
Abstract
BACKGROUND:
Fibromyalgia (FM) is a chronic condition characterized by widespread muscular or musculoskeletal pain of at least 3 months’ duration, occurring above and below the waist, on both sides of the body.
OBJECTIVE:
The aim of this study was to evaluate the effectiveness of a rehabilitation program based on motor imagery versus a conventional exercise program in FM in terms of pain, functional and psychological outcomes.
METHODS:
Twenty-nine female subjects were randomly assigned to a group receiving motor imagery-based rehabilitation (MIG) or to a control group (CG) performing conventional rehabilitation. Outcome assessments were performed before (T0) and after 10 sessions of treatment (T1) and at a 12-week follow-up (T2). Pain, function and psychological measurements were conducted by means of different questionnaires.
RESULTS:
Both treatments improved all outcomes at post-treatment (T1) and follow-up (T2). The MIG showed a significant improvement in anxiety disorder associated with FM with respect to the CG, as well as improvements in coping strategies.
CONCLUSIONS:
Rehabilitation treatment based on motor imagery showed a stronger effect on anxiety and coping behavior than traditional physiotherapy in patients with FM. Integrated psychological support would be desirable in this setting. Further research is needed to explore the aspects investigated in more depth.
Introduction
Fibromyalgia (FM) is a chronic condition characterized by widespread muscular or musculoskeletal pain of at least 3 months’ duration, occurring above and below the waist, on both sides of the body. According to the 1990 American College of Rheumatology criteria [1, 2], it was formerly defined by pain on digital palpation of at least 11 out of 18 predefined tender points. FM is estimated to affect about 5% of the general population, with a prevalence of 3.4% in women and 0.5% in men.
Although the etiology and pathogenesis of FM are still not well defined, some authors suggested that it may be due to peripheral or central “hyperexcitability” of the central nervous system at the level of the spinal cord or brain stem, causing alteration of pain perception. Also, the memory of recent pain and of painful situations, above all contextual with movement of the body, leads FM patients to avoid situations linked to emotional distress and to be afraid of physical activity [3]. In fact, FM can be considered to fall within Craig’s definition of chronic pain which recognizes both a perceptual component and emotional component [4]: “pain occurs in the body but is recognized in the mind”.
With regard to the mechanisms underlying chronic pain, some authors have suggested a balanced relationship between proprioception, tactile acuity and cortical modulation [5, 6, 7, 8]. The persistence of chronic pain can be interpreted as an inability of the body to overcome a perceptual afferent discrepancy, creating a “sensorimotor” conflict [9, 10]. To date, the scientific literature shows no evidence on the application of rehabilitation programs that take into account these elements in FM, whereas in chronic non-specific low back pain, programs based on movement observation and motor imagery have been tested [11, 12, 13, 14]. The aim of this research was to study the possible efficacy of a novel rehabilitation approach involving a motor imagery-based exercise program, versus a conventional rehabilitation approach in FM syndrome. Pain reduction was set as the primary outcome, and patients’ psychological and emotional conditions were also analyzed.
Materials and methods
This was a pilot study designed as a double-blind, randomized, controlled trial, and took place from July 2016 to December 2017 at the rheumatology clinic of the Sant’Andrea University Hospital in Rome. Female patients who had previously been diagnosed with FM using the 1990 American College of Rheumatology criteria were recruited. The 2010 diagnostic criteria [15] could not be considered in the present study as they were published after the diagnosis of most of these patients. The FM syndrome diagnoses were made a rheumatologist on the basis of the aforementioned criteria; accordingly, we included all patients who had experienced widespread pain for more than 3 months, and who experienced pain with 4 kg/cm
Through an oral presentation, patients were informed in detail about the scope and procedures of the study (as per the Declaration of Helsinki). They were then invited to participate in the clinical trial, in which they were randomly allocated to the motor imagery-based rehabilitation group (MIG) or the control group receiving conventional rehabilitation treatment (CG). Patients were allocated according to a computer-generated simple randomization list at a 1:1 ratio (software MATLAB R2007b
With regard to the assignment of the patients to the study groups, a physiatrist assessed the patients sent by the rheumatologist in order to confirm the presence of the inclusion criteria and rule out the presence of any exclusion criteria. A psychologist then provided information to the patients and had them sign an informed consent document. In all cases, the physiatrist, patient and psychologist were unaware of the rehabilitation treatment group (conventional or motor imagery) to which the patients were assigned.
This study protocol was developed in accordance with the Consolidated Standards of Reporting Trials (CONSORT) guidelines [16]. The study protocol was approved by the ethics and experimental research committee of the Department of Psychology of the Sapienza University of Rome. Outcome assessments were performed in each group before treatment (T0), at the end of treatment, i.e. after 10 rehabilitation sessions (T1), and at a 12-week follow-up (T2).
Evaluation of fibromyalgia pain and psychological impact
At each of the three assessment time points, patients were administered the following scales:
The Fibromyalgia Impact Questionnaire (FIQ) [17]. This is a self-administered scale used to assess the present health status of patients with FM. Scores range from 0 to 100, and higher scores indicate a greater impact of FM on functioning (0 to 39 represents a mild effect, 40 to 60 a moderate effect, and 61 to 100 a severe effect). The Health Assessment Questionnaire. Usually self-administered, this is a comprehensive scale used to measure health outcomes in patients with a wide variety of chronic diseases [18]. It contains 20 items distributed across 8 components and the scores for each dimension are transformed to give an overall disability index score of between 0 and 3. The Fibromyalgia Assessment Status (FAS). This is a simple, self-administered index that combines, in a single measure (score range: 0 to 10), a patient’s assessments of fatigue, sleep disturbances and pain evaluated based on a list of 16 non-articular sites [19]. A visual analog scale (VAS), ranging from 0 (no pain) to 10 cm (maximum pain). VAS is a one-dimensional measure widely used to assess pain intensity [20].
In both groups, a psychologist administered the following scales to assess the subjects’ psycho-emotional profile:
The Hamilton Anxiety Rating Scale (HAM-A) [21]. Anxiety severity was assessed using the HAM-A, which includes 14 items that investigate physical and mental indicators. Each item is rated on a five-point Likert-type scale with scores ranging from 0 to 4, where higher scores indicate more severe anxiety: the psychic subscale (items 1–6 and 14) addresses the more subjective cognitive and affective complaints of anxiety (e.g., anxious mood, tension, fears, difficulty concentrating), and is particularly useful in assessing the severity of generalized anxiety disorder. The somatic subscale (items 7–13) focuses on features such as autonomic arousal, respiratory, gastrointestinal and cardiovascular symptoms. The Hamilton Depression Rating Scale (HAM-D). This scale contains 17 items pertaining to symptoms of depression experienced over the last week; eight of these are scored on a 5-point Likert-type scale and nine on a 3-point Likert-type scale. A score of 20 or higher indicates moderate to severe depression. The existence and severity of the measured items were evaluated by the interviewer (psychologist), who was trained in HAM-D evaluation [22]. The Italian version of the 20-item Toronto Alexithymia Scale (TAS-20). Used to assess alexithymia, the TAS-20 is composed of 20 items rated on a five-point Likert scale, from “strongly disagree” to “strongly agree”. In addition to the total score, the TAS-20 provides three subscale scores: difficulty identifying feelings (DIF); difficulty describing feelings (DDF), and externally oriented thinking (EOT). In accordance with the literature, the following cut-off points were used to classify patients as non-alexithymic (total score Finally, COPE-NIV, which is the Italian version of the Coping Orientation to Problems Experienced (COPE) inventory, was used to measure a broad range of coping styles. The COPE inventory is comprised of 15 four-item scales. Using the dispositional response format, participants were asked to indicate how frequently they use each coping strategy on a four-point scale ranging from “usually do not do this at all” to “usually do this a lot” [24]. Five subscales were considered: social support (SS), avoidance strategies (AS), positive attitude (PA), problem solving (PS), and turning to religion (TR).
All patients performed a total of 10 treatment sessions. Sessions lasted 60 to 90 minutes and were performed twice a week in groups of three to four patients. If patients missed a session or sessions due to personal or professional reasons, they were able to recoup the missed session(s) in order to ensure that all of them completed the whole program. To promote patients’ independence in pain management, a physiatrist conducted a brief educational session to enhance the patients’ knowledge of FM and improve their self-care skills.
Sample of exercises performed during a motor imagery (MI) rehabilitation session: supine position. A: alternating knee-to-chest movements; B: head and hip rotation in opposite directions; C: “frog” legs and crawling position. D: leg extension, alternating sides; E: “greeting the sun” exercise; F: “cat” position (back flexion and extension).
The gold standard was to choose simple and safe exercises in order to encourage the patient to repeat the schedule at home. The exercises proposed to the MIG were chosen respecting the following principles: slowness, painlessness, promoting attention, easy to imagine.
Each session was divided into six phases:
The patient relaxed on the ground, in supine position, and began diaphragmatic breathing (10 minutes) while the physiotherapist promoted awareness of the body and its contact with the environment (using phrases such as: relax, feel your breathing, feel the contact between each part of your body and the carpet); The patient watched a video clip showing an exercise that was subsequently to be imagined (motor imagery exercise) (5 min); The patient imagined the exercise seen in the video clip (imagining himself/herself executing the observed movement The patient wrote down, and then shared with the physiotherapist and the group, his/her various impressions and thoughts during step 3 (even negative ones relating to imagined pain) (5 min); The patient performed two or three series of at least 10–15 repetitions of the movement, with 3- to 5-minute pauses between series (10 min); The patient shared his/her impressions with the group (10 min).
At each new session, a new exercise to be imagined was added to the rehabilitation program. The rest of each rehabilitation session was devoted to repetition of the exercises proposed during the imagery phases in dynamic training series, ending with stretching exercises.
The main purpose of performing motor imagery-based exercises was to bring the patient back to a condition of feeling and self-perceiving the execution of the movements. The quality of the movement, free from pain, was considered more important than the quantity of repetitions. For this reason, the sessions lasted from 60 to 90 minutes, because the patients often required more time and were not to be rushed into executing the movements.
Sample of exercises performed during a motor imagery (MI) rehabilitation session: seated/standing position. A: passing from the sitting position to the standing position. B: semi-squat on the lower limbs, resting the back against the wall, alternating with the interposition of a sponge ball; C: flexion and extension of the spine as through “taking water from the sea”.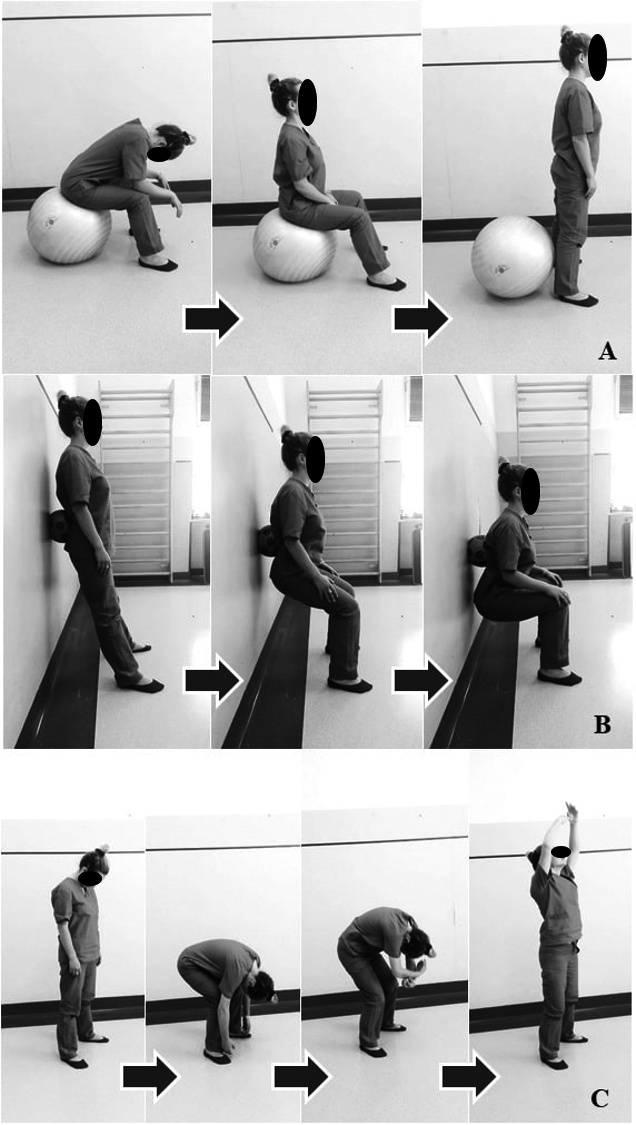
Figures 1 and 2 show the proposed exercises. In supine position, (1A) flexion of the knees to the chest (diaphragmatic breathing, sometimes using soft balls to support and press on the painful points of the back); (1B) rotation of the head and pelvis in opposite directions; (1C) “frog” position, abduction and flexion of the hips at 90
The CG received a conventional rehabilitation protocol, based on ten 1-hour sessions, held twice a week (over a 5-week period), previously found to be effective in FM [25]. The exercises included low- to moderate-impact aerobics training, walking in a circle, alternating with periods of going up and down stairs (3 steps, for 10 minutes), for a total of 20 consecutive minutes; there were also posture exercises for the back and proprioceptive exercises for the trunk, to improve axial stability. Each exercise was repeated 10 times (3 series of 10 repetitions), with a rest of at least 3 minutes between series. All sessions ended with stretching and diaphragmatic breathing exercises.
Statistical analysis
Because the clinical scores are ordinal numbers, the data are expressed as median and quartiles, including inter-quartile range (IQR, the third minus the first quartile). Data were shown using box and whiskers plots for the FIQ and HAM-A scales: the boxes show the first and third quartiles and median (middle bold line in box), whereas the whiskers represent the most extreme values within 1.5 times the inter-quartile range from the ends of the box (Figs 3 and 4). Repeated-samples Friedman’s two-way analysis of variance by rank test was carried out to assess the scale score changes in each group over the three evaluations (T0, T1 and T2). Nonparametric statistics were also used for the between-group analyses; in fact, the two groups were compared using the Mann-Whitney U test, setting the alpha level of significance at 0.05. All data analysis was performed using SPSS for Mac v.21 (SPSS Inc., Chicago, IL, USA).
Box and whiskers plot of The Fibromyalgia Impact Questionnaire (FIQ) at the three assessment timepoints for the two groups.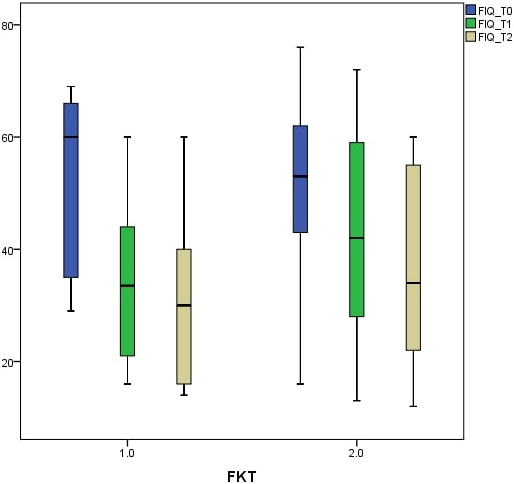
Box and whiskers plot of the Hamilton Anxiety Rating Scale (HAM-A) at the three assessment timepoints for the two groups.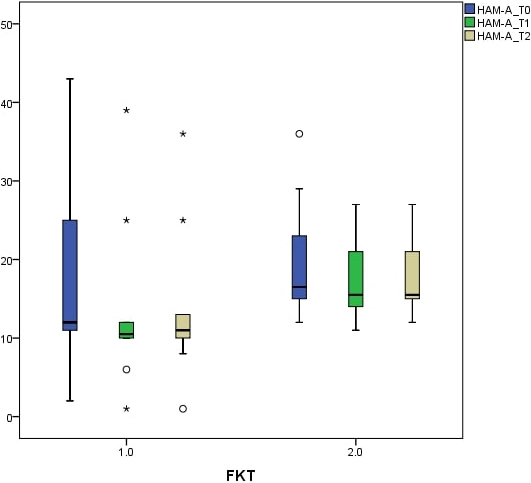
Group comparisons at baseline (T0). Median and interquartile range (IQR) are reported. In comparisons,
VAS: visual analog scale, MIG: motor imagery group, CG: control rehabilitation group.
A total of 44 patients were enrolled, 29 of whom were randomly assigned to the two groups. Over the course of the treatment, three patients dropped out (2 in the MIG and 1 in the CG). No patient discontinued the rehabilitation due to acute exacerbation of pain, and all patients performed ten treatment sessions.
At baseline, the two groups were homogeneous with regard to age, height, weight, body mass index, and VAS score, as shown in Table 1. Also, the median scores for the three clinical scales (FIQ, FAS and HAQ) did not differ significantly at baseline (T0).
Median and interquartile range (IQR) of clinical scores for the two groups at the three assessment times.
-values in the last column for each scale refer to within-group FR analysis, whereas
-values in the bottom row refer to group comparisons at baseline, based on the MW.
-values are reported in bold if statistically significant (
0.05)
Median and interquartile range (IQR) of clinical scores for the two groups at the three assessment times.
MW: Mann-Whitney U test, FR: Friedman analysis, FIQ: Fibromyalgia Impact Questionnaire, FAS: Fibromyalgia Assessment Status, HAQ: Health Assessment Questionnaire, VAS: visual analog scale, MIG: motor imagery group, CG: control group, Time: Time of assessment, T0: baseline, T1: end of the treatment, T2: follow-up.
Median and interquartile range (IQR) of psychological scores for the two groups at the three assessment times.
MW: Mann-Whitney U test, FR: Friedman analysis. HAM-A: Hamilton Anxiety Rating Scale, HAM-D: Hamilton Depression Rating Scale, COPE: Coping Orientation to Problems Experienced, TAS-20: 20-item Toronto Alexithymia scale, MIG: motor imagery group, CG: control group, Time: Time of assessment, T0: baseline, T1: end of treatment, T2: follow-up.
Median and IQR of COPE-NIV scores (cognitive and behavioral strategies to manage stress), in five independent dimensions, for the two groups at the three assessment times.
MW: Mann-Whitney U test, FR: Friedman analysis, COPE-NIV: Coping Orientation to the Problems Experienced (Italian version), SS: Social Support, AS: Avoidance Strategies, PA: Positive Attitude, PS: Problem Solving, TR: Turning to Religion, MIG: motor imagery group, CG: control rehabilitation group, Time: time of assessment, T0: baseline, T1: end of the treatment, T2: follow-up.
Tables 2–4 show the median and IQR values and summarize the results for the outcome measures, which differed significantly between T1 and T2 in both groups. Friedman’s analysis in the MIG revealed statistical significance (
In the between-group analyses, the Mann-Whitney U test revealed, for the HAM-A scale, a statistically significant difference between the two groups in favor of the MIG (T1,
Our results seem to support the use of motor imagery in rehabilitation of FM syndrome: the novel approach consisting of a MI exercise program, when compared with a conventional rehabilitation approach, showed stronger effect on anxiety and coping behavior than traditional physiotherapy.
In terms of VAS, MIG showed better results than no treatment group, but not in comparison to a usual physiotherapy group. The MIG showed an improvement in anxiety disorder associated with FM, and also in coping strategies (COPE-SS and COPE-PA). These results were maintained at follow-up, and with regard to the HAM-A scale, there emerged a statistically significant difference between the two groups in favor of MIG. The majority of patients with chronic fatigue syndrome and FM inappropriately adopt defensive coping strategies, partly because of an altered perception of their disease condition. In addition, patients with FM often show a high level of kinesiophobia and a lot of concern about their illness, tendencies that lead them to develop catastrophic thoughts: in these cases, a rehabilitation approach alone can be insufficient and additional psychological treatment is needed [26, 27]. Our results support this aspect, as both groups (MIG and CG) showed abnormal levels of coping strategies. Although there was no statistically significant difference between the two groups, the response to treatment was better in the MIG with regard to the COPE items SS and PA (Table 4).
The presence and intensity of depressive symptoms and anxiety correlate significantly with the symptoms of FM. Moreover, anxiety is a relatively constant feature of the personality of people with FM, meaning that it is important to involve a psychotherapist in the rehabilitation program of these patients as discussed in the European League Against Rheumatism (EULAR) recommendations [28].
The introduction of motor imagery exercises allows the physiotherapist to use a “narrative” approach during rehabilitation that might result in a shared understanding of the patient’s attitude [29]. The patients were encouraged to talk with the physiotherapist and to share the sensations they had during the imagination phase with the other group members. This step was treated as a proper rehabilitation exercise (phases 4 and 6 of the MIG program). Other authors have suggested the importance of training approaches that may be effective in reducing comorbid anxiety symptoms and physical inactivity: findings show that a fundamental focus is the patient’s adherence to the long-term rehabilitation program, because a longer duration of treatment with good adherence allows better containment and reduction of anxiety [30, 31].
Another important aspect in FM is the qualitative aspect of chronic pain, which is closely linked to the psycho-emotional profile. Cognitive stress may negatively affect central pain modulation in patients with FM leading to higher hippocampal activation: however, even though this topic is very interesting, the scientific evidence is still limited [32]. Motor imagery exercises seem to act positively on the pain experience of the FM patient [33]. Ideomotor cues do not only influence preplanned responses; indeed, they can also effectively insert intentions to act, creating behavior de novo, as predicted from ideomotor patterns of action control [34]. An interesting aspect of our research is the finding that both the rehabilitation treatments (at T0, TAS
Although the enrolled patients were evaluated at a twelve-week follow-up, the absence of a longer-term follow-up may be considered a limitation of our study. In addition, there was no blinding of all subjects, therapists and evaluators, and furthermore quantitative measurements were not used but only ordinal ones, without a unit of measurement. Finally, increasing the number of patients in each group may enhance the generalizability of our findings. On the other hand, our research represents an attempt to investigate the efficacy of an alternative rehabilitation pathway, which also takes into account the subjects’ psychological profile. It is important to consider that FM patients are often reluctant to undergo a psychological consultation or psychotherapy, while they readily accept rehabilitation. A treatment involving motor imagery, having a positive impact on psychological aspects, may play an important role in this regard.
Conclusions
In conclusion, the motor imagery-based rehabilitation treatment seemed to have a positive effect in terms of reducing pain and improving physical function, and it also showed a good impact on anxiety mood in patients with FM syndrome. Given the close interconnection between mind and body in FM syndrome, the integration of psychological support would be desirable in this setting. A personalized motor imagery-based rehabilitation program involving neurocognitive techniques may represent a polyvalent tool for the management of both physical and psychological symptoms in FM. Further research is needed to investigate these aspects.
Availability of data and materials
The datasets supporting the conclusions of this article are included within the article.
Funding
None to report.
Footnotes
Acknowledgments
The authors want to thank Daniela Altavilla from the Department of Dynamic and Clinical Psychology, Sapienza University of Rome, Italy, and Gabriele Fidenzi and Claudia Piscitello from the Department of Anatomical and Histological Sciences, Legal Medicine and Orthopedics, Sapienza University of Rome, Rome, Italy, for their work.
Conflict of interest
None of the authors reported any financial and/or personal relationships with other people, or organisations, that could inappropriately influence (bias) the work.