
Abstract
BACKGROUND:
Low back pain (LBP) causes disability in daily life, and presents not only a health but also a socio-economic problem. New treatment options need to be tested and confirmed.
OBJECTIVE:
Compare the effect of the McKenzie method and spiral stabilization in patients with LBP.
METHODS:
Sixty patients with an average age of 47 years, which were included in our prospective, comparative study were randomly divided into two 30-member groups. One group exercised according to the McKenzie method (MDT), the other one according to the Spiral Stabilization Method (SPS). During the initial examination the Aberdeen Back Pain Scale was used to determine the degree of managing with daily activities and functionality, and the Roland-Morris Disability Questionnaire was used to determine the degree of disability. Check- up was performed after 2 and 6 weeks of treatment.
RESULTS:
In both groups, there was a significant improvement in results after 2 and 6 weeks of treatment (
CONCLUSIONS:
None of these two treatment methods achieved better results, as they both have a comparable effect on reducing disability and improving the management of daily activities and physical functions. Therefore, both are equally effective in patients with LBP.
Background
Musculoskeletal disorders affect millions of European workers in all types of employment each year, and are the most common occupational disease at a European level [1]. One of these disorders are vertebrogenic diseases, which has a significant negative impact on the social and economic side of the human and society. They represent a large group of not only functional but also degenerative diseases, of which common sign is a pain. Regarding low back pain (LBP) itself, the global prevalence among the general population is estimated at 12% [2], to 80% [3, 4]. The causes of mechanical LBP are most often cited by repeated microtraumas and overload [5]. Likewise, the lack of active rest leads to a reduction of the strength and endurance of the postural muscles [6], which results in the development of functional disorders of the musculoskeletal system and pain. One thing to keep in mind is that muscle and the capsule-ligament apparatus begin to weaken with involution processes starting after the age of 45 and related degenerative changes occurring in the joints. Therefore, people need to particularly care for the somatic condition in order to maintain morpho-functional fitness and related body posture at an optimal level in relation to age. Improper body work can cause various failures, including postural disorders and spinal deseases [7].
Treatment of non-specific LBP is currently mainly focused on non-pharmacological treatment. Guidelines encourage active treatments that address psychosocial factors and improvement in function [8].
Physiotherapy, as an irreplaceable part of the treatment of LBP uses various treatment methods nowadays, including commonly used McKenzie Method [9, 10] and Spiral Stabilization methods.
McKenzie Method
The McKenzie Method – Mechanical Diagnostics and Therapy
Spiral stabilization method
Spiral stabilization is an original physiotherapeutic method invented by the Czech doctor Richard Smíšek. It is a set of active exercises with the use of an elastic rope. The goal of the exercise is the stabilization of the spine through the activation of muscle groups, anatomically connected into muscle chains. A muscle chain is a group of muscles whose interplay during movement ensures the stability of the body and by that allowings movement to be performed correctly. The activation of these muscle chains - spirals, produces traction forces affecting the spine, which reduces the pressure generated on the intervertebral discs [14]. According to the current state of the disease, patients practicing this method are divided into 4 groups:
Acute, painful phase – it consists of traction and stabilization of the spine, traction manual techniques, which are part of the concept of SPS, are suitable. These techniques focus on muscle relaxation such as musculus iliocostalis, musculus quadratus lumborum and musculus multifidus. Subacute, less painful phase - focused on relaxing and stretching the shortened muscles that compress the intervertebral discs. At this stage the main techniques are traction, stabilization and relaxation. Healing phase – there should be no pain or loss of function. Beside stabilization and traction, this group also includes exercises for spine rotation and gait coordination. Stabilization phase – formed mainly by stretching the basic muscle groups with a tendency to shortening [14].
Participants
The research group consisted of 60 patients, 19 men and 41 women with an average age of 46.85 years (20–60 years). 60 patients were randomly divided into two equal groups. They all underwent orthopedic examination with the result: vertebrogenic pain syndrome in the lumbar region of functional etiology. Everyone was familiar with the General Data Protection Regulation (GDPR) and agreed to participate in our research.
The set of respondents was deliberately selected according to predetermined criteria. The inclusion criteria were: vertebrogenic pain syndrome in the lumbar region of functional etiology, age 18–60 years. Exclusion criteria: patients, who were taking various types of medication that could affect the results of the research, were not included in the study, discogenic disease with neurological symptoms, pregnancy, age less than 18 years. After meeting the criteria, 74 respondents were contacted, but 60 respondents agreed to be included in the study. The selection of patients for the study took a predetermined time of 6 months. This study group is representative of the population of people aged 18–60 with vertebrogenic pain syndrome in the lumbar region of functional etiology.
Study design
Patients were included in our comparative study in a consecutive manner. Assignment to the appropriate groups was performed in a randomized manner, with patients born in an even month assigned to the MDT group and patients born in an odd month assigned to the SPS group.
Intervention
All patients were treated at the private medical facility Osteocentrum, s.r.o. Presov, Slovakia. The first group was treated only with the McKenzie method. Based on the initial examination, 29 probands were classified with derangement syndrome and 1 with dysfunctional syndrome. No other patient fell into the category of postural syndrome or other group. Of the 29 patients who belonged to the derangement category, 27 used the extension type of exercise as part of their treatment strategy and 2 others used the flexion type of exercise. The mentioned one patient with dysfunctional syndrome used the flexion type of exercise in therapy. After that, they were instructed on exercising at home and postural correction. The frequency of exercise for patients was chosen according to the recommendations of this method. Basically, it was either one type of exercise (number of repetitions 10x) or a static position (with a duration of 2–3 min.). Patients were exercising every 2–3 hours, a total of 6–7 times a day. Often it was only one exercise or position, that did not take too much time, and in similar cases it was necessary to adapt the exercise so that the patient could perform it away from home, e.g. at work. At each visit to the physiotherapist the correctness of the exercise(s) practiced at home was checked first and then additional exercises based on the patient’s current health condition were individually added, following the concept concerning the progression of forces and pressures.
Input and output results after 2 and 6 weeks of treatment in group of patients who were treated with the McKenzie method (MDT)
Input and output results after 2 and 6 weeks of treatment in group of patients who were treated with the McKenzie method (MDT)
Input and output results after 2 and 6 weeks of treatment in a group of patients who were treated with the Spiral Stabilization Method (SPS)
The average values of input and output outcomes of the Aberdeen Back Pain Scale. MDT: group of patients with McKenzie therapy, SPS: group of patients with Spiral Stabilization therapy, input: input outcome, 2 weeks: output outcome after 2 weeks therapy, 6 weeks: output outcome after 6 weeks therapy.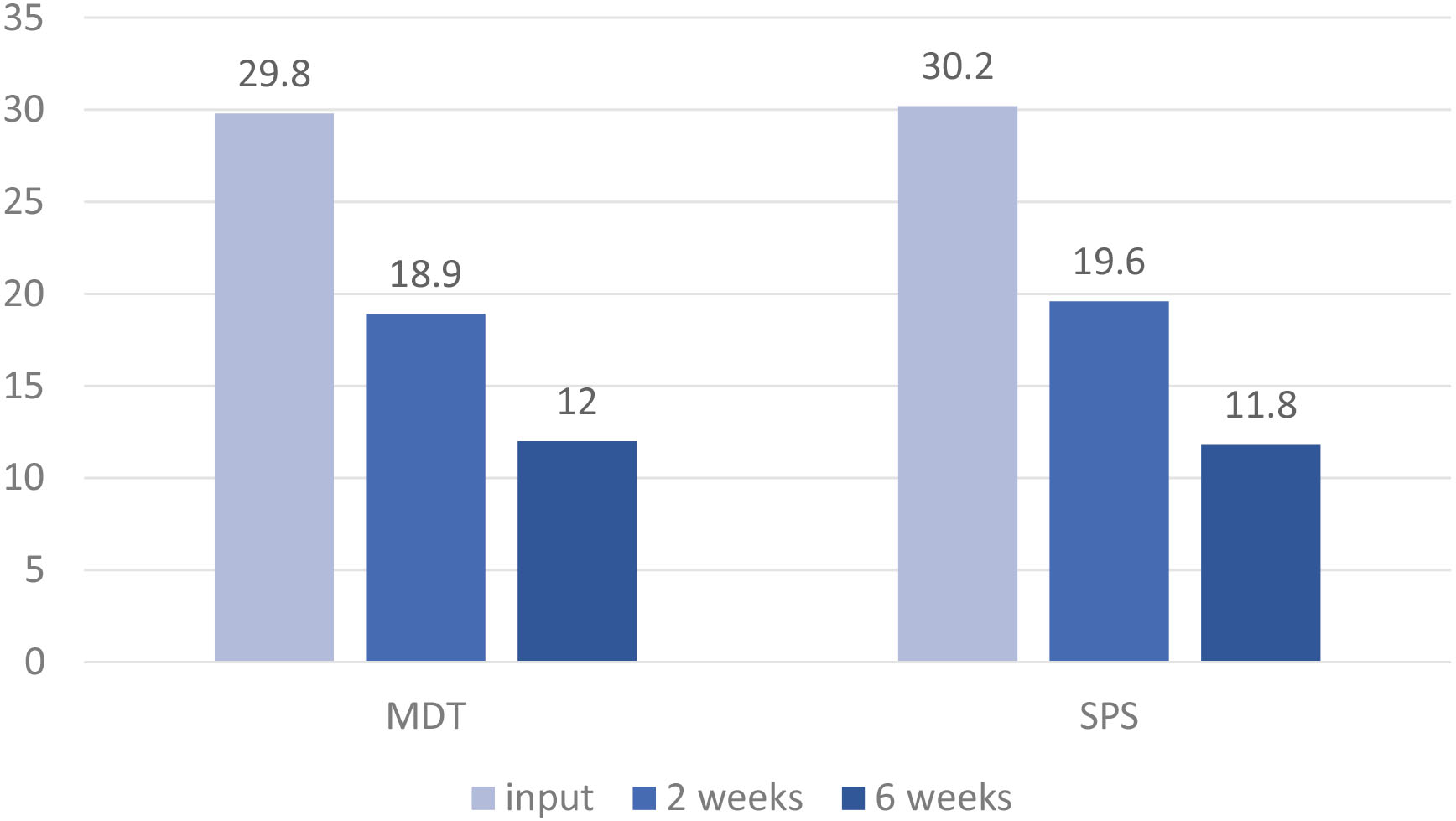
The second group of patients was taught a set of exercises from the method of Spiral Stabilization of the spine as part of physiotherapeutic treatment, which were chosen after the initial examination, based on their health condition. These patients belonged to the second and third group (subacute phase, healing phase). After that, probands were instructed about exercise at home and the principles of the Back School [15]. They usually practiced a set of recommended exercises 2–3 times a day: in the morning, in the evening, or even in the afternoon. At each following visit to the physiotherapist the correctness of the exercise(s) practiced at home was checked, and then, based on the patient’s current health condition, additional exercises were added.
A physiotherapy program was created individually for each patient in both groups, according to their current health condition. All patients underwent individual kinesiotherapy (MDT, SPS) under the supervision of a physiotherapist once a week, a total of six times.
Managing with daily activities and functionality were evaluated through The Aberdeen Back Pain Scale [16] and disability through the Roland-Morris Disability Questionnaire [17]. These questionnaires were filled in three times by patients in both groups: at the beginning of the treatment process during initial examination, after 2 weeks of treatment and for the third time after six weeks when the treatment process finished. The Aberdeen Low Back Pain Scale is a questionnaire that is considered reliable [18], well validated and therefore recommended for use without further validation studies [19]. It contains 19 questions that monitor how pain affects the management of various daily activities and functionality (self-care, gait, sitting, standing, sports activities, housework, rest, sleep, bending, sexual activity), pain and the distribution of symptoms in patients with LBP. 0–5 points are added for each question. The lowest score, 0 points, indicates the highest ability to perform activities and the highest level of functionality, and the highest score of 76 points indicates their maximum limitation. The Roland-Morris Disability Questionnaire assesses disability and contains 24 simple and easy-to-understand questions that monitor the ability to perform daily activities, the presence of auxiliary actions (use of railings when walking up stairs, etc.), need of help from other people and mental condition (irritability). For each question there is a choice of yes or no answers, with one point added to the total score for a positive answer. The highest score (24) expresses maximum disability, the lowest score (0) expresses no disability.
Data analysis
The data collected through the questionnaires were statistically processed through the STATISTICA 12 statistical program. The Shapiro Wilk test was used to verify the normality of the sample distribution.
To verify the success of treatment after two and six weeks, and to determine the significance of the differences between input and output results, Friedman’s nonparametric test was used for both examined parameters and with both groups of patients. The output results collected after two and six weeks of treatment were statistically evaluated for each parameter in both tested groups (MDT, SPS) and for each parameter separately using the Mann-Whitney nonparametric test.
Comparison of the outcome between the two groups after 2 and 6 weeks of treatment
Comparison of the outcome between the two groups after 2 and 6 weeks of treatment
The average values of input and output outcomes of the Roland-Morris Disability Questionnaire. MDT: group of patients with McKenzie therapy, SPS: group of patients with Spiral Stabilization therapy, input: input outcome, 2 weeks: output outcome after 2 weeks therapy, 6 weeks: output outcome after 6 weeks therapy. 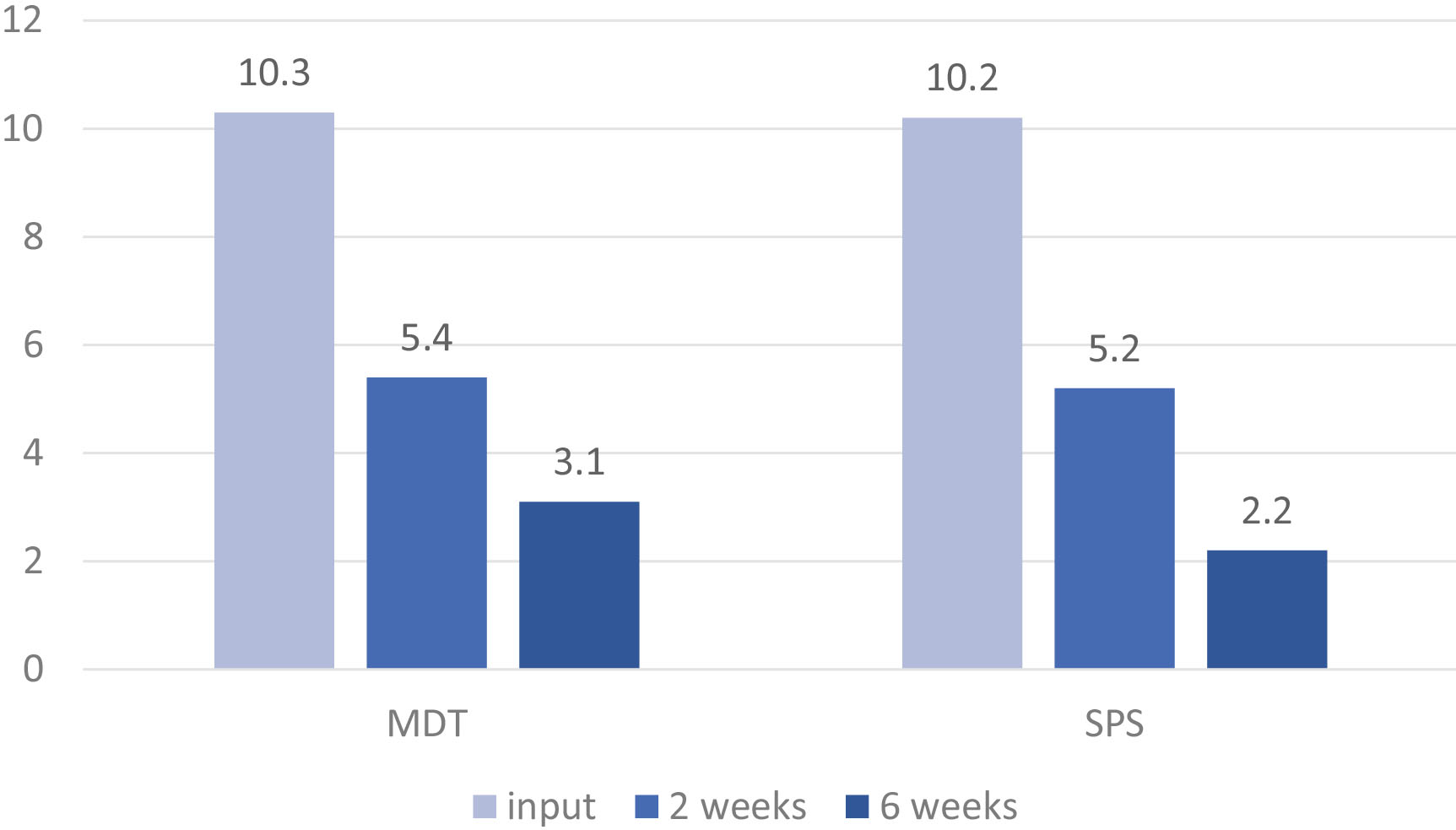
By comparing the input and output data, it was found that the health condition improved in both groups of patients after two and six weeks of treatment (Figs 1–2). There was an improvement in the management of daily activities and functionality, as well as a reduction in disability in both groups of patients (Tables 1–2). Based on the comparison of the medians of the output results in the individual examined parameters, it is clear that in both groups of patients, 6 weeks of treatment was more effective than 2 weeks. The statistical analysis of input and output results of two and six weeks treatment in the group of patients treated by the MDT therapy method showed statistical significance difference
Similarly, in the group of patients treated by Spiral Stabilization therapy, it found a statistical significance difference of
The results of the statistical processing thus show that after 2 or 6 weeks of treatment there was no significant difference in the management of daily activities and functionality and disability between both groups (Table 3).
Discussion
The McKenzie Method uses static and dynamic exercises, as well as the concept of progression of forces and pressures to mechanically influence the single structures of the kinetic segments of the spine.
The Spiral Stabilization Method mainly uses muscle spirals in therapy. Based on this fact, it may be assumed that the effect of the McKenzie Method will be more effective in patients with LBP compared to the SPS method. But that was not confirmed. The reason for the rapid and comparable improvement of the condition of patients in both groups may be their active and conscientious approach to treatment and home exercise; but especially the fact that the research sample consisted of patients with a vertebrogenic pain syndrome of functional etiology. Functional disorders are not based on a pathomorphological background and therefore are easier to manage therapeutically compared to morphological disorders.
The MDT Method is globally recognized and established. Its effect on the beneficial influence of LBP is confirmed by many studies [20, 21, 22, 23]. Similarly, our study showed a positive effect, when the improvement of the monitored parameters was significant after two and six weeks of treatment (
As the results of this study show after two and six weeks of treatment, both of the applied methods had a comparable effect (
Similar results were obtained by Hasanpour-Dehkordi et al. in their randomized study [26]. They compared the effect of the Pilates and McKenzie Methods. The study included 36 patients with chronic low back pain. They were voluntarily divided into three groups of 12 people: the Pilates group, the McKenzie group, and the control group. The Pilates group participated in a 1-hour exercise, 3 times a week for 6 weeks. The McKenzie group exercised 1 hour a day for 20 days. The control group was not treated. The authors rated the overall health of all participants using the General Health Questionnaire 28 and pain using the McGill Pain Questionnaire. There was no significant difference in pain relief after the Pilates and McKenzie treatment finished (
Lam et al. [27] also reached similar results in their review of the literature. They used meta-analysis identified randomized controlled trials to research the effect of MDT in patients with LBP from six databases. Of the 17 studies that met the inclusion criteria, 11 provided valid data for analysis. They found that there was moderate to good evidence that MDT was no better than other rehabilitation interventions to reduce pain and disability in patients with acute LBP. In patients with chronic LBP, there is medium to high quality evidence that MDT is superior to other rehabilitation interventions in reducing pain and disability. However, it depends on the type of intervention compared to MDT.
Other authors also arrived at interesting results. Alhakami et al. [28] in their qualitative review focused on comparing the effect of the McKenzie Method and stabilization exercises in patients with chronic LBP. From six databases, 829 articles were found, out of which 10 randomized controlled trials were finally selected. Of these ten, only two studies compared stabilization exercises and McKenzie in the treatment of chronic nonspecific LBP. Therefore, there is insufficient evidence for any convincing comparison of the effects of McKenzie and stabilization exercises regarding this disease. However, both McKenzie and stabilization exercises were superior to conventional exercise programs to reduce pain and functional disability in patients with chronic nonspecific LBP.
The findings of the current study are supported by the literature, which proves that the McKenzie Method in this particular group of patients represents a safe and effective treatment for vertebrogenic pain syndrome. Our results pointing to the effectiveness of the SPS Method are not supported by the literature. The databases available to us (PubMed, ProQuest, Scholar Google) do not publish works related to this issue. This makes the results of this study original and point to another alternative in the treatment of back pain.
Conclusion
The results of this study showed that the treatment by McKenzie and Spiral Stabilization in patients with vertebrogenic pain lumbar syndrome has a significant effect on improving the management of daily activities and physical functions as well as reducing disability. Both methods showed a more significant effect after six weeks of therapy compared to two weeks. But none of the methods was proven to be better when compared to each other, as they have a similar effect on reducing disability and improving the management of daily activities and functionality. That said, they are equally effective in patients with vertebrogenic pain lumbar syndrome.
Footnotes
Conflict of interest
The research is not funded, and the authors have no conflicts of interest to report.
Ethical declarations
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. The study was approved by the Ethics Commission of the Factulty of Health Care on 14 May 2019 (no. 2/2019)