
Abstract
BACKGROUND:
Low back pain (LBP) is one of the most common reasons for visiting the doctor. The Mézières method (MM) emphasises body awareness and uses a global postural rehabilitation approach. It is used in the management of LBP, but its effectiveness has received limited formal evaluation.
OBJECTIVE:
To determine the effects of MM on quality of life, pain and functional disability in people with LBP and understand the patient’s bodily experience during the MM intervention.
METHODS:
This protocol study of single-blind randomised controlled trial with a mixed methods design will include 54 people with LBP aged 18 to 65 years. Participants will be randomised into two groups, one will receive MM and the other will receive a control intervention, administered through 10 treatment sessions. Participants will also construct a narrative to provide an understanding of their bodily experience.
RESULTS:
The assessed outcomes will include pain, back pain-related disability assessed using the Roland Morris Questionnaire, and quality of life related to health assessed using the SF12. Outcomes will be assessed at baseline, after the intervention and at a 6 weeks follow-up.
Introduction
Low back pain (LBP) is a major public health problem and is one of the most common reasons for visits to the doctor [1]. It is a multidimensional disorder with interrelated features, including physiological, sensory, affective, sociocultural, behavioural and cognitive aspects [2]. Many different conservative interventions have been reported to benefit individuals with LBP, but the effect sizes are generally small [3, 4]. Furthermore, recurrence rates are high [1], reflecting the complexity of LBP [1]. It is more than just a physical symptom but rather a complex phenomenon that requires a deeper understanding.
Many hypotheses have been proposed for the cause of LBP, the majority of which relate to biological or biomechanical characteristics [5]. Another hypothesis is that the body is conditioned by the sociocultural environment in which it exists [5]. That is, it is not the individual’s conscious decision to use their body as they do; instead the contexts in which they have moved and will move determine this behaviour [5]. To deal with this bodily challenge, the person must understand and use themselves so that they gain a body awareness and associate it with the tasks and environment to which they belong [6]. In this study, this awareness is conceptualised as “self-knowledge” or “self-use” [7, 8].
The Mézières method (MM) is a physiotherapeutic strategy that promotes “self-knowledge”. It was created in France in 1947 by the physiotherapist Françoise Mézières. The approach has provided the foundation for other techniques such as the global (whole body) postural rehabilitation Godelief Denys Struff method, among others [9]. The MM focuses on the interaction between a physiotherapist and patient from a global or holistic perspective. It is based on stretching the myofascial chains of the body, applying manual techniques and performing symmetrical and asymmetrical body exercises with associated sensorimotor work and breathing exercises [10]. Self-knowledge, such as the one presented by the MM, emerges from the use of related forms of movement. The patient’s attention is directed toward their motor behaviour during everyday activities, which translates into the constant quest for quality movements for the body to use to interact with the world. These quality movements may reflect changes in balance, kinetic changes, spinal and cortical excitability and proprioception, among others, which ultimately modify the functioning of the spinal segments affecting the person’s life [10]. In this process, the clinician seeks to identify the causes that may explain the presence of pain, not only to achieve a mechanical objective, but also to help the person explore themselves and understand the factors leading to any imbalance in the musculoskeletal system which may ultimately translate into pain. However there have only been a few studies on the MM approach in people with LBP [11, 12].
The objectives of the study are as follows:
To determine the effects of the MM on quality of life, pain and functional disability, posture and flexibility in persons with LBP compared to a control program of heat, massage and exercises. To understand the meaning of the bodily experience during treatment with the MM from the point of view of patients with LBP.
The following hypotheses will be tested:
The MM is more effective than a program of heat, massage and exercises on improving quality of life, pain and functional disability, posture and flexibility in patients with LBP. The bodily experience of people with LBP who are managed with MM is associated with better bodily awareness and “use of self” than the control program of heat, massage and exercises.
This protocol uses a mixed methods design and will be conducted at the Universidad de La Sabana clinical center, Colombia. The study combines a parallel singleblind randomised clinical trial with a qualitative study using a phenomenological research design
Participants
The participants in the study will be adults with chronic non-specific LBP. Non-specific LBP is classified as the presence of painful symptoms at rest or with movement localised between the lower ribs and the gluteal region, without the presence of other signs that suggest structural damage to the spinal column or adjacent structures. Pain is defined as chronic when it lasts for longer than three months [13]. Participants will be recruited through advertising in the clinic on the university campus and in medical centres near the research centre. Volunteers who are interested in the study will be registered and undergo an initial evaluation, where sociodemographic data will be recorded. In this same evaluation, it will be determined whether volunteers meet the inclusion or exclusion criteria for the study. Participants will attend the clinic at the Universidad de La Sabana.
CONSORT flowchart.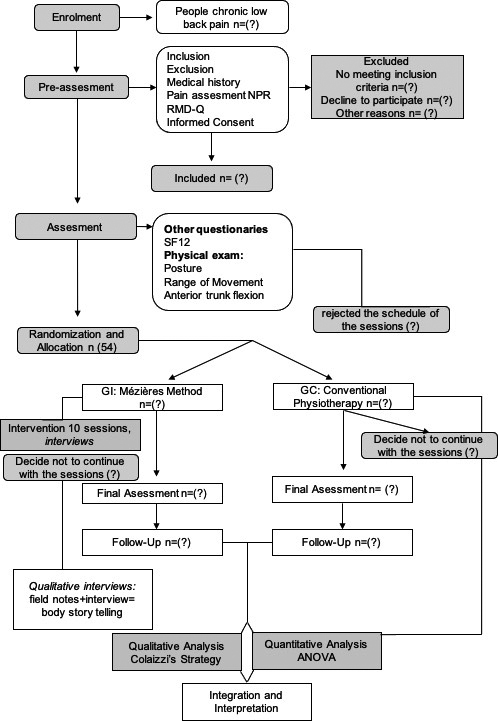
Males or females aged 18 to 65 years with non-specific LBP lasting longer than three months will be included if they have a Roland-Morris questionnaire score higher than 4/24 and an average numerical pain rating (NPR) scale score greater than 2/10 in the past two weeks. Both the Roland-Morris and NPR scores are considered to have clinical relevance in LBP [14, 15].
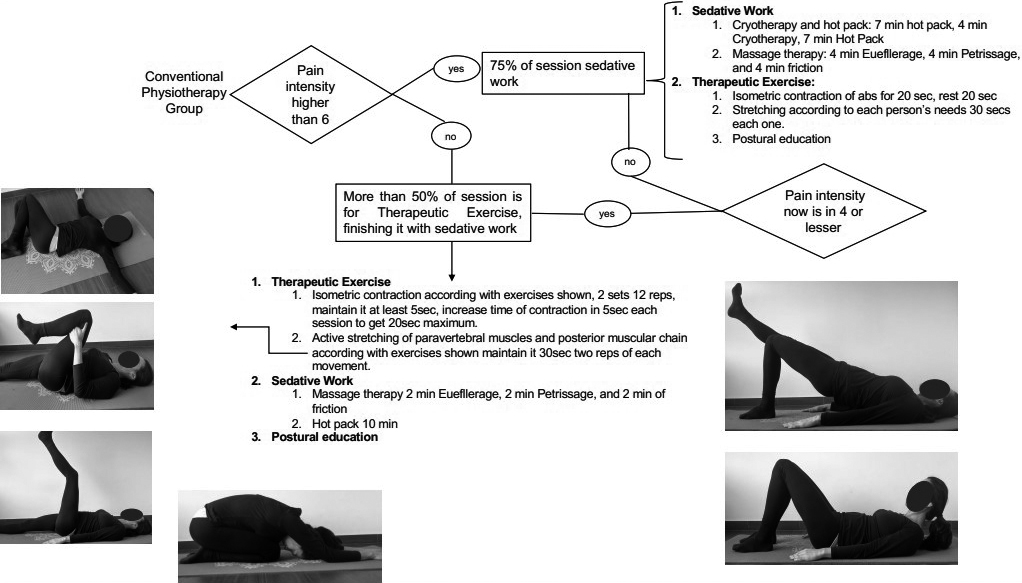
Mézières method intervention. Source: authors.
Individuals will be excluded from the study if their medical history or a review of their clinical records identifies red flags (e.g., tumours), signs of a serious illness associated with LBP, history of vertebral fracture, any physical modification that could impair movement of the lower back and pelvic area (e.g., spinal fusion, post-lumbar surgery, congenital anomalies), LBP associated with lumbar radiculopathy, pregnancy, body mass index higher than 35, and participants with a high risk of persistent disabling LBP identified by the STarT Back Screening Tool [16], evidenced by scores higher than 4 in subscores Q5 to Q9, indicating the need for an interdisciplinary approach to LBP.
Participation in this study will be voluntary. Participants will receive information about the study and will be asked to sign an informed consent form. The study has received ethical approval from the research ethics committee of Universidad de La Sabana Clinic (Oct-9/2018) and the academic research ethics committee of Ramón Llull University (Jun-2/2018). The protocol has been registered under trial registration number NCT03738306 on ClinicalTrials.gov.
All participants will undergo two treatment sessions per week for 5 weeks (10 sessions in total), whether randomly allocated to the intervention group (MM) or the control group (heat, massage and exercises).
MM intervention
The MM intervention will be performed by a physiotherapist certified in MM with 10 years of professional experience who is blinded to both the randomisation and evaluation processes. The sessions will be individual, lasting 45 to 60 minutes. The treatment will begin with a body awareness phase, with the goal of supressing bodily imbalances and myofascial tensions that may be associated with the pain (Fig. 1). The participant will be encouraged to avoid holding their breath and instead try to breathe freely and rhythmically with the breathing pattern that works the best for them. Exercises to improve the extensibility of the myofascial chains will be conducted, while simultaneously avoiding any local or distant compensations that may arise while executing them. The notion of postural alignment and proprioceptive awareness will be encouraged for better sensorimotor integration during each phase of the session [17].
The MM allows the physiotherapist to use different verbal and manual techniques during the movements to assist with the relief of any tension in the myofascial system. Neuromuscular techniques (contraction-relaxation, reciprocal inhibition, myofascial release techniques and deep massage of the muscular system) will be used with the goal of improving the balance of the myofascial chains and thus releasing tensions affecting the lumbar-pelvic complex. This group will not undergo a self-management protocol because the principles of the method so described it.
Control intervention group
The control intervention protocol will include the application of heat, therapeutic massage and muscle stretching and strengthening exercises [18, 19]. The session will be organised according to the intensity of the person’s pain. If the intensity of pain exceeds a score of 6/10, contrasting temperatures (alternating cold and heat) will be applied followed by therapeutic massage. After the sedative therapy, a muscle strengthening and stretching protocol will be commenced (Fig. 2). If the participant’s pain does not exceed an intensity of 6/10, the intervention will commence with trunk muscle strengthening exercises, followed by stretches for the paravertebral and lower lumbar muscles, and finish with heat and massage therapy.
Patient demographics and medical history will be collected. For both baseline and follow-up outcome data, participants will complete questionnaires and undergo a physical examination which will be undertaken by trained physiotherapists who are blinded to the randomisation process and group allocation.
Sample size: The total size of the sample was calculated to be 54 persons (27 participants per group). The following estimated values were used for this calculation: likelihood of type one error of 0.05, likelihood of type two error of 0.2, power of 80%, and effect size of 078 [20] for the primary outcome. The sample size was calculated according to the formula
Randomisation and allocation concealment: A simple computer-generated random number method will be used for the randomisation process. Randomisation will be conducted by an independent researcher who is not involved in the other phases of the research. Once a participant has undergone the baseline evaluation and been included in the study, the independent researcher will be notified and they will assign the participant to the next generated group. The researcher then sends the contact data of the person in a sealed envelope to the relevant treating physiotherapist (intervention or control group). The treating physiotherapist will get in touch with the person to make an appointment and start the assigned intervention.
Qualitative sampling: A sample of the cases will be extracted from participants in the intervention and control groups. Narrative information will be collected in interviews of each participant regarding their bodily experience during the physiotherapy sessions.
Primary outcomes
Pain
The numeric pain rating scale (NPR) [14] is a one-dimensional measure to evaluate the intensity of pain in adults on a numerical scale from 0 to 10, with 0 meaning no pain and 10 meaning the worst pain imaginable.
Measurements of posture and flexibility
Measurements of posture and flexibility
ASIS, anterior superior iliac spine; PSIS, posterior superior iliac spine.
Questions asked in the semi-structured interviews
Roland-Morris disability (RMD) questionnaire
The RMD questionnaire is a simple and easy-to-use instrument that can be self-administered. It consists of 24 items which reflect limitations in different daily activities that can be attributed to LBP. Each item marked by the person receives a score of 1. The total score ranges between 0 and 24, with 24 being the maximum disability that can be attributed to LBP [15], the minimal clinically important difference for RMD will be at least of five points [21].
SF-12
The SF-12 questionnaire evaluates the participant’s quality of life related to health. It seeks to determine how the physical and mental dimensions of health affect a person’s quality of life. This test consists of 12 questions and the total score ranges from 0 to 100, where indicates the lowest level of health and 100 indicates the highest level of health [22].
Posture and flexibility
The postural and flexibility evaluation will be conducted using the ADIBAS
The tests will be conducted under the same environmental conditions in terms of physical space, temperature and time. The Kinect sensor will be secured to a tripod and located around 180 to 90 cm above the person for image capture of the entire body, and from 80 to 120 cm above the person for image capture of the spinal column. The camera will be placed at a height of 90 cm. Participants will perform the tests barefoot and wear appropriate clothing (women in a two-piece swimsuit and men in a one-piece swimsuit) for exposure of the anatomical points of interest: acromion, anterior superior and posterior iliac crests, centre of the kneecap, sacroiliac joint, C7, T1, T7, T12, L3, and S2. Hypoallergenic markers 1 cm in diameter will be attached to the skin in the established anatomical zones to analyse the angles of the variables studied. The participants will stand on a platform marked with footprints so that they place their feet in a parallel position. Measurements of standing posture will be performed and the participant’s flexibility will be assessed in trunk flexion using a modified version of the Thomas test (Table 1).
Qualitative data collection
In this study, semi-structured interviews of participants in both the MM and control groups will be undertaken following sessions 4 and 8. The purpose of this interview is to inquire into the body sensations felt during and after the physiotherapy sessions, the participant’s perception of the physiotherapy sessions and any changes in LBP (Table 2). Qualitative data collection will close when data saturation is reached using a constant comparative method in open coding process with each interview in session 4 and 8.
Follow-up assessment: Re-evaluation will be conducted post-intervention and at 6 weeks following the completion of treatment. Longterm follow-up data will not be collected due to a lack of available resources for the study. The questionnaires and physical tests will be repeated by the blinded physiotherapy assessors.
Statistical analysis (randomised controlled trial)
The statistician conducting all analyses will be blinded to group allocation. Demographic and baseline characteristics of the participants will be analysed to assess the baseline comparability between the groups. Data will be analysed based on the intention-to-treat principle to avoid the effects of possible dropouts. To prevent dropouts researcher team will be in contact with the participants during treatment and assessment periods. All data will be checked for a normal distribution using the Kolmogorov-Smirnov test. Differences in the changes in scores for all outcome measures will be compared between groups using repeated-measures ANOVA. If the data do not have a normal distribution, the Friedman (non-parametric) test will be used. Effect sizes will be calculated for primary outcomes by Cohen’s standardised difference between two means, calculated as follows: [mean [group 1] – mean [group 2]/standard deviation] [24].
Qualitative analysis
The participant interviews will be transcribed for analysis so that their perceptions during the intervention can be extracted. Analysis of data will follow the process proposed by Colaizzi [25]:
transcriptions. formulated meanings. categorisation and clustering of themes. exhaustive description of the phenomenon. fundamental structures. validation of exhaustive description and its fundamental structure: return to the participants.
The formulated meanings phase will be mixed and framed within a deductive-inductive process. To finalise the results and conclusions, the quality criteria for qualitative research will be followed [26]. Formulated meanings will be included following the recommendations by Corbin and Straus [27] starting with open coding and continuing with axial coding to obtain categories and clusters of themes. The generation of categories and themes will be developed by at least two investigators, who will agree on the meanings and relations to categories and themes. This process will be developed using ATLAS.ti software. After determining categories and themes, exhaustive description of the phenomenon will be undertaken, which will take into account the bodily experiences of patients in both groups during physiotherapy sessions.
The qualitative analysis will be conducted with the narrative information collected from participants with LBP. The qualitative and quantitative data will be triangulated to seek complementary or convergent results related to the best effects on the outcomes studied [28]
LBP is a prevalent problem in society and remains the leading cause of chronic disease burden in terms of years lived with disability [29]. Many conservative management approaches are available; however, as might be expected with the varied nature and presentation of LBP, no singular approach has provided the answer to the management of LBP. This study assessed the MM, which was first described some 70 years ago. It has been used clinically and has informed other approaches, but its efficacy for the treatment of chronic LBP has not been rigorously tested in an RCT. It is being trialled at this time because it brings together and implements concepts that have shown value in recent research such as mindfulness [30].
The proposed RCT uses a mixed methods design. The qualitative aspect of the research will add a rich dimension of patient experience with the two treatment protocols. Interactions occur between patients and physiotherapists during a treatment session. This study will seek qualitative information from the patients to build a narrative of their bodily experience while participating in interventions for chronic LBP. The qualitative description will provide an understanding of the patient’s experience and if and how MM facilitates better bodily awareness. There have been no qualitative studies on MM to date, and this study stands to provide a novel insight into patient experience.
We will triangulate the outcome data from the quantitative (RCT) and qualitative assessments for the purpose of obtaining a more complete understanding of LBP [31]. This study considers the personal nature of physiotherapy practice, which requires that clinicians attend not only to quantitatively derived information, but also to the qualitative impact of the lived experience of patients with LBP during physiotherapy sessions [32].
Ethics approval and consent to participate
This protocol study was approved by the ethical committee of the Blanquerna Faculty of Psychology and Education and Sports Sciences on 4 June 2018 and by the ethical committee of the clinical centre of Universidad de La Sabana on 9 October 2018.
Funding
This study was founded by the Universidad de La Sabana under study registration number ENF2019 and was developed at the clinical centre of Universidad de La Sabana with an advisor from the Blanquerna Faculty of Psychology and Education and Sports Sciences.
Footnotes
Acknowledgments
Clinical centre of Universidad de la Sabana. Emeritus Professor Gwendolen Jull, School of Health and Rehabilitation Sciences, The University of Queensland.
Conflict of interest
The authors declare they have no conflicts of interest.