehabilitation and time spent by the mothers caring for their children
Types of complaints from mothers
Comparisons within and between the groups before and after the treatment
Both groups showed statistically significant differences in FSS, and PSQI for pre- and post-interventions (
Although it has been reported in the literature that mothers of children with disabilities develop problems over time such as fatigue, anxiety, poor sleep quality, and chronic musculoskeletal system pain [3, 6, 7, 8, 9], no studies on rehabilitative and supportive exercise therapies for mothers have been performed to eliminate these problems. From a review of the literature, only a few studies were found [38, 39, 40] that compared the effectiveness of breathing and stabilization exercises on LBP patients. There was no evidence of the effects of breathing exercises on a population of mothers with NLBP, who are caring for a child with SHCN. The aim of this study was to evaluate the effect of breathing exercises on mothers suffering from NLBP, and to assess the effectiveness of the breathing exercise in addition to the stabilization treatment. The study results suggest that the use of breathing exercises in addition to a stabilization program is more effective than stabilization alone. Both groups obtained better results in musculoskeletal pain and fatigue when compared with the baseline after 8 weeks, but major changes occurred in the BSET group. The findings from the present study suggest that the practice of breathing exercises in addition to a stabilization program improved the anxiety and sleep quality scores of the mothers with NLBP more than stabilization exercises alone in a period of 8 weeks.
All the mothers in the study assumed full responsibility for the care and rehabilitation of their children with physical disabilities, and 56.5% of the mothers in the BSET group and 50% in the SET group stated that they spent 12 hours a day or more caring for the child. Thus, the majority of the mothers were spending half or more of each day involved with the care and rehabilitation of the child, and therefore experienced some difficulties and problems. When the mothers were questioned about their complaints, the most common complaints reported were musculoskeletal system pain, fatigue, listlessness and sleeplessness, and pain had been ongoing for longer than 3 months.
Regular exercise has been reported to have a positive effect on muscle strength, the physiological system of the body, and general health, and to reduce pain [12, 14, 16]. Previous studies in the literature related to the effect of stabilization exercises on musculoskeletal system pain have generally focussed on lower back pain and these exercises have been seen to be effective in reducing chronic musculoskeletal system pain [34, 35, 36]. Positive effects have also been reported on increasing the ability to cope with stress, depression, and anxiety [37].
To be able to correctly interpret the study results, the etiology of LBP and the effect on respiration must be taken into consideration. Loss of motor control involves failure to control joints, because of the lack of co-ordination of the agonist-antagonist muscle co-activation [25]. Reasons for chronic pain may include altered muscle length relationships, postural changes, muscular imbalances, and variations in location of the centers of mass and of pressure [41]. Panjabi stated that the central nervous subsystem (control), the osteoligamentous subsystem (passive), and the muscle subsystem (active) work together to maintain spinal stability [25]. Anything that interferes with co-ordination can lead to stabilization dysfunction of the trunk muscles, and is related to the alteration of neuromuscular mechanisms, which can produce low back instability and pain [21, 22]. All these changes lead to patients moving differently, compared to healthy individuals. Motor control, as well as muscle activation and co-ordination deficit of these muscles, is considered to be responsible for LBP and weakness, since it impairs the efficient use of these muscle group [14, 26].
Stabilization exercises are physical exercises that promote core strength, motor control and balance [21, 22]. Core stabilisation exercises increase the strength and stability of the lumbopelvic region in functional positions and movements and help in the energy transfer required to create strength in the extremities. Thus, an individual uses the existing energy more economically and becomes less tired.
Furthermore, each step of stabilization exercises can be adapted to the level of physical pain of the subject and can therefore be practiced by a wide range of people regardless of their physical level or age [21, 22, 23, 24]. Diaphragmatic breathing exercises provide a decrease in blood pressure and pulse rate by stimulating the parasympathetic system, and have been reported to lower stress levels and have a sedative effect on the individual [18]. Pursed-lips breathing provides relaxation, helping to control dyspnea and feelings of panic, through the control of the rate and depth of respiration [17]. In addition, diaphragmatic breathing exercises allow the use of the diaphragm, which is the main inspiratory muscle, rather than the auxiliary respiratory muscles during breathing. Thus, when the diaphragm is strengthened, auxiliary muscle activity is reduced and fatigue is prevented by reducing the amount of energy spent on respiration [11, 15, 16, 17, 18, 19].
Studies have pointed out that the breathing of LBP patients is different from that of healthy groups [10, 11, 42, 43]. In an experimental study, Haggings et al. [10] demonstrated that individuals with LBP had greater inhaled lung volume when performing a lifting task compared to individuals without LBP. Those findings are consistent with the theoretical link between breath control, intra-abdominal pressure, and lumbar segmental control. Roussel et al. [42] evaluated the breathing pattern in patients with chronic non-specific LBP and in healthy subjects, both at rest and during motor control tests. The breathing pattern was evaluated at rest and while performing clinical motor control tests, i.e. bent knee fall out and active straight leg raise. It was determined that there were significantly more altered breathing patterns in chronic LBP patients during the motor control tests. It was concluded that changes in breathing pattern during motor control tests were not related to pain severity but were related to motor control dysfunction.
Therefore, the focus for the treatment of chronic LBP patients should include patient education of the correct way to breathe and activate their core muscles. The emphasis of the patient education should be on becoming conscious of and able to control the activation of the core muscles through the performance of various tasks during the treatment sessions. It is also important to insist on the necessity of controlling the activation of these muscles in daily-life activities. This motor learning and muscle reprogramming is believed to be responsible for the beneficial effect of stabilization exercises and learning to control the breathing on posture, pain relief, muscle activation and functional status improvement [24, 25, 26].
Spielberger defined state anxiety as the somatic and emotional reactions which develop against stimuli that are perceived as threatening in a particular situation, and trait anxiety as the tendency of an individual to anxiety, regardless of conditions and situations [30]. According to the results in this study of the evaluations of state and trait anxiety, which are two different types of anxiety with different characteristics, the vast majority of the mothers who were responsible for the care of a child with SHCN experienced some psychological difficulties and problems in addition to physical problems. The high level of trait anxiety is particularly thought-provoking.
While pain is associated with altered breathing patterns, increased anxiety is also caused or aggravated by disordered breathing patterns [19]. Breathing pattern disorders are in turn exacerbated by anxiety and pain. Therefore, another positive aspect of practicing breathing exercises is the positive influence on anxiety. A reduction in anxiety levels may help to improve patient activity. Thus, controlling breathing patterns and learning the correct way to breathe can help to relax and activate the muscles [42, 43]. In the current study, a significant decrease was observed after the 8-week program in all anxiety levels in the BSET group where pursed-lips breathing exercises were applied, and the difference between the groups was statistically significant. Similarly, in a study by Chen et al. [44], a diaphragmatic breathing relaxation (DBR) training program was seen to provide a significant decrease in anxiety level.
Previous studies have shown an association between emotional status and lower back pain. When the literature related to the effect of core stabilization exercises on anxiety levels was examined, it was found that stabilization exercises reduced the lower back pain of patients and there was an associated decrease in levels of anxiety, stress, and depression [36, 37]. In the SET group of the current study, where stabilization exercises only were applied, there was seen to be a significant decrease in VAS-neck, VAS-back, and total FSS and PSQI scores, which reduced the levels of pain and fatigue in the mothers, and improved the quality of sleep. However, in the BSET group, where breathing exercises were applied together with stabilization exercises, significant improvements were obtained in all the parameters and significant differences were obtained especially in the anxiety and sleep quality values of the mothers when compared to the SET group. These findings suggest that breathing exercises have a positive effect on reducing anxiety levels and improving sleep quality.
Based on these results, it can be recommended that therapeutic exercises are provided for the mothers of children with disabilities, who are generally responsible for their care, especially in private rehabilitation centers in the periods when they are waiting while their children undergo treatment. The provision of group exercises, including breathing exercises, which could reduce anxiety, stress, pain and fatigue, and improve the sleep and quality of life of the mothers, would be beneficial.
At the end of the 8-week treatment programs, the positive results obtained in pain, fatigue, anxiety and sleep quality suggest the recommendation of the use of breathing exercises together with stabilization exercise programs for mothers of disabled children affected by CLBP. This study focused on the effectiveness on pain and functional status of adding diaphragmatic and pursed lip breathing exercises to stabilization exercises for mothers with CLBP. The results obtained suggest that the improvements in anxiety and sleep quality in the breathing exercise group were maintained. Nevertheless, further studies on this target population are needed to be able to evaluate the long-term effects and to compare different types of breathing exercise programs and their effects on CLBP.
There were some limitations to this study, primarily that the evaluation methods used were subjective and were only made at baseline and at the end of 8 weeks, so there was no assessment of long-term effects. Another limitation could be that there was a difference between the groups in the mean age of the mothers, despite the randomization applied.
Conclusion
The results of this study showed that breathing exercises seem to present additional benefits for women with CLBP, in comparison to performing stabilization exercises only. Improvements were determined in the group with breathing exercises plus stabilization training in respect of lower anxiety levels and improved sleep quality. Further studies should be performed to assess the long-term results.
Footnotes
Conflict of interest
The authors report no conflicts of interest.