
Abstract
BACKGROUND:
Myofascial pain is a common, but poorly understood multifactorial condition.
OBJECTIVE:
This study analyzed how the degree of central sensitization (nociplastic pain) can impact the response to physical therapy for patients with myofascial pain.
METHODS:
This prospective, observational cohort study compared pain phenotyping and functional measures in 30 participants with non-acute neck/shoulder girdle primary myofascial pain following 3-months of physical therapy. The Fibromyalgia Survey Questionnaire Score served as a surrogate of central sensitization.
RESULTS:
All participants demonstrated some benefit from physical therapy; however, those with moderate levels of nociplastic pain features were less likely to have clinically significant improvements on the Neck Disability Index, PEG score, or pain catastrophizing measures. Those with higher levels of nociplastic pain had a similar chance of showing improvement as those with lower levels, except regarding catastrophizing. Significant improvements were independent of the type or amount of therapy received.
CONCLUSION:
The degree of nociplastic pain in patients with myofascial pain appears to be inversely related to improvements from a peripherally based treatment. This is not to say that individuals with moderate to higher levels of nociplastic pain do not benefit from physical therapy, but they proportionally benefit less.
Introduction
Myofascial pain is a clinically diagnosed condition in which pressure on tender muscles will illicit pain at a distant location. The prevalence of myofascial pain is unknown, but has been reported from 30% of regional pain complaints in a general medicine clinic up to 85% in a comprehensive pain practice [1, 2]. Myofascial pain appears to disproportionally impact females [3]. Overuse injuries, faulty posture, muscle imbalances, poor body mechanics, connective tissue disorders, and prior soft tissue trauma have all been implicated as peripheral risk factors for developing and sustaining myofascial pain [4, 5]. Central factors including psychological stress, mood disturbances, and poor sleep may also contribute to the confluence of a more broad condition often referred to as myofascial pain syndrome [1, 4, 5]. Numerous studies have indicated that sensitization of the central nervous system can result in multiple pain conditions and hypersensitivities, including muscular pain [3, 4, 5, 6, 7, 8, 9, 10]. Furthermore, there is emerging evidence of hyperinnervation of myofascial trigger points by the sympathetic nervous system [11].
Nociplastic pain is the most recent term used to describe the category of pain that appears to be distinct from nociceptive or neuropathic pain [12]. In addition to the prototypical nociplastic pain condition of fibromyalgia (FM), a number of other conditions such as chronic fatigue, irritable bowel disease, temporomandibular disorder (TMD), chronic back pain, and regional pain conditions (including myofascial pain) have been proposed as having nociplastic pain features [3, 4, 6]. In addition to widespread pain, the core symptoms of a nociplastic pain include fatigue, memory difficulties, mood changes, and sleep disturbances [6, 7]. Previously, the diagnosis of FM was based on widespread pain and the presence of a delineated number of localized tender points, not necessarily including the associated referral patterns seen with myofascial pain trigger points [8]. In 2010, the American College of Rheumatology (ACR) established the Fibromyalgia Survey Questionnaire (FSQ) as a new research criteria for the diagnosis of FM with greater emphasis on the above core symptoms of nociplastic pain, in addition to widespread pain complaints [9, 10]. This was a paradigm shift away from a more peripheral pain generator focus within the muscle towards an emerging appreciation for maladaptive nociplastic changes resulting in central pain sensitization. The FSQ Score has demonstrated good reliability and validity to help guide clinicians and researchers in establishing a diagnosis of FM [13]. The score from the FSQ provides a continuous variable that serves as a potential surrogate to the degree of central sensitization features, often referred to a “fibromyalgia-ness”. This tool predicts both pain and disability levels across a number of painful conditions traditionally considered having a peripheral inflammatory or nociceptive basis, including rheumatoid arthritis, pelvic pain, and osteoarthritis [14, 15, 16]. These nociplastic pain features have been shown with both quantitative sensory testing and functional neuroimaging [15, 17]. This new appreciation has allowed researchers to report that patients with higher levels of nociplastic pain are less likely to improve, or have atypical responses to, interventions targeting peripheral tissue pathology, such as surgery or spinal injections [14, 16, 18].
To progress towards more individualized pain management strategies, this first-ever known prospective study of how the degree of nociplastic pain features can influence the management of myofascial pain. The purpose of this prospective, observational cohort pilot study was to assess the impact of the baseline FSQ Score on pain and functional outcomes for patients referred to physical therapy for subacute or chronic neck and/or shoulder girdle pain consistent with a primary myofascial pain diagnosis. Our hypothesis was that participants that are higher on the continuum of nociplastic pain features would demonstrate fewer symptomatic and functional improvements following a peripherally based treatment of physical therapy. Conversely, participants with lower indices of nociplastic pain would have greater improvements in these areas. The impact of this study furthers the understanding of how nociplastic pain features influence treatment outcomes of various pain conditions previously felt to reside solely in the periphery.
Methods
This study was approved by the University of Michigan Institutional Review Board (HUM00093722) and registered with ClinicalTrials.gov (NCT04929171). A total of 85 participants were recruited and completed the baseline survey with 41 completing the follow-up survey; however, an additional 11 were excluded due to missing data. Thirty compensated participants completed both baseline and approximately three-month follow-up questionnaires after completing a course of physical therapy between May 2, 2016 and November 23, 2019. Participants were drawn from new patients evaluated at a tertiary care spine and musculoskeletal clinic. In addition to recruitment within the clinic, research staff contacted potential participants that were identified through a chart review of the clinic’s medical record. The primary inclusion criteria were for English-speaking participants ages 18 and over who were diagnosed by their physician with non-acute (more than two weeks) neck and/or shoulder girdle primary myofascial pain who were subsequently referred to a physical therapy treatment. Additional criteria included physician documentation of muscle tenderness with a referral zone reported. Participants with a known diagnosis of FM were included as this was a key variable in the study. The goal was to obtain a relatively equal number of males and females; however, it is understood that both myofascial pain and nociplastic pain tend to impact females at a much higher rate [3].
To reduce the potential confounding that another medical condition could lead to a secondary myofascial pain response, extensive comorbid exclusion criterion included: TMD, frozen shoulder, visceral pain, cervical radiculopathy, postlaminectomy syndrome, rheumatoid arthritis, Sjögren’s syndrome, connective tissue disorders, acute soft tissue injury/trauma, myositis, myopathy, or other clear potential secondary causes. Other exclusions included: use of chronic high-dose opioid medication greater than 100 mg oral morphine equivalents per day; individuals receiving or applying for compensation or disability; the inability to provide informed consent; severe physical impairment (e.g., blindness, deafness); comorbid medical condition limiting function (e.g., malignant cancer); reported illicit drug use; a severe psychiatric condition that would limit judgment; lack of internet access.
This study was no more than a minimal risk as the questionnaires used were determined not to impact the patient’s usual and customary physical therapy care. After reviewing and agreeing to the informed consent, qualifying participants received instructions on how to navigate the web-based interface. Baseline questionnaires required about 30 minutes and were completed at the initiation of the physical therapy course using a series of validated self-report questionnaires. Concomitant pain medications usage and other treatments, (e.g., osteopathic/chiropractic manipulations, acupuncture, and injections) were also collected. Similar follow-up measures were recorded at three-months to assess participant response to physical therapy and additional treatments.
Consistent with other foundational nociplastic pain studies, the following measures were used to establish pain phenotyping, as well as baseline and outcome functional measures [14, 16, 18].
Pain phenotyping measures:
The 2010/2011 ACR FSQ criteria for FM is a validated self-report survey that contains measures of both a Widespread Pain Index (WPI) and Symptom Severity Scale (SSS) comorbid symptoms on a 0 to 31 scale. Research criteria for the diagnosis of FM was considered a score of 13 or higher [3, 9, 10, 13]. For this study a median tertile-split analysis categorized nociplastic pain features on the continuum as low (0–6), medium (7–12), or high (13 or higher). The results of this questionnaire will be referred to as the FSQ Score. The PainDETECT is a measure designed to help distinguish between nociceptive and neuropathic pain [19]. Patient Reported Outcomes Measurement Information System (PROMIS) is a series of valid and reliable measures of patient-reported health status for physical, mental, and social well-being. The following PROMIS measures were included: Global Health (10 items); Pain Interference (4 items); Fatigue (7 items); Depression (8 items); Anxiety (8 items); Sleep Disturbance (8 items); Anger (5 items). There was a total of 50 items [20]. The Hospital Anxiety and Depression Scale (HADS) is a valid and reliable instrument for detecting depression and anxiety in medical outpatient clinics [21]. The Pain Catastrophizing Scale (PCS) is a valid and reliable measure of irrational thoughts related to pain with subsections on rumination, magnification, and helplessness [22].
The following functional outcomes were used to determine improvement from a physical therapy referral. Percent change was calculated as [(baseline score
The Neck Disability Index (NDI) is a widely used valid and reliable measure of cervical spine functional limitation [24, 25]. The QuickDASH-9 has been shown to be a valid and reliable measure of upper limb functional limitation [26]. The PEG is a valid and reliable multidimensional measure for initial assessment and follow-up of chronic pain in a primary care setting [27]. A portion of the PEG was used separately to report average pain severity over the previous week on a 0 to 10 scale.
This clinical-based study was focused more so on the response to a referral to physical therapy, and thus, the individual treatment selection was at the discretion of the physical therapist. The referring physicians and physical therapists were blinded to their patient’s participation in the study. The frequency, duration, and discharge from therapy was also left up to the participants and their therapist. Insurance restrictions on physical therapy services were not available to the research team.
The initial intention was to have all participants receive physical therapy within the same health system for improved consistency and data collection. As a tertiary care center, patients come from around the region, and it was determined the expectation for patients to travel great distances to receive regular physical therapy treatments within the health system was not practical. A chart review of all the participants indicated that care was provided by 12 physicians and 24 physical therapists. There did appear to be consistency within individual participants, as the same therapist generally managed them throughout the course of their treatment.
Usual and customary physical therapy treatments for myofascial pain were recorded and categorized as passive, active, or educational interventions. Passive treatments included modalities (ultrasound, hot/ice packs, electrical stimulation, percussion, etc.) or manual therapies (myofascial release, massage, joint mobilization/manipulation, etc.). Active treatments included corrective exercise (stretching, strengthening, etc.) or cardiovascular exercise. Education interventions included postural training, pacing, or ergonomics recommendations. There was no documentation of pain neuroscience education by the physical therapists.
A review of the available post-intervention physical therapy notes indicated that all participants received some combination of therapy interventions including: 100% stretching and/or strengthening, 96.67% manual therapy, 23.33% modalities (heat, e-stim etc.), 76.67% educational (posture, ergonomics, etc.). The mean number of physical therapy visits for all participants was 7.3
Normality of data was assessed using histogram and Q-Q plot assessment. Continuous outcomes (symptom measures, age, number of therapy visits) were assessed with one-way analysis of variance (ANOVA) and repeated measures ANOVA. Pairwise comparisons were completed for significant tests using Bonferroni’s correction for multiple comparisons. Continuous outcome results are presented as mean
Thirty participants were included in the final analysis having completed both the baseline and follow-up surveys after their physical therapy. Table 1 indicates that most of the participants were white (76.9%) women (83.3%) with a mean age of 44.9 years-old
Participant demographics organized by tertile split based on degree of baseline nociplastic pain features
Participant demographics organized by tertile split based on degree of baseline nociplastic pain features
For all 30 participants, the baseline mean (SD) FSQ Score was 10.10 (6.75). Twenty-three percent (
All participants experienced a reduction in their symptoms at (
Percent change in mean outcome measures based on degree of baseline nociplastic pain features
At baseline, Table 2 indicates that nociplastic pain severity levels had a significant effect on all symptom outcomes, except depression. Post hoc testing found that participants with low nociplastic pain severity levels reported significantly lower symptoms in all domains compared to higher level participants following physical therapy. Similarly, low nociplastic pain severity level participants had significantly lower symptoms of anxiety, fatigue, and pain catastrophizing compared to the outcomes from those with a moderate level. Moderate and high nociplastic pain severity levels did not differ significantly in the outcomes for any symptom domain, except pain interference. Similar to baseline measures, nearly all domains were significantly lowered in low nociplastic pain severity level participants compared to high nociplastic pain severity level. When compared to the moderate level, the low nociplastic pain severity level demonstrated significantly lower neck disability, fatigue, sleep, anxiety, and pain catastrophizing following their physical therapy intervention. To demonstrate the functional improvements per nociplastic pain severity level, Fig. 1 shows the change in NDI score that individual participants experienced from baseline to post-therapy.
Individual participants’ change in NDI score from baseline to post-therapy based on degree of baseline nociplastic pain features (Percent Change 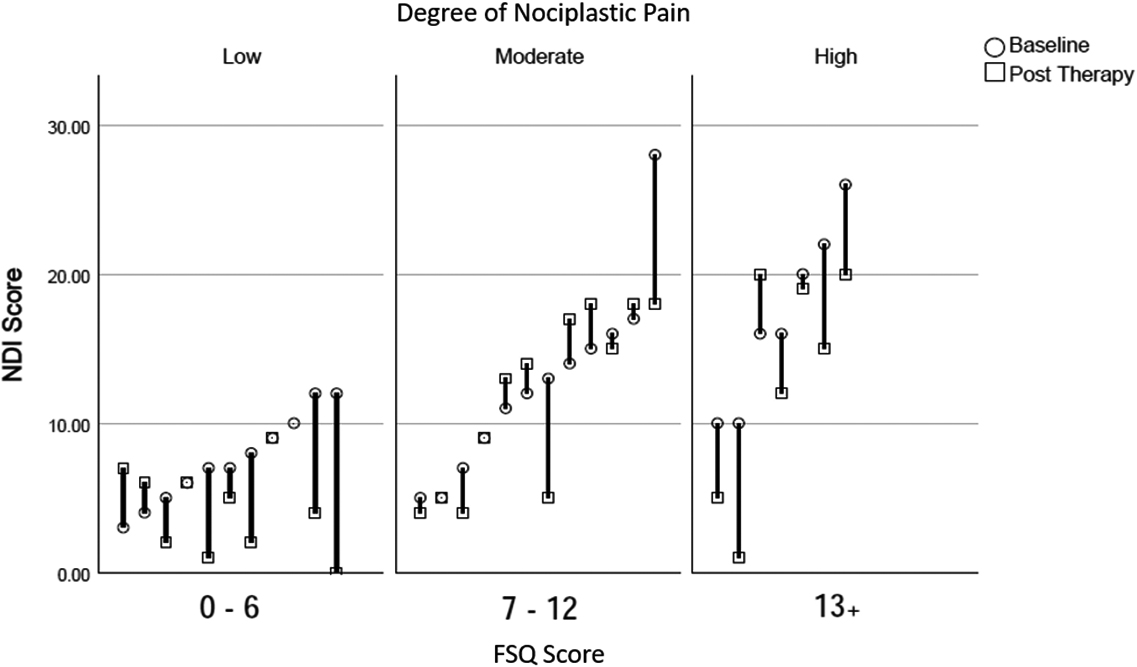
Following a course of physical therapy, 30% of the participants reported more than 50% improvement in their functional outcomes, as measured by the NDI. The nociplastic pain severity level was found to be a significant predictor for achieving a significant improvement in the NDI. Moderate nociplastic pain severity level participants were found to be 92% less likely (B
Regarding PEG score, the moderate nociplastic pain severity level participants were 92% less likely (B
Finally, moderate nociplastic pain severity level participants were 97% less likely (B
While myofascial pain is a rather common condition, secondary myofascial pain appears to be far more common than primary [29]. For example, many individuals experience primary myofascial pain of the upper trapezius with referral to the head or jaw in the absence of any clear identifiable cause. In the setting of shoulder adhesive capsulitis, restricted glenohumeral joint motion can lead to altered scapulohumeral rhythm, which can elicit a secondary myofascial pain response in the very same upper trapezius muscle. This type of interplay can be demonstrated throughout the body. A confounding factor to this is if an underlying primary medical or other musculoskeletal condition (e.g., adhesive capsulitis) was poorly managed, then this could negatively impact the participant’s recovery from their secondary myofascial pain. With such extensive potential for comorbidities, it is nearly impossible to exclude all contributing factors. This study imposed strict criteria to exclude participants with clear peripheral secondary causes for their muscle pain complaint, aside from those with a known diagnosis of FM. While recruitment for this study was challenging under these strict criteria this did provide increased purity in the analysis of participants with primary myofascial pain.
The interplay between central and peripheral factors does not operate in isolation. While widespread pain is the hallmark feature of FM, it can often be misdiagnosed as myofascial pain. Likewise, both patients and clinicians can often misinterpret focal primary myofascial pain as FM [30]. A scoping review by Bourgaize in 2018 reported that there remains no gold standard for the diagnosis of myofascial pain. Thus, not surprisingly there was poor diagnostic sensitivity and specificity for differentiating myofascial pain from FM [31]. It has been postulated that the relentless peripheral stimulation from myofascial pain can contribute to maintaining nociplastic pain in FM [32, 33]. A 2015 meta-analysis concluded that manual therapies, such as myofascial release or connective tissue massage, had moderate-to-large positive effects on pain, anxiety, depression, and function in women with FM [34]. Furthermore, encouraging results from recent dry needling and trigger point injection studies has prompted a 2016 review article by Fernández-de-las-Peñas to advocate for the role of reducing peripheral nociception in the management of patients with FM [35, 36]. As with most myofascial pain studies to date, the impact of central sensitization was not accounted for.
There are currently no widely accepted physical therapy treatment guidelines for myofascial pain [37]. For this observational study, rather than attempting to isolate one specific physical therapy approach (myofascial release, stretching, heat, ultrasound, etc.), the focus was on the overall response to the physical therapy referral. This is a more clinically relevant study as it reflects what actually happens when a physician refers a patient to physical therapy for a muscle pain complaint. While the initial intention was to have participants treated within one health system’s physical therapy clinics (76.67%) to improve consistency, there was a relatively high number of individual physical therapists (25) involved throughout the entire study. This is the reality for most clinicians making a referral to physical therapy, with the exception of smaller communities or confined referral networks. Fortunately, consistency in the study was improved by a relatively high continuity of care for each participant remaining with their own therapist.
Consistent with mounting literature, this study suggests that the degree of nociplastic pain features will impact both symptomatic and functional outcomes from peripherally based physical therapy treatment approaches in the management of myofascial pain. Furthermore, the FSQ Score was inversely correlated with the degree of improvement from physical therapy. Compared to participants with lower nociplastic pain features, those with a moderate severity level were 92% less likely (B
Numerous studies have explored the response of patients with either myofascial pain or FM to various physical therapy interventions [38]. While all participants in this study appeared to benefit from a combination of active, passive, and educational treatments, the types of treatment or number of visits did not appear to impact if the participant had clinically significant pain relief or functional improvements. Further analysis indicated that those participants with moderate degrees of nociplastic pain were less likely to have significant improvements in pain severity, catastrophizing, or function despite receiving similar physical therapy interventions and number of visits. An additional consideration is that a course of physical therapy may impact more than just peripheral pain generators. Pain neuroscience education has been emerging in the field of physical therapy for years and has become integrated in many practices [39, 40]. Even if not documented, elements of reassurance, education, and other psychological strategies are utilized by a physical therapist over the course of their treatment to mitigate the central effects of pain sensitization [41, 42].
This study reviewed participant concomitant use of any of the above medications or interventions started between the baseline and follow-up assessment, but the sample size was too small to clearly identify a confounding impact. A 2021 randomized controlled trial concluded that Pregabalin plus exercise was more effective than exercise alone at improving quality of life in patients with myofascial pain [43]. For patients with higher nociplastic pain features, optimizing pharmacologic and non-pharmacologic management should be considered prior to initiating a referral for more peripherally focused physical therapy treatments.
While this study had a reasonable number of participants enrolled, one of the limitations was a rather large loss to follow-up rate. This is likely multifactorial, but adherence to medical recommendations and exercise has been shown to be rather low in patients with FM. Research teams should be aware of this potential for data loss and plan accordingly to have measures in place to optimize participant adherence to the research protocol. Ultimately, a more robust study may offer insight into factors related to timing, intensity, and frequency of different therapy interventions and specific exercise protocols. While specific neck and upper extremity functional measures were collected, further data on participant’s overall physical activity changes in response to therapy would add value.
This study provides helpful information for clinicians when considering referring a patient to physical therapy for a primary myofascial pain complaint. Physical therapy may offer some but not full relief for patients with moderate or higher degrees of nociplastic pain. Identifying where a patient resides on the continuum of nociplastic pain, using the relatively simple FSQ Score, can help guide clinical decision making and tracking outcomes. It is recommended that once identified, higher levels of nociplastic pain features should be addressed regardless of the underlying etiology [30]. Likewise, as secondary myofascial pain is far more common than primary, clinicians should strive to identify and address underlying factors that may be causing or perpetuating a muscle pain complaint.
Conclusion
This clinically based study offers valuable considerations for the management of patients with muscle pain complaints. All participants with non-acute primary myofascial neck and/shoulder pain demonstrated improved musculoskeletal symptoms (e.g., pain severity, pain interference, neuropathic pain, and pain catastrophizing) following a course of physical therapy, while non-physical symptoms (e.g., sleep, fatigue, anxiety, depression, anger) did not significantly improve. Compared to lower levels of nociplastic pain, participants with moderate levels were less likely to have significant improvements in multiple dimensions of pain, catastrophizing, or function following a physical therapy referral. This study indicates that the baseline degree of nociplastic pain has an impact on both symptomatic and functional outcomes following a referral to physical therapy regardless of the type of treatment or the number of therapy visits. Larger studies of this population are required to compare the effectiveness of individual physical therapy interventions on the full continuum of nociplastic pain features.
Footnotes
Acknowledgments
Grant funding from Michigan Institute for Clinic & Health Research (MICHR).
Conflict of interest
None to report.