
Abstract
BACKGROUND:
Several biomechanical outcomes are being used to monitor the risk of injuries; therefore, their reliability and measurement errors need to be known.
OBJECTIVE:
To measure the reliability and measurement error in lower limb 3D gait analysis outcomes during a 90
METHODS:
A test re-test reliability study for ten healthy recreational players was conducted at seven-day intervals. Kinematics (Hip flexion, adduction, internal rotation angles and knee flexion abduction angles) and kinetics (Knee abduction moment and vertical ground reaction force) data during cutting 90
RESULT:
The ICC values of the kinematics, kinetics, and vertical ground reaction force (VGRF) outcomes (90
CONCLUSION:
The current study results support the use of kinematics, kinetics, and VGRF outcomes for the assessment of knee ACL risk in clinic or research. However, the hip internal rotation angle should be treated with caution since the standard measurement error exceeded 10% compared to the mean value. The measurement errors provided in the current study are valuable for future studies.
Keywords
Introduction
An anterior cruciate ligament (ACL) injury is considered one of the most devastating injuries in sports [1]. The annual prevalence of ACL injury among recreational athletes has been found to range between 0.03% and 1.62% [2]. A more recent systematic review and meta-analysis showed an incidence proportion of 3.5% for females and 2% for males and an incidence rate of 1.5/10000 and 0.9/10000 for ACL injury over a period of one session to 25 years [3]. ACL injury has been linked to the development of knee osteoarthritis (OA). A previous systematic review showed a seven to eight times increase in the likelihood of developing OA after ACL in around 10 years [4]. This fact highlights the importance of identifying risk factors and designing a preventive program to reduce this injury.
Previous studies have shown that increasing the knee external abduction moment and knee valgus angle (abduction angle) will lead to a higher risk of noncontact ACL injury [5, 6, 7]. Moreover, it has been found that ACL is under great stress when the knee extension is combined with a high increase in the valgus moment, angle, and internal tibial rotation [8, 9]. In addition, previous studies have shown that increasing the knee valgus angle and external abduction moment is associated with the hip positioned in more flexion, abduction, and internal rotation [10, 11, 12]. A recent study showed that a reduction in the knee flexion angle and a higher vertical ground reaction force are associated with increased ACL injury risk [13]. The previously mentioned variables were identified from activities associated with a higher risk of ACL injury, such as a change of direction (COD).
COD manoeuvres are essential and crucial in many sports, such as soccer. Unfortunately, it can lead to a noncontact ACL injury [14, 15]. In addition, COD is related to both ACL risk and sports performance [16] and has been used to assess the risk of injury and to identify talented individuals [17]. The high prevalence of ACL injury has led to the development of a preventive program that targets biomechanical risk factors to reduce the risk of injury [18, 19]. Such a program’s effect on biomechanical variables can be measured using a three-dimensional (3D) gait analysis system commonly used in lower limb biomechanics and is considered a gold standard [20, 21, 22]. However, before using any outcome to assess the risk of ACL injury, its reliability [23] and measurement errors should be known. This knowledge will let the researcher know if the change passes the measurement error and is considered a real change.
Although researchers investigated the reliability of lower limb biomechanical outcomes during COD manoeuvres at 45
Method
The current study is a reliability study that gained ethical approval from the Salford University ethical committee under ethical number HSCR16–88 (approval date: 13/9/2016). The research complied with all relevant national regulations and the Declaration of Helsinki.
Anatomical and tracking markers and joint location definition used in current study
Anatomical and tracking markers and joint location definition used in current study
To be enrolled in the study, a participant must be of the general population, healthy, and physically active. The participant must be a recreational, non-elite soccer player who practices soccer for at least 30 minutes three times a week over the last six months in regular basis. Moreover, each participant had to practice 90
Procedure
A Qualisys motion analysis system (Gothenburg, Sweden) with ten cameras (Qualisys Oqus 700+) synchronized with three force platforms (AMTI BP400600, USA) operating via Qualisys Track Manager software (version 2.16) was used. The sampling rate was 250 Hz for kinematics and 1000 Hz for kinetics. Participants were tested twice at the same time of the day, one week apart. The selection of a time interval in reliability depends on whether the time should be enough to reduce recall bias and not too long to cause real change. Based on previous similar studies, seven-day intervals were selected [20, 30].
Before the participants arrived in the lab, the lab was calibrated. A supervisor familiar with specialised techniques manages the lab and calibrates the force platform to ensure that it runs perfectly regularly. The calibration process starts by placing the L-shaped metal frame in a previously specified place along the corner of one of the force platforms. Then, the wand is waved randomly in the required volume. For the calibration to be accepted, it must get residual volume below 1 mm for each camera based on the manufacturer’s recommendation.
Upon the participants’ arrival, the experiment was described, and consent forms were distributed and obtained after providing enough time for participants to think, ask questions, and decide. Demographic characteristics (age, mass, height) and previous medical histories were taken. Then, each participant was asked to change into shorts and a T-shirt. Standardized shoes (New Balance, UK) were used to reduce the possibility of interaction between shoes and the surface. The Calibrated Anatomical System Technique (CAST) method was used to place the markers [31], as shown to reduce error compared to an earlier model [32]. The CAST model allows for two sets of 14.4 mm markers (technical marker, anatomical marker). The anatomical marker is used to define the local coordinate system in relation to the anatomical frame, while the technical marker is used to track movement. The segment was defined by the proximal and distal endpoints (Table 1) [33]. Four clusters were attached securely with a Velcro strap in each participant’s shank and thigh in an anterior lateral direction (Fig. 1). Each participant was given enough time to practice until they felt comfortable and natural. The static trial was captured, and after that, static markers were taken off [34].
Example marker placement for one participant.
To perform the required task, participants were asked to run in a straight direction for five meters, and when they hit the force platform by the required limb, they changed the direction (90
Experimental setting with cones placed at 90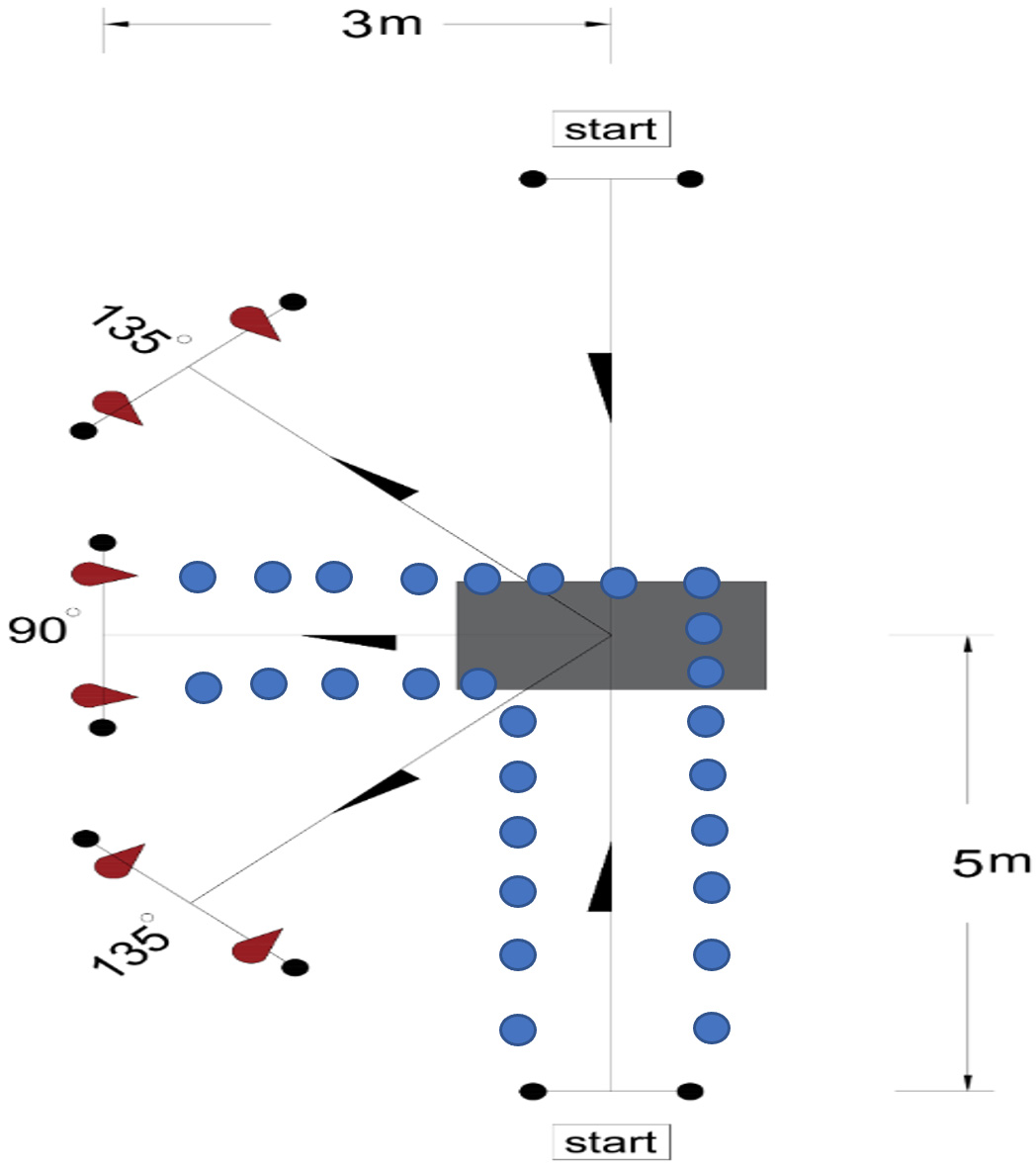
Peak vertical ground reaction force (VGRF), peak knee flexion angle and peak abduction angle, peak external knee abduction moment (KAM), peak hip joint flexion, adduction, and internal rotation angle outcomes were selected. The rationale for choosing these outcomes is that higher VGRF will lead to higher KAM, and a previous study showed an increased risk in ACL with higher VGRF [13]. An increase in the knee abduction angle has been linked to an increased risk of ACL injury and KAM increase [16, 37]. In the sagittal plane, reducing the knee flexion angle has been linked to increasing ACL loads [13]. A higher KAM leads to an increase in the tension on the ACL and an increase in the risk of injury [16]. A previous review highlighted that the sagittal plane hip had been linked to the occurrence of ACL injury [16]. In contrast, transverse plan hip motion has been linked to increased abduction through dynamic valgus [16]. Moreover, the increase in the hip adduction angle was found to be a significant predictor for the knee abduction angle [11].
Between days reliability (ICC, SEM) for 90
COD manoeuvres
Between days reliability (ICC, SEM) for 90
ICC
Between days reliability (ICC, SEM) for 135
ICC
The raw data were captured and labelled through Qualisys Track Manager Software (version 2.16). After labelling, each trial was exported as a visual 3D file to be processed in Visual 3D (Version 6.00.16, C-Motion Inc., Rockville, MD, USA). In Visual 3D, the kinematics and kinetics data were filtered by a 25 Hz and 12 Hz Butterworth fourth-order bi-directional low pass filter, respectively, and interpolated for ten frames. This filter cut-off was selected based on previous studies [38, 39].
The lower extremity model was then created and modelled as a conical frustra using the inertial parameters estimated via the anthropometrics data. X-Y-Z Euler rotation sequences were used to process the joint kinematic angles, where X represents flexion-extension, Y means abduction-adduction, and Z represents internal-external rotation [40]. The joint kinematic data were calculated based on inverse dynamics theory. Joint moments were normalised on body mass and presented as an external moment, while kinetics and kinematics data were normalised on 100% of the stance phase. Initial contact was defined as the point when VGRF exceeds 20 newtons, while toes off when VGRF falls below 20 newtons [20].
Statistical analysis
The required sample was calculated based on a previous method published in 2018 [41]. The minimum accepted reliability value for ICC was 0.40 in the equation. The expected reliability value for the ICC was between 85 to 95 with 90% power, which shows that the required sample size ranged from 7 to 17 participants.
The statistical analysis was conducted using Statistical Package for Social Sciences (SPSS) software version 21. The mean of the five trials from both visits was used to calculate reliability. An ICC two-way mixed model with absolute agreement was used since only one investigator conducted all the measurements [42]. The ICC model was interpreted according to the following criteria: 0.40 to 0.70 fair, 0.70 to 0.90 good and 0.90 and above excellent [43]. The confidence interval (CI) and standard deviation (SD) were also calculated and presented. Moreover, the standard error of measurement (SEM) was calculated since the ICC cannot alone provide any indication of the level of disagreement [23]. SEM was calculated based on the following formula: SD* SQR(1-ICC) [44]. SQR can be defined as a square root. SEM provides a number with the same unit for the outcome measure, with a lower value indicating low measurement error. The mean of both visits and absolute difference between visits were calculated.
Results
Ten healthy male recreational soccer players were recruited for the current study. The sample’s age, height, mass, and body mass index (BMI) were 22
The reliability of 90
COD manoeuvres
Table 2 represents the between-day reliability for 90
135
COD manoeuvres reliability
Table 3 represents the between-day reliability for 135
Discussion
The current study aimed to investigate the between days’ reliability of lower limb 3D gait analysis outcomes during 90
The ICC values ranged from 0.85 to 0.98 for COD manoeuvres (90
In addition, VGRF showed a high reliability value with low measurement error in both tasks (90
One of the essential measurements in reliability is the measurement error since it help to estimate the range in which the true value lie [44]. Gaining such value is essential, especially in follow-up sessions, such as post-treatment. Knowing SEM allows the researcher to know that if observed improvement exceeds the measurement error, it is considered a real improvement [50]. The current study showed that in the joint angle, the value for standard error of measurement was between 0.44
The result of the current study is subjective to limitations. First, the generalizability of the results is limited to settings like the laboratory, researcher ability, and the model used. Second, the shoe used in the current study (Mondo) was standard, which may be uncommon, and the interaction between the shoe and floor may not be similar to that between shoe and grass. An effort was applied by providing time for familiarization until participants felt natural with the shoe. However, there is a need for a study that will investigate the effects of real sports shoes on grasses. Interestingly, only intrarater reliability was investigated in the current study; therefore, future studies should investigate interrater reliability and calculate minimal detectable change. Finally, the present study sample was a recreational healthy soccer player; therefore, the result may not apply to those elite players, and more studies need to investigate such a population.
Conclusion
Change of direction manoeuvre is associated with a higher risk of ACL injury caused by an increase in knee abduction moment and change in kinematic and kinetic variables. However, for such an outcome to be used in the clinic and field, it must be reliable. The current study showed that all the biomechanical outcomes measured in 90
Footnotes
Acknowledgments
The authors appreciate the participants who devoted their time and contributed invaluably to the study.
Conflict of interest
The authors declare no conflicts of interest.
Funding
The authors report no funding.