
Abstract
BACKGROUND:
The cranio-cervical flexion exercise and sub-occipital muscle inhibition technique have been used to improve a forward head posture among neck pain patients with straight leg raise (SLR) limitation. However, little is known about the cranio-vertebral angle (CVA) and cervical spine range of motion (CROM) after applying stretching methods to the hamstring muscle.
OBJECTIVE:
To compare the immediate effects of static stretching and proprioceptive neuromuscular facilitation stretching on SLR, CVA, and CROM in neck pain patients with hamstring tightness.
METHODS:
64 subjects were randomly allocated to the static stretching (
RESULTS:
There were no between-group effects for any outcome variables (
CONCLUSIONS:
There were no between-group effects for any outcome variable; however, SLR, CVA, and CROM significantly improved within-group after the one-session intervention in neck pain patients with hamstring tightness.
Keywords
Background
Neck pain is a predominant problem in the general population and carries a high hazard of ongoing relapses or complaints. The primary peculiarity of neck pain represents a pain in the cervical region, often accompanied by range of motion (ROM) limitations and dysfunction [1]. Forward head posture (FHP) is a common symptom of neck pain with an immoderate anterior head position concerning a perpendicular reference line. A previous study has reported that cervicothoracic junction manual therapy significantly affects the cranio-vertebral angle (CVA) and cervical mobility [2]. Similarly, the cranio-cervical flexion exercise (CCFE) activates deep neck flexor muscles and improves the cervical and thoracic spine’s upright posture when one assumes a prolonged sitting position [3]. It happens because the superficial back line of the myofascial chain connects the neck to the lower limbs, and the soft tissue in the cervical area connects the dura matter and sub-occipital muscle fascia [3].
A limited straight leg raise (SLR) can be a predisposing factor for non-specific lower back pain and alterations in the lumbo-pelvic rhythm [4]. Reduced SLR, as evidenced by the limited ROM in the passive SLR test, could be due to changed neuro-dynamics affecting the sciatic, tibial, and common fibular nerves [5]. A previous study reported that stretching methods had been used to improve the SLR test results used in clinical practice, including static, neuro-dynamic stretching, and proprioceptive neuromuscular facilitation (PNF) stretching [6]. Among the stretching methods, static stretching (SS) and PNF stretching have demonstrated efficacy for increasing SLR [7]. The theoretical basis for these longitudinal neuro-dynamic methods includes mobilizing adhesive tissues around the nerve, which may have resulted from some sort of traumatic incident and may directly influence the nerve [8] and decrease the forces linking structures may have on sensitive neural tissues [9]. Interestingly, the SLR improvement can help recover a normal posture because shortened hamstring muscles influence pelvic and spinal postures [10].
To date, several studies have reported the effects of the sub-occipital muscle inhibition (SMI) technique and CCFE in patients with neck pain or SLR limitation [11, 12] and have found improvements of the SLR and CVA [3]. This study aimed to compare the short-term effects of SS and PNF stretching of hamstring muscles on SLR, CVA, and cervical spine range of motion (CROM) among neck pain patients with SLR limitation.
Materials and methods
Study design
This prospective randomized study was conducted according to the principles of the Declaration of Helsinki. The ethics committee and institutional review board at Korea University Medical Center approved the study (2019AN0109). All study patients provided written informed consent, and their privacy would be protected. Based on previous research for hamstring flexibility in patients with a short hamstring [13], an SLR difference
(A) Static hamstring stretching, (B) Proprioceptive neuromuscular facilitation hamstring stretching.
This study was conducted from March to August 2019, and participants were recruited from among hospital patients and visitors. Before the data collection, all patients received an explanation of the experimental protocol, provided by the investigator, and signed an informed consent form before being included. All patients and two outcome assessors were allocated (through a randomized and concealed allocation procedure) to one of the two groups. Only patients with short hamstring who had
Evaluation
Two assessors participated in the study. The intervention and allocation were conducted by a physical therapist (more than 12 years’ experience) who had blinded data analyses and assessments’ features. Analysis and evaluation were performed by an independent physical therapist (more than 15 years’ experience) who was blinded to the intervention protocol.
The SLR test accurately measured the flexibility and tightness of the hamstring muscle. The patient was placed in the supine position on the table with the lower limbs in an extended and relaxed position to measure SLR. The first evaluator held the talus without rotating the hip joint. The subject’s dominant leg was lifted gradually with hip flexion keeping the knee extended until the patient noted discomfort. The opposite limb or pelvis was observed to begin rotating or moving. The second evaluator measured SLR using an AcuAngle
The CVA was measured from a picture of the patient’s lateral view taken by a digital camera (Sony a55; Sony, Tokyo, Japan), using ImageJ image analysis software (ImageJ 1.8.0, National Institutes of Health, USA). Researchers measured the CVA of each patient in both sitting and standing positions and used a previously described method that reported high reliability of this procedure (intraclass correlation coefficient ICC, 0.88) [18]. The CVA has been projected to lie between a horizontal line running through the spinous process of the seventh cervical vertebra (C7) and a line connecting the ear’s tragus with the spinous process of the seventh cervical vertebra (C7). A smaller CVA is associated with a greater FHP [18].
The CROM was measured by a previously described method using a universal goniometer for which the author found extensive intra- and inter-reliability (ICC
Flowchart of the participants throughout the study.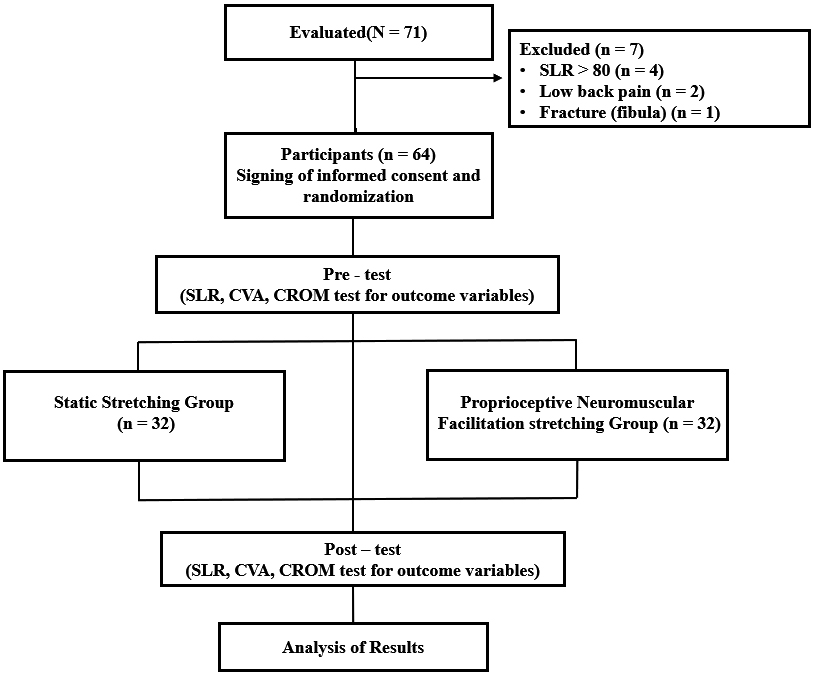
Each subject is placed in a supine position to apply the SS technique on the table with all limbs relaxed. Patients in the SS group received hamstrings stretching in the SLR position until resistance from the hamstring muscle was felt by the first evaluator. Each patient’s dominant leg was lifted gradually to 90
Baseline characteristics of the participants (
64)
Baseline characteristics of the participants (
The PNF stretching used hold-relax (HR) and HR with antagonist contraction (HR-AC) methods to reduce the disturbance of myotatic reflexes, autogenic inhibition, and neural activity in the related muscles [22]. The patient was able to apply PNF stretching in a supine position on the table with all extremities relaxed. The first evaluator lifted the patient’s dominant leg to 90
Statistical analysis
The statistical analysis was performed using SPSS 22.0 (SPSS Inc., Chicago, IL, USA) at a confidence level of
Results
Participants’ general demographics for each group
Excluded patients are shown in Fig. 2. In total, 64 patients were recruited to participate; each was allocated using a random-number table to either the SS or PNF stretching group. This study excluded 7 patients with SLR
Comparison of the SLR test between the 2 groups
The values of the SLR test in each group are summarized in Table 2. For the intra-subject measurements, significant differences were found between pre-intervention and post-intervention values of the SLR test in the SS and PNF stretching group (
Comparison of the SLR test, CROM and CVA measurements for the two intervention groups (
64)
Comparison of the SLR test, CROM and CVA measurements for the two intervention groups (
Note. Values are expressed as mean
The values of the CROM measurements in each group are summarized in Table 2. For the intra-subject measures, significant differences were found between pre-intervention and post-intervention values of the CROM measurements for all cervical spine movements in the SS and PNF stretching group (
Comparison of the CVA measurements between the 2 groups
The CVA measurements on sitting and standing positions in each group are summarized in Table 2. For the intra-subject measures, significant differences were found between pre-intervention and post-intervention values of the CVA on sitting position in the SS and PNF stretching group (
Discussion
The purpose of the present study was to compare the immediate effects of two different types of hamstring stretching methods on SLR, CVA, and CROM in neck pain patients with hamstring tightness. The most important aspect of the present study was that it compared the SS and PNF stretching groups. There were no between-group effects for any outcome variable, however, SLR, CVA, and CROM significantly improved within-group after the intervention.
There were no between-group effects for SLR (
The present study found no significant difference in CVA (
The present study found no between-group effects for CROM (
Therefore, the present study’s results indicated that there were no between-group effects for any outcome variable regarding the SS and PNF stretching groups, but SLR, CVA, and CROM significantly improved within-group after the one-session intervention in neck pain patient with hamstring tightness.
Limitations
Although the between and within-group comparisons demonstrated favorable SS and PNF stretching results, our study’s restrictions can be further addressed in future studies. Researchers did not assess biomechanical or kinematic parameters, such as muscle activation and joint moments. Therefore, future studies that provide direct qualitative parameters evaluating the biomechanical parameters and electromyography recordings from the neck and hamstring muscles are also necessary. Further, the present study focused on patients with SLR
Conclusions
The SS and PNF stretching groups had no between-group effects for any outcome variable, but SLR, CVA, CROM significantly improved within-group after the one-session intervention in neck pain patients with hamstring tightness.
Footnotes
Acknowledgments
The authors are grateful to all subjects involved in this study, as well as authors/publishers/editors of all articles, journals, and books reviewed and discussed for this study. This study was supported by a Korea University Grant (K1605431).
Conflict of interest
All authors were fully committed to absolute integrity and remained unbiased throughout the study. None of the authors had any conflicts of interest or carried any commitments that would influence their duties. The roles of the authors in this study are as follows: Eun-Dong Jeong and Chang-Yong Kim are the primary authors and wrote the manuscript, performed the experimental procedures, interpreted the results, managed the study, and provided critical discussion. Nack-Hwan Kim performed the experimental procedures and critical discussion. Hyeong-Dong Kim performed the experimental procedures and critical discussion.