
Abstract
BACKGROUND:
Gluteus medius (GM) is a segmented muscle involving three muscular subdivisions. Rehabilitation exercises has been suggested to strengthen specific subdivisions.
OBJECTIVE:
This study aimed to evaluate muscular activation of the anterior, middle, and posterior subdivisions of the GM during two different exercises.
METHODS:
A total of 28 healthy active subjects participated in this study. Muscle activity using surface electromyography was recorded for the three GM subdivisions during figure-of-four position (FFP) and wall press (WP). Non-parametric Kruskal-Wallis test was used to detect differences between GM subdivisions on each exercise and the Mann-Whitney
RESULTS:
There were statistically significant differences (
CONCLUSION:
In line with the WP exercise, the FFP produces sufficient activity to provide potential strength gains on the posterior subdivision and could be a viable option to include in the early stages of the rehabilitation process. Clinicians may use this information to make more informed decisions about exercise selection for strengthening specific GM subdivision.
Introduction
As a single muscle, the gluteus medius (GM) acts as primary hip abductor [1, 2] and has an important role in pelvic stabilization and lower limb motion control [3, 4, 5]. It is a key muscle in stabilizing the hip during single-limb stance to prevent the contralateral pelvis dropping and is critical to controlling hip adduction and internal rotation during weight-bearing activities [4, 6, 7]. However, cadaveric and electromyographic studies have described the GM as a segmented muscle involving 3 muscular subdivisions (anterior, medium and posterior) [8], with distinct functions and different muscular activities [7, 9, 10]. All 3 GM subdivisions act as hip abductors, whereas the posterior subdivision also acts as an external rotator [11, 12]. Therefore, weakness or decreased activation of the posterior GM subdivision could result in increased hip adduction and internal rotation during functional activities [12] noted in persons with lower extremity musculoskeletal injuries [6, 13, 14], including iliotibial band syndrome [15], anterior cruciate ligament [16] and particularly patellofemoral pain (PFP) [17, 18].
Previous studies reported conflicting results regarding electromyographic (EMG) activity of the three GM subdivisions in individuals with PFP, when compared with matched controls. Cowan et al. [18] found that individuals with PFP had delayed onset of anterior and posterior subdivisions during a stair-stepping task and O’Sullivan et al. [19] reported similar activation levels between PFP and healthy subjects in all GM subdivision during different weight-bearing exercises. Interestingly, O’Sullivan et al. [19] also found that the posterior subdivision was always less active during all exercises performed by the PFP group supporting the hypothesis that PFP patients may present poor dynamic external rotation of the hip [14, 20].
Based on the apparent association between GM weakness and lower extremity dysfunctions, the exercise therapy has been advocated as the intervention of choice for PFP [21, 22, 23]. Some rehabilitation protocols for PFP are focused on the GM subdivisions [24, 25] suggesting specific weight-bearing exercises targeting the posterior subdivision to improve pelvic stability and control the excessive hip internal rotation [26, 27]. Among those exercises, the wall press (WP) exercise is highly recommended for the treatment sessions and previous EMG studies have shown that it is particularly effective on the activation of the GM posterior subdivision compared with other weight-bearing exercises [19, 28]. However, non-weight-bearing exercises are often initiated to target a specific muscle or used at the initial stages of the rehabilitation when patients are unable to perform weight-bearing exercises [29, 30]. The figure-of-four position (FFP) is a suggested non-weight-bearing exercise for early stages when PFP patients presents a marked internal femoral rotation and difficulties in activating the GM on a standing position [25, 31]. During the exercise patient is asked to contract the gluteal muscle in inner range for some seconds [26, 27]. As a result of this isometric contraction, it should be expected a greater activation of the gluteal muscle, especially the posterior subdivision of the GM due to its horizontal fiber orientation [4, 10, 32]. Clinicians trend to suggest hip strengthening exercises based on knowledge of anatomical structure and function, whereas no evidence exist to confirm the exact role in activating particular muscles during a specific movement. In this regard, a study on the ability of the FFP exercise in activating the GM subdivisions is needed.
Among common weight-bearing exercise, previous EMG studies support the WP as the most effective exercise to activate the GM, especially the posterior subdivision [19, 28], whereas a limited information exists regarding non-weight bearing exercises. Since the WP (weight-bearing exercise) and FFP (non-weight bearing exercise) are suggested for the same purpose at different stages of the GM exercise program, a study to identify differences in EMG activity among each GM subdivisions between both exercises could add valuable information, helping to guide the decision-making process for GM exercise prescription and progression in the management of PFP patients.
Therefore, the first aim of this study was to evaluate the muscular activation of the three GM subdivisions during the FFP and WP exercises in healthy subjects using surface electromyography (sEMG). The study also aimed to identify which exercises produced greater activity in all GM subdivisions. We hypothesized significant differences among GM subdivisions in both exercises. Based on previous studies, we also hypothesized that the WP exercise generates greater activity compared to the FFP, particularly in the posterior subdivision.
Material and methods
Study design
This was a cross-sectional study reported following the STROBE guidelines.
Participants
Thirty healthy participants (8 male, 22 female) volunteered for this study. They were recruited from the local university campus community using email invitations, posters and flyers. Participants were included in the study if they had between 18–30 years [28, 33] and presented at least a moderate level of physical activity using International Physical Activity Questionnaire (IPAQ). Participants were excluded if they had history of surgery or significant back or lower extremity dysfunction requiring treatment in the past 6 months [28, 33]. Written informed consent was obtained from all participants. Sample size calculation was performed using ClinCalc software online program (
Electromyography
An sEMG system was used to measure the activation levels of each GM subdivision during two distinct exercises: FFP and WP. Disposable pre-gelled stick-on surface electrodes in a bipolar configuration were placed at an interelectrode distance of 20 mm. The electrodes were connected to 8-channel EMG unit (PhysioPLUX – PLUX
Exercises
All exercises were performed with the dominant leg, identified by which leg the participant used to kick a ball [30]. The order in which they were performed was also randomized using the same randomization tool. Each participant was given a short description and demonstration of the exercises and given time to practice until they demonstrated ability. This instruction was completed by an experience member of the research team. Before data collection the participants rested for 5 minutes to prevent possible fatigue. For the FFP exercise the participant lies in prone with the hip of the dominant leg abducted, externally rotated and extended position. The non-dominant leg is extended and lies on top of the bent leg. The malleolus of the underneath leg is at the level of the tibial tubercle. The participant attempts to flatten the abducted and rotated hip by pushing along the length of the thigh and sustain gluteal isometric contraction for 5 seconds during each trial (Appendix) [26, 27]. Standardized verbal encouragement was given to each participant to ensure a maximum contraction [37]. For the WP exercise, participants were instructed to stand next to a wall with the dominant leg furthest from the wall. They were then asked to assume a single leg stance position by flexing their non-dominant side hip to 60
EMG acquisition and processing
The EMG data was stored on a personal computer and processed using OpenSignals (r)evolution software (PLUX – Wireless Biosignals
Statistical analysis
Analyses were performed using IBM Statistical Package for Social Sciences (SPSS) 28.0. Non-normal distribution of data was verified with Shapiro-Wilk test, so data were analyzed with non-parametric tests. Mann-Whitney U test for independent samples was used to compare the muscular activation of each GM subdivision between exercises, and the Kruskal-Wallis test to compare muscular activation between GM subdivisions on each exercise. All data were expressed as median and inter-quartile ranges. The significance level was set at
Results
From the 30 initially recruited volunteers, two were excluded due to problems with EMG data storage. Thus, data from 28 participants were included in this study. The participants’ demographic characteristics are presented in Table 1.
Demographic characteristics of the participants (
28)
Demographic characteristics of the participants (
Legend: SD
Differences between muscular activation of the GM subdivisions during figure-of-four position and wall press exercise (values are expressed as %MVIC)
Legend: GM
Differences between exercises on muscular activation of the MG subdivisions (Values are expressed as %MVIC)
Legend: FFP
Table 2 summarizes the differences between muscular activation of the GM subdivisions in both exercises. The results showed statistically significant differences between all three GM subdivisions during the FFP (X
Muscular activation of the GM subdivisions during figure-of-four position and wall press exercises.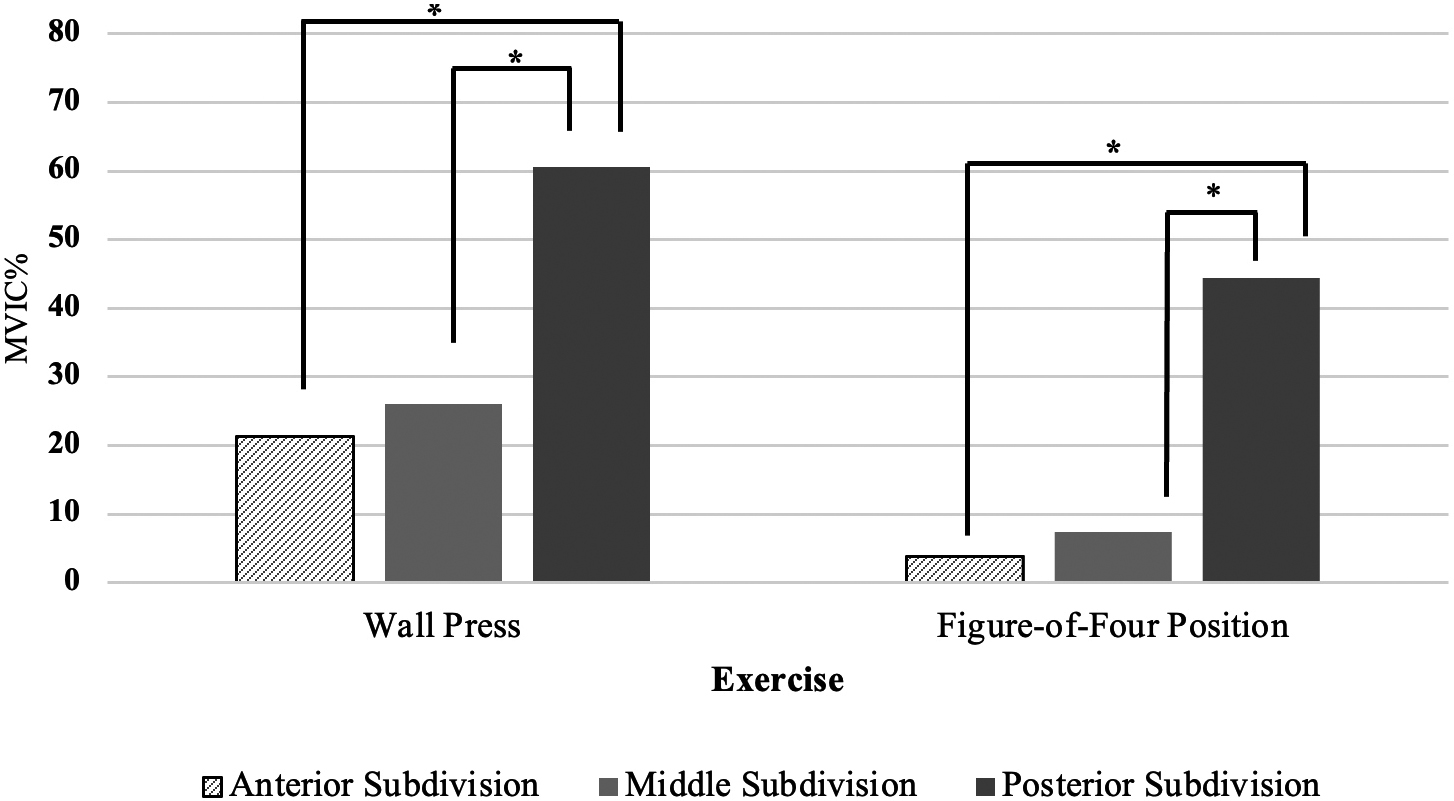
The results in Table 3 seem to confirm the initial hypothesis were there was a statistically significant superiority of the WP exercise in activation of the posterior subdivision rather than FFP exercise (U
The primary purpose of this study was to compare the muscular activation of all three GM subdivisions during WP and FFP exercises, using sEMG. Regardless of the nature of these exercises, the results of the present study showed that the activation of the GM subdivisions was not homogeneous during the exercises, confirming significant differences in EMG activation between the anterior, middle, and posterior subdivisions. These findings seem to support the idea that all GM subdivisions have distinct functional actions when performing different exercises, as described by previous studies [1, 2, 4, 7, 28]. Moreover, we also observed higher activation of the posterior subdivision, compared to middle and anterior subdivisions in both exercises.
In the FFP exercise, the posterior subdivision activated substantively more (44% MVIC) than the middle (7% MVIC) and anterior subdivisions (4% MVIC). This may relate to the fact that the tested leg is initially positioned in abduction and external rotation, facilitating greater isometric activation of the posterior subdivision due to a more horizontal trajectory of its muscle fibers. Previous literature indicates that EMG amplitudes between 40–60% MVIC provide an effective stimulus to strengthen the GM muscle [37, 39]. Some authors have been suggesting that patients who are unable to perform weight-bearing exercises can effectively strengthen the GM with a non-weight-bearing exercise [30, 40]. In this sense, the results of the present study seem to suggest that FFP is an effective non-weight-bearing exercise to strengthening the posterior subdivision and that it can be considered in the initial stages of the GM training programs in management of PFP patients.
To our knowledge, this was the first study to evaluate the activation of the GM subdivision during FFP exercise, and comparison with other studies could not be made. Current research is mainly focused on weight-bearing exercises [4, 7, 28], hip isometric contractions [2, 41] and manual strength testing [3], whereas a limited information exist on the muscular activity of the GM subdivisions during non-weight-bearing exercises. Nevertheless, Semciw [42] and Moore [43] examined the ability of the clam exercise on the activation of GM individual subdivisions and interestingly found greater activation levels of posterior subdivision relative to the middle and anterior subdivisions. However, both studies used fine wire electrodes, which compromises any assumptions or direct comparisons with the results of the present study.
As expected, the WP exercise was also more demanding on the activation of the posterior subdivision (61% MVIC) compared to the middle (26% MVIC) and anterior (21% MVIC) subdivisions. These results seem to be in line with previous studies [4, 28], supporting the idea that the WP is an effective isometric strengthening exercise for the GM and especially the posterior GM subdivision. However, there is a wide variation of EMG values across all GM subdivisions between these previous studies and the present study that need to be considered. In fact, O’Sullivan [28] concluded that the WP exercise effectively activated all GM subdivisions, reporting EMG amplitudes of 76%, 38% and 27% MVIC for the posterior, middle and anterior subdivisions, respectively. A reason for these differences may be related to distinct methodological approaches affecting the interpretation and comparison between studies. According to Macadam [40], a precise EMG activity comparison between studies should at least consider identical methods to collect and record the MVIC. While we used the normalization of the EMG signal through manual resistance tests with the participants lying on a treatment table, O’Sullivan [28] established the MVIC in a standing position using an isokinetic dynamometer, which compromises an assertive comparison between EMG amplitudes. Furthermore, we elected the average of the 3 repetitions to record the MVIC of each GM subdivision whereas O’Sullivan [28] and Ju [4] used a more demanding normalization protocol by choosing the highest EMG value of the 3 repetitions. For this reason, it should be expected lower %MVIC values in their studies, however, it only occurred in the study of Ju [4], where the WP exercise produced the lowest activation of all GM subdivisions.
The results of this study add value to the existing literature confirming that the GM subdivisions work in distinct ways and the EMG activity levels can be affected by the nature of the exercises (weight-bearing vs non-weight-bearing). Additionally, both exercises appear to be effective decisions for strengthening the GM, especially the posterior subdivision. The FFP and WP exercises produce sufficient activity (greater than 40% MVIC) in the posterior subdivision and inferences can be made about their potential for strength gains as a non-weight-bearing and a weight-bearing exercise, respectively. However, when comparing both exercises, the WP exercise was the most effective in activating the posterior subdivision. Moreover, among other weight-bearing exercises, the WP was also more effective in targeting the posterior subdivision in healthy [19, 28] and PFP subjects [19]. This information may enable physiotherapists to develop specific exercise programs for each GM subdivision in the management of PFP since prior research has identified deficits in muscular recruitment [18] and activity [19] in more than one GM subdivision in patients with PFP.
The present study expands the understanding of the muscular activation of the three GM subdivisions during exercise, thereby providing clinicians with evidence to support its selection in many other musculoskeletal conditions where the GM is weak or atrophied [43]. For example, patients with balance disorders or patients who have recently sustained a hip injury or surgery [33, 44] and are unable to perform weight-bearing exercise, the non-weight-bearing exercises can be appropriate introductory exercises to effectively strengthen the GM. However, further research is needed to evaluate the muscular activity of the GM subdivisions during other common exercises and conducted on clinical population.
Our study has several strengths. sEMG is commonly used as a non-invasive method to evaluate muscular activity and our laboratory has experience with this technique [45, 46]. Furthermore, in our study protocol the participants perform the MVIC and the exercises in a random order minimising the effects of cumulative fatigue on the GM subdivisions. Additionally, the use of an adequate sample size is also a strength, since other similar studies includes less participants [4, 28]. This study also has some limitations that should be addressed. Measurement using sEMG is influenced by crosstalk from nearby muscles or even adjacent muscle subdivisions that can affect the results [4, 28]. This limitation is inherent to all sEMG studies, and we attempted to minimize these factors by applying standard skin preparation, using a small interelectrode distance [47], all electrodes were placed by the same examiner and properly securing the electrodes to prevent movement [30]. Furthermore, anatomical landmarks were confirmed by a second experienced examiner [28] and a standardized electrode placement was chosen based on previous GM subdivisions sEMG studies [4, 19]. Despite these measures, some crosstalk might have occurred between muscles.
Our participants were healthy and physically active, thus limiting the generalization of our results to symptomatic individuals. Further research must be conducted on patients with musculoskeletal conditions or other pathologies to increase the clinical applicability of our findings. The present study evaluated only the muscular amplitude of GM, and not the muscular time activation, which is an important factor to consider in future studies [28]. Possible delays in pre-activation of the GM muscle have been previously reported in PFP patients during several functional activities [48]. All participants performed the exercises with the dominant leg, which may have inflated the levels of muscle activation. Future studies should evaluate common GM exercises using both legs to extend the clinical significance of our findings. In addition, we did not measure the force applied by the subjects during exercises, thereby we cannot guarantee that all participants applied the same force.
Conclusion
The results of this study support the hypothesis that the GM subdivisions have distinct functional actions and the muscular activity levels can be influenced by the nature of the exercises. This is the first study to evaluate the ability of the FFP exercise in activating the GM subdivisions. As in line with the WP exercise, the FFP produces sufficient activity to provide potential strength gains on the posterior subdivision. Furthermore, this non-weight-bearing exercise could be a viable option to include in the early stages of the rehabilitation process of patients with PFP and other musculoskeletal conditions. This information can be used to make more informed clinical decisions about exercise selection for strengthening specific GM subdivision. However, further studies focused on other common exercises and clinical populations are needed to increase the clinical applicability of our findings.
Ethics statement
Ethical approval was obtained from the Ethics Committee of the Polytechnic Institute of Setúbal (07A/ LN/2017).
Funding
The authors gratefully acknowledge the financial support from the Polytechnic Institute of Setubal.
Informed Consent
Informed consent was obtained from all participants in the study.
Author contributions
MJ was involved in planning and supervising the work, data collection, analysis and prepared the manuscript. IS was involved in data collection, processing data, performing analysis, preparing tables and figures, and interpretation of the results. MGS was involved in planning and supervising the work and manuscript development. All authors reviewed and approved the final manuscript.
Supplementary data
The supplementary files are available to download from https://dx-doi-org.web.bisu.edu.cn/10.3233/BMR-220188.
Footnotes
Acknowledgments
The authors would like to thank their colleagues of the Musculoskeletal Research Group, Setubal, Portugal, for their support and contribution to this work.
Conflict of interest
The authors declare that they have no conflict of interest.