
Abstract
BACKGROUND:
Core stability exercises have been widely advocated for management of patients with different musculoskeletal conditions, even though its effect on postpartum Lumbopelvic Pain (LPP) has not been fully investigated.
OBJECTIVE:
This study was conducted to investigate the effect of core stability exercises on postpartum LPP.
METHODS:
Thirty four women suffering from postpartum LPP were randomly assigned to the study or control group. The control group (
RESULTS:
There was a significant improvement in PPT, VAS and ODI post-treatment compared with the pre-treatment in both groups (
CONCLUSIONS:
Core stability exercises in addition to traditional treatment significantly decreased pain and improved function for women with postpartum LPP.
Introduction
Lumbopelvic Pain (LPP) refers to self-reported pain in areas of lower back, anterior pelvis, posterior pelvis, or any combination of these locations [1, 2]. It is a common complaint for women after labour, and this is supported by a systematic review which found that 25% of newly delivered women experienced low back and/or pelvic pain [3]. Also, it has been reported by postpartum follow-up studies that about 8–20% of women still have persistent non-specific LPP for 2–3 years after delivery [4]. The presence of LPP is often identified and confirmed by diagrammatic representations of self-reported pain location alone or in combination with clinical tests [4, 5, 6, 7, 8, 9, 10, 11], and most LPP is reported in and around the lumbar area, which is responsible for supporting the majority of the upper body weight [12].
Factors associated with LPP occurrence in the postnatal period include maternal age, parity, obesity, smoking, oral contraceptives, previous history of LPP, uncomfortable working conditions, and lack of exercise [9, 13, 14, 15, 16]. Also, non-optimal stability which result from weakening or insufficient motor control of the trunk muscles, is proposed as the most common cause for postpartum LPP [17, 18, 19].
Persistent LPP can negatively impact women’s ability to perform daily activities and quality of life. Among postnatal women it has been shown that LPP leads to sleep problems, depression, fatigue, anxiety and a general inability to do activities that involve carrying or lifting [20, 21, 22, 23]. For instance, Gutke et al. [20] found that women suffering from LPP are three times more likely to experience symptoms of postnatal depression compared to those without LPP. In another study conducted by Gutke et al. [4], 40 % of women with postnatal LPP reported moderate to severe disability with pain intensity being the major explanatory variable for disability level. They also found that the impact of having pelvic girdle pain, combined pain or lumbar pain were equivalent in terms of disability, pain intensity, health-related quality of life, activity level and kinesiophobia.
Different interventions have been used to reduce LPP in general including exercise, acupuncture, drugs, therapies using heat/cold, traction, laser, ultrasound, short wave and massage [24, 25]. An increasingly common approach used within the physical therapy management of Low Back Pain (LBP) and lower extremity pathology is the core stabilization exercises [26], which is a form of training that challenges the stability of the spine while training muscle activity patterns and postures that ensure sufficient stability without unnecessarily overloading tissue [27, 28]. Clinical trials and experimental studies using these types of exercises have shown improved objective and subjective outcomes in specific subgroups of patients with LBP, such as those with radiologic evidence of instability, acute first-episode LBP and pelvic girdle pain [29, 30].
The core as described by Akuthota et al. [31] is a muscular box with the abdominals in the front, paraspinals and gluteals in the rear, the diaphragm at the top, and the pelvic floor and hip girdle musculature at the bottom. The muscles and joints of the hip, pelvis, and spine are located centrally to maintain stability necessary for the limbs to function properly, thus providing the proximal stability required for distal mobility of the kinetic chain [32]. Hence, the main emphasis of core strengthening is focused on muscular stabilization of abdominal, paraspinal and gluteal musculature [33]. Strengthening and neuromuscular reeducation of the core musculature is thought to play a significant role in restoring stability to the spinal column and in turn minimizing pain associated instability [32], which developed partially in response to evidence indicating specific neuromuscular alterations in the control and activation of the back and abdominal muscles in the presence of back pain [34, 35, 36, 37, 38].
Although core stability training has become a popular fitness trend that has begun to be applied in rehabilitation programs [31], up until now the literature was unable to identify any study that investigated the effect of core stability exercises in treating postpartum LPP. Consequently, the purpose of this randomized controlled study was to evaluate the effect of core stability exercises in treating postpartum LPP.
Methods
This randomized experimental trial was conducted at the Outpatient Clinic of the Faculty of Physical Therapy at Cairo University, Egypt, from November 2017 to March 2018. The study protocol was explained in detail to each patient before the initial assessment and enrollment in the study. All patients signed an institutionally approved informed consent form which was approved by the Ethics Committee of the Faculty of Physical Therapy at Cairo University (P.T.REC/012/001882). The study was registered in the Pan African Clinical Trial Registry database (no. PACTR 201802003232225).
Study population
Women who suffered from pain in areas of lower back and pelvis were initially screened. After the screening process, women were eligible to participate in the study if they had an age ranging from 25–35 years, parity (2–4) times, a body mass index that did not exceed 30 Kg/m
Flow chart of study participants.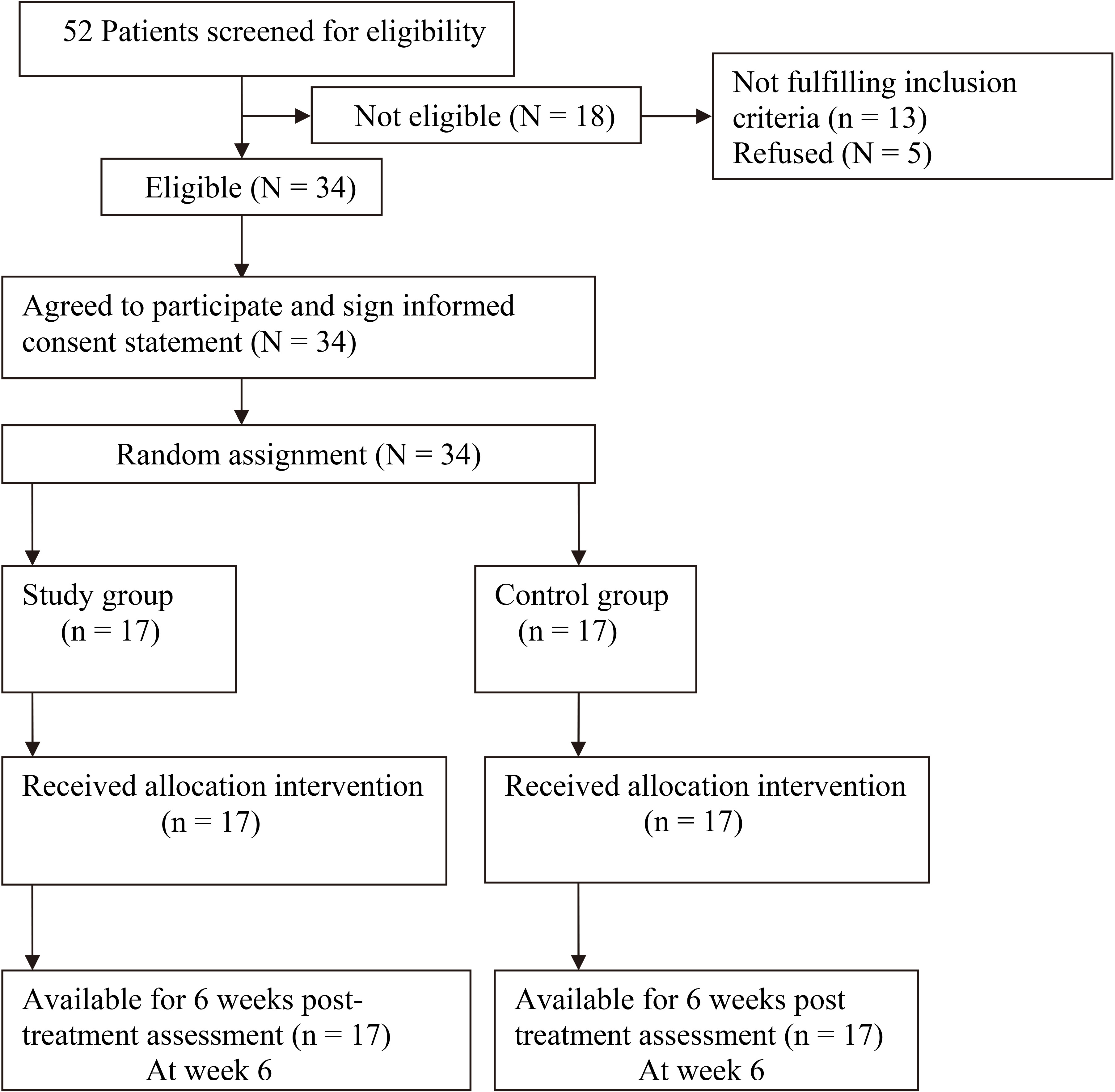
The women were randomly assigned to the study group (
Patients in both the study and the control groups received the same traditional treatment. This includes infrared irradiation followed by continuous ultrasound on the lumbosacral region. The patient was instructed to lie prone and her clothes were removed so that the skin in the lumbosacral region was exposed. Infrared irradiation was applied on the lumbosacral spine for 15 minutes at a 50–75 cm distance (R 125, 250 watt, Philips; 126597: Australia). Then, continuous ultrasound was used with 1.5 W/cm
The study group additionally received core stability exercises 3 times a week for 6 weeks. Before the patient started the main stability exercise, she performed a warm-up exercise which involved a “Cat-Camel” motion of the spine (spine flexion-extension cycles), stretching exercises for calf, hamstring, quadriceps and lower back for about 5 minutes. After that, the participant was asked to perform the core stability exercises. Each exercise was repeated for 10 repetitions with brief rest periods of 3 sec between repetitions and 1 minute rest between each exercise. It is recommended that the isometric contraction in each repetition be held no longer than 7–8 sec [39]. During each repetition for every exercise, the patient was asked to contract her abdominal muscles and maintain this contraction while maintaining her normal breathing pattern.
Abdominal hollowing: The patient assumed the crock lying position and the therapist stride standing at the level of patient’s waist line with both thumbs placed bilaterally anterior and inferior to the anterior superior iliac spine and the fingers of both hands fanned bilaterally lateral to rectus abdominus muscles. Then, the patient was asked to contract her abdominal muscles and press her lumbar region down and hold. Bilateral knee raise: From crock lying position, the patient was asked to slowly raise her right leg toward her chest until it just passes 90 degrees of hip flexion while allowing the knee to flex normally and hold the right leg in this position. Then, she was asked to lift her left leg in the same way so both legs would be elevated. Then, she had to return her right leg to the starting position followed by the left leg. Supine extension bridge: The patient was lying on her back with knees bend and feet flat on the bed. She was asked to slowly raise her pelvis up from the bed until the trunk is in line with the thigh with maintaining her head, upper back, arms and both feet as the point of contact with the plinth and hold. Then, she was asked to lower her hips slowly to the bed. Straight leg rise from prone: From prone lying position, the patient was asked to slowly raise her right lower limb toward the ceiling while maintaining her knee extended and hold. Then, she was asked to return her right leg to the starting position and repeat this exercise alternatively with the left lower limb. After this, the patient was asked to slowly raise both her right and left lower limb toward the ceiling while maintaining her knees extended and hold, then return them slowly to the bed. Alternate arm and leg raise from quadruped position: The patient assumed the prone kneeling position and she was instructed to keep her body movements controlled while performing each step of exercise. The patient was asked to flex her right upper limb and hold, then relax and return to starting position, and repeat this action on the left upper extremity. Then, the patient was asked to raise her right leg backwards off the table no higher than her buttocks and hold, then lower her foot back to the table and relax, and repeat this action to the left leg. After this, the patient was asked to raise the right arm and left leg (opposite upper and lower limbs) and hold then relax, and repeat this action on the opposite arm and leg. Prone abdominal body bridge: From prone lying position, the patient was asked to slowly raise her body up from the treatment table allowing the elbows and feet to be the point of contact with the treatment table, then relax and return to the starting position.
The outcome measures were carried out for each patient individually before and after 6 weeks of treatment by the outcome assessor who was not masked during the study. The main outcome variable was Pain Pressure Thresholds (PPT) using a pressure algometer. The pressure algometer has been found to be non-invasive, efficient and reliable in the exploration of physio-pathological mechanisms involved in muscle pain syndromes [40]. In this study we used a pressure algometer (12-0303 Push-Pull Force Gauge, Fabrication Enterprises, Inc., USA) with a probe size of 1.0 cm
Other outcome measures used to compare the treatment effectiveness between the study and control groups included severity of pain and disability. Severity of pain was evaluated by the Visual Analogue Scale (VAS). Each patient was asked to mark and score on a line at the point that represents her intensity of pain on a 100 millimeter scale, in which 0 represents no pain and 100 represents maximal pain intensity [41].
Baseline participant demographics
Mean and standard deviations of PPT, pain intensity and disability
Disability was measured using the Oswestry Disability Index (ODI). The ODI consists of 10 sections that evaluate pain and domains of daily life that might be disrupted by low back pain, including: personal care, lifting, walking, sitting, standing, sleeping, sexual activity, social activity and traveling. Each section was scored on a 0–5 scale, in which 5 represented the greatest disability. The index was calculated by dividing the summed score by the total possible score, which was then multiplied by 100 and expressed as a percentage. Thus, for every question not answered, the denominator was reduced by 5. If a patient marked more than one statement in a question, the highest scoring statement was recorded as a true indication of disability. Scores are reported on a 0–100% scale with 100% representing severe disability [42].
On the basis of a pilot study, the primary clinical outcome of the current study (PPT) was determined to obtain a power of 0.9 with a significant level of 0.05 and a large effect size of 1.9; total sample size estimation would be 14 participants per group using G*power 3.1 software (Institut für Experimentelle Psychologie: HeinrichHeine-Universität niversitätsstraße, Düsseldorf, Germany). To account for dropout rates, the sample size was increased by 20%, to be 17 per group.
Data analysis
Descriptive analyses, including mean and standard deviation, were performed for all variables. T-test was conducted for comparison of subject characteristics between both groups. Normal distribution of data was checked using the Shapiro-Wilk test for all variables. Levene’s test for homogeneity of variances was conducted to test the homogeneity between groups. Mixed MANOVA was conducted to compare the mean values of PPT, VAS and ODI between the study and control groups, as well as between group comparison and between pre- and post-treatment in each group as within group comparison. Post-hoc tests using the Bonferroni correction were carried out for subsequent multiple comparison. The level of significance for all statistical tests was set at
Results
Base line participant characteristics
The clinical and demographic features of the patients are presented in Table 1.
Between group analysis
Results are summarized and presented as mean (SD) in Table 2. No statistically significant differences were observed between the two groups in any variables at baseline, while after 6 weeks of treatment there was a significant increase in the PPT and significant decrease in VAS and ODI of the study group compared with that of control group (
Discussion
This study demonstrates that the group who received core stability exercises in addition to traditional treatment in form of infrared radiation and continuous ultrasound showed more improvement than the control group in pain and functional disability based on the increase in PPT and decrease in pain intensity and ODI.
The core stability group’s statistically significant increase in the PPT are in accordance with the findings of Cho et al. [43] who conducted a study to evaluate the effects of the core exercise program on pain and active range of motion in patients with chronic LBP, and reported that the core group showed significantly increased PPT in the quadratus lumborum. Furthermore, this result corresponds to the result of a study by Senthil [44], who confirmed a statistically significant increase in PPT after applying segmental stabilization exercise in chronic LBP patients. In the same line, Paungmali et al. [45] reported that the PPT increased by approximately 7.6% after lumbopelvic stabilization training, and they concluded that lumbopelvic stabilization training may be considered as part of the management programs for treatment of chronic LBP.
In the case of chronic pain conditions, such as chronic LPP, the central neuroplastic changes play an important role in the processing of abnormal pain. These changes are caused by continued stimulation rather than by inflammation or damage to peripheral structures. Therefore, patients experience increased sensitivity to pressure and to pain stimuli of a normal degree [46]. According to the biomechanical model theory, weakened muscles cause mechanical irritation in the lumbar spine, thereby causing pain by stimulating pain-sensitive structures [47]. Such continued stimulation serves as an initial cause of central sensitization and chronic pain [48]. It has been reported by Kumar et al. [49] that core stability exercises have the ability to adequately strengthen all trunk muscles responsible for maintaining a strong and stable spine without exceeding cautious injury thresholds for compressive and shear loading. Thus, the effect of core stabilization exercises in activating the deep abdominal muscles, restore the function of weakened muscles and augment the ability to support and control the spine and pelvis, which help to alleviate the mechanical irritation and pain, might explain the significant increase in the pain threshold and reduced pain intensity in the study group in comparison to the control group in the current study.
The reduction of pain intensity in the study group, which received core stability exercise, is in agreement with the findings of Javadian et al. [50] who demonstrated that 8-week stabilization exercise program (involving abdominal bracing and abdominal hollowing exercises) plus routine exercise was more effective than routine exercise alone in reducing pain and disability in a similar subgroup of LBP patients, both post-intervention and at a 3 month follow-up. This is similar to the results by Goldby et al. [51] which showed pain reduction in chronic LBP patients after 10 weeks of specific spinal stabilization, as well as those of Koumantakis et al. [52], which showed the continuation of significant pain reduction in patients with LBP 3 months after application of stabilization enhanced exercise. The result of the current study are also supported by Wang et al. [53], who stated that compared to general exercise, core stability exercise is more effective in decreasing pain and may improve physical function in patients with chronic LBP.
On the contrary, the findings of the current study concerning the reduction of pain intensity in the core stability group are in contrast with those of other studies conducted by Shamsi et al. [54] and Cairns et al. [55]. They concluded that core stability exercise is not more effective than general exercise for reducing pain in chronic non-specific LBP patients, and there was no additional benefit of adding spinal stabilization exercises to a conventional physiotherapy package for patients with recurrent LBP. This contradiction may be attributed to difference in the conventional treatment modalities for the control group between their studies and the current study, as in their studies the control group received a general exercise which may lead to a generalized increased activity rather than the core stability exercise.
The significant reduction in the pain intensity in the core stability group in comparison to the control group, might be explained by the effect of core stability exercise in increasing the tissue blood flow to the affected area which may help to relief the pain by supplying more oxygen and nutrients to the painful area as well as removing waste products and irritant substances from the sensitive tissues. This explanation is in line with the study conducted by Paungmali et al. [56], to investigate the effect of lumbopelvic core stabilization training in improvements of tissue blood flow and lumbopelvic stability in patients with chronic non-specific LBP. They reported that after core stability training there are significant improvements in the tissue blood flow and lumbopelvic stability levels among patients with chronic non-specific LBP.
Increasing the functional performance of patients with LPP is a desirable and tangible outcome to researchers but most importantly to patients. Concerning the significant improvement in LPP intensity and functional disability in the core stability group compared with the control group in the current study is in agreement with the findings of França et al. [57] who reported that segmental stabilization exercises effectively reduce pain and functional disability in individuals with chronic LBP. Furthermore, functional disability improvement was in line with the study of Stuge et al. [30] who found that specific stabilizing exercises were considerably more effective in improving functional status and improving health related quality of life as compared to an intervention without specific stabilization exercises.
The current study has some limitations, however, each of which point toward directions of future study. The primary limitation was the lack of blinding of the physiotherapist who provided interventions, due to the type of intervention which need the direct communication between the physiotherapist and the patients. In addition, the initial selection of the patients was represented as a convenient sample rather than a random sample of the whole population. Furthermore, the study considered only the immediate effects of core stability exercise on pain intensity and functional disabilities among postpartum LPP patients and did not reflect the long term effects. Despite the limitations, the current randomized controlled study indicates that core stability exercises may be appropriate treatment for postpartum LPP by decreasing pain and improving the functional performance.
Conclusion
The results of the present study show that core stability exercises in addition to infrared radiation and continuous ultrasound have positive effects on pain threshold, pain intensity and disability. These observed effects should be of value to clinicians and health professionals involved in the treatment of postpartum LPP.
Footnotes
Acknowledgments
The authors would like to thank all participants for their collaboration in this study.
Conflict of interest
None to report.