
Abstract
Primary hepatic angiosarcoma (PHA) is a rare malignancy with a badly poor prognosis. The extremely low morbidity and untypical clinical manifestations conduce to a missed diagnosis. The present study reported a case of an adult male patient who was pathologically confirmed to be PHA, which mimicked intrahepatic cholangiocarcinoma on conventional ultrasound and contrast-enhanced ultrasound. Findings on various imaging examinations were carefully evaluated and the associated literatures were also reviewed.
Keywords
Introduction
Primary hepatic angiosarcoma (PHA) accounts for up to only 2% of primary hepatic tumors [1, 5] but it is the most common malignant mesenchymal tumor of liver [20, 26]. PHA is a highly malignant tumor, and portends a poor prognosis. Most patients progressed rapidly and died within a year of diagnosis [16, 17]. Most patients may be asymptomatic at first, who often be misdiagnosed as atypical hemangioma by imaging studies. When the symptoms showed up, that tended to be nonspecific, including abdominal pain, fever, anorexia, weight loss and fatigue [17, 27], and the disease usually was at an advanced stage. The absence of specific clinical symptoms and laboratory findings combined with high mortality make early detection by imaging study very crucial.
The various appearances of PHA on computed tomography (CT) images and magnetic resonance imaging (MRI) have been delineated in case reports and in a few small series [3, 16]. But its ultrasound (US) appearances, particularly on contrast-enhanced ultrasound (CEUS), have not been clearly described [19, 20]. In this manuscript, we reported a case of PHA which mimicked intrahepatic cholangiocarcinoma (ICC) on conventional US and CEUS. Findings on various imaging examinations were carefully evaluated and the associated literatures were also reviewed.
A case report
A 43-year-old male patient was referred to the university hospital for further investigation due to a space-occupying lesion (SOL) in the liver found in other hospitals. The SOL was firstly found with conventional US and was referred to contrast-enhanced magnetic resonance imaging (CEMRI) one year and eight months ago. At that time, the lesion was about 3.7 cm×3.1 cm on CEMRI and was diagnosed as atypical hemangioma. The patient had no symptoms and all the serum markers were negative thus the patient chose radiographic follow-up. One month ago, the patient presented with intermittent and slight pain in the right upper quadrant abdomen. CEMRI a week ago showed the SOL size significantly increased to 6.2 cm×3.3 cm and the lesion was suspicious of ICC on MRI. The patient had a history of three and a half-year exposure to vinyl chloride and denied any history of hepatitis, tuberculosis, or diabetes mellitus.
Laboratory examination showed only slightly higher γ-glutamyl transpeptidase (68.6U/L; normal range, 10–60 IU/L). Other laboratory data including HBsAg, aspartate aminotransferase (AST) and alanine aminotransferase (ALT) were all within normal range. Hematologic tests, including complete blood counts, blood coagulation tests, were all normal too. Tumor markers were negative as following: cancer antigen 125(CA125) (10.12 IU/L; normal range, <35 IU/L); cancer antigen 19-9(CA19-9) (6.41 IU/L; normal range, <27 IU/L); cancer antigen 153 (CA153) (14.26 IU/L; normal range, <25 IU/L); α-fetoprotein (AFP) (5.2 ng/mL; normal value, <20 ng/mL); carcinoembryonic antigen (CEA) (1.69 ng/mL; reference value, <5 ng/mL).
Afterwards, he accepted conventional US, CEUS, and contrast-enhanced computed tomography (CECT) examinations in our hospital. The imaging findings, as well as those at previous imaging studies, were reviewed as following.
Imaging findings
Conventional US and CEUS
Conventional US and CEUS were performed with a LOGIQ E9 scanner (GE Healthcare, Milwaukee, WI, USA) and a 1–5 MHz curvilinear abdominal transducer. Gray-scale US showed an inhomogeneous hypoechoic and ill-defined lesion measuring 6.2 cm×3.5 cm×5.5 cm in segment IV of the liver with a patch-like macrocalcification in the lesion which showed posterior acoustic shadowing. Color Doppler US demonstrated a few peripheral blood flow signals in the lesion. CEUS was then performed with injection of 1.5 ml US contrast agent (SonoVue, Bracco, Milan, Italy), which can allow the assessment of blood flow and distribution down to microcapillary level in real-time, followed by 5 ml of 0.9% sterile saline flush through the antecubital vein [7, 9]. SonoVue consists of phospholipid-stabilized shell microbubbles filled with sulfur hexafluoride gas [9]. In arterial phase, the lesion demonstrated peripheral irregular rim-like hypo-enhancement. The contrast arrival time in the lesion was slower than that in surrounding liver parenchyma. Remarkable non-enhancement with sparse dotted/lined enhancement was appeared in central area of lesions. In portal and late phases, the lesion showed remarkable hypo-enhancement, resulting in a sharp contrast in comparison with adjacent normal tissue. The initial diagnosis was suspicious of ICC with conventional US and CEUS.
CEMRI
The MR examinations were performed on Magnetom® Trio Tim 3.0 MRI (Siemens AG, Munich, Germany). The contrast medium was applied by means of a bolus injection of Gd-DTPA with a dose of 2 mmol/ kg and an injection rate of 2 ml/s. On MRI one year and eight months ago, the lesion was about 3.7 cm×3.1 cm and was heterogeneous hypo-intense on T1-weighted images whereas heterogeneous hyper-intense on T2-weighted images, with a poorly defined boundary. The adjacent liver capsule appeared a little retraction. A short T2 signal about 1.0 cm was seen in the lesion center. Diffusion weighted imaging (DWI) demonstrated a remarkable high signal. On dynamic CEMRI, lesion appeared nodular and patchy peripheral enhancement, and progressive centripetal enhancement was observed. On delayed phase, the lesion’s signal was lower than that of the surrounding hepatic parenchyma. The lesion was diagnosed as atypical hemangioma at that time. On MRI a week ago, the lesion increased to 6.2 cm×3.3 cm, with a poorly defined boundary. On dynamic CEMR, the lesion showed more obvious intensity of enhancement in comparison with the previous MRI results. The lesion was suspicious of ICC (Fig. 1).
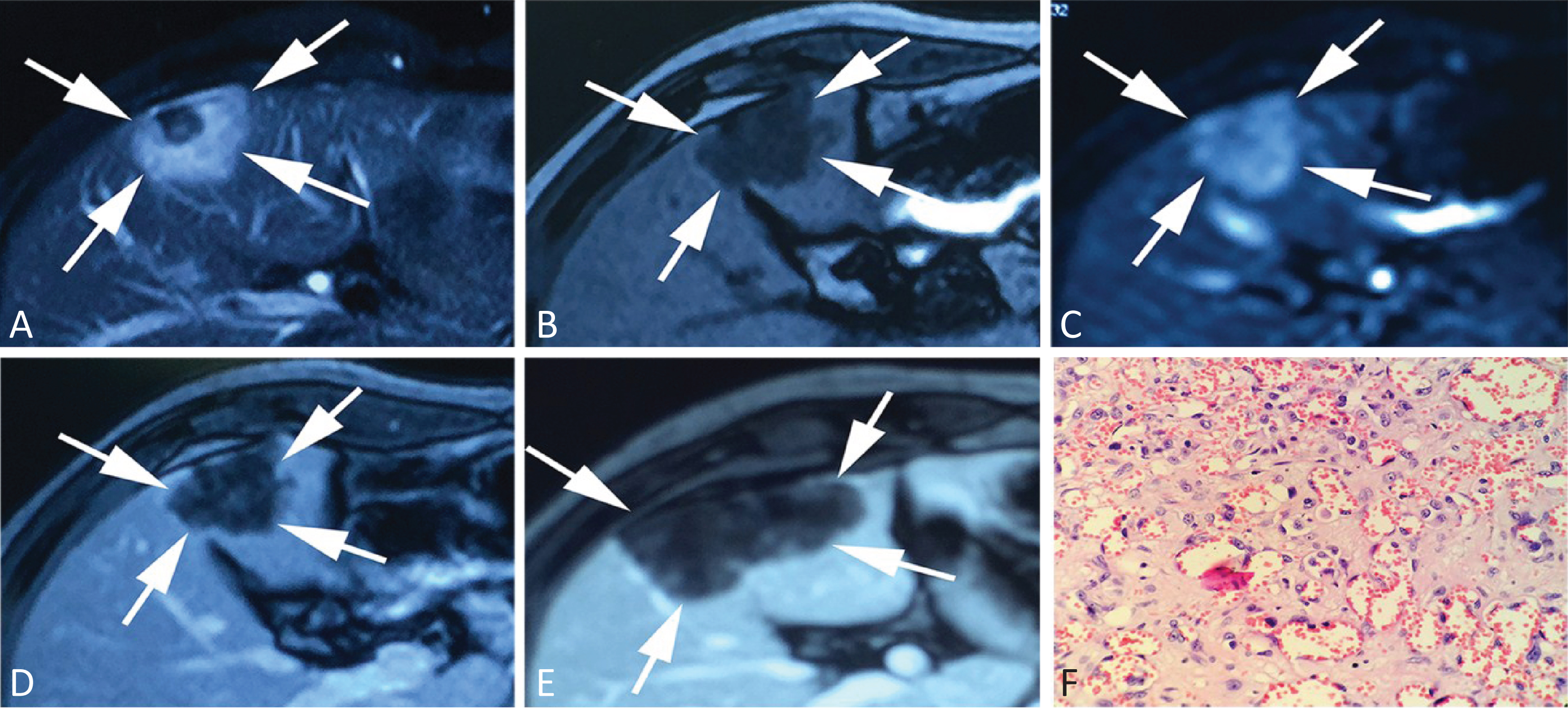
(A) T2-weighted image: Heterogeneous hyper-intense the lesion (white arrow) on T2-weighted image and lesion’s center saw a focal about 1.0 cm in diameter short T2 signal. (B) T1-weighted image: The lesion (white arrow) was heterogeneous hypo-intense on T1-weighted image. (C) Diffusion Weighted Imaging (DWI): the lesion (white arrow) demonstrated a remarkable high signal. (D) Dynamic CEMRI: lesion (white arrow) appeared nodular and patchy peripheral enhancement, and progressive centripetal enhancement was observed. (E) The latest Dynamic CEMR: the lesion (white arrow) showed more obvious intensity of enhancement in comparison with the previous MRI results. (F) Light microscopic examination for gross specimens: (original magnification, ×400; HE staining) reveals plenty of spindle-shaped neoplastic cells, which demonstrated vascular formation.
The CT examinations were performed on a 64-slice CT scanner (Aquilion 64, Toshiba, Otawara, Japan). The contrast medium was injected using iopromide with a dose of 1.5 ml/kg and an injection rate of 3.5 ml/s. On unenhanced CT, a 6.5 cm×2.3 cm×4.0 cm, slightly lower density of SOL was found in liver segment IV and segment V, with a poorly defined boundary. The CT value was about 30 HU. Nodular calcification about 1 cm in diameter was seen in the anterior portion of the lesion. On CECT, the lesion behaved as mild enhancement with a poorly defined boundary. The lesion was suspicious of malignancy (Fig. 2).
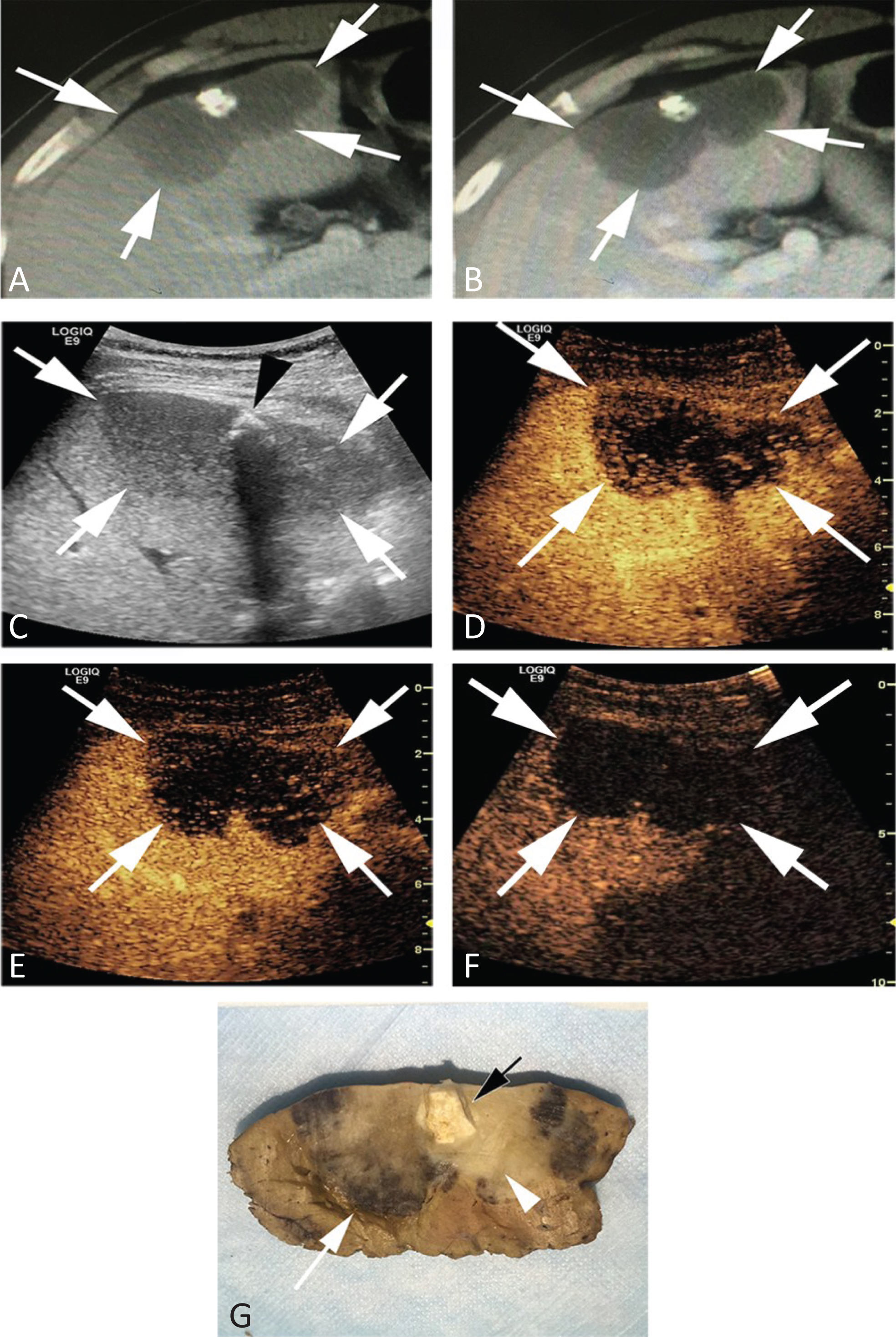
(A) Unenhanced CT: a 6.5 cm × 2.3 cm × 4.0 cm, slightly lower density of SOL(white arrow) was found in liver segment IV and segment V, with a poorly defined boundary. Nodular calcification about 1 cm in diameter was seen in the anterior portion of the lesion. (B) Dynamic CECT: the lesion (white arrow) behaved as mild enhancement with a poorly defined boundary. (C) Gray-scale US showed an inhomogeneous hypoechoic and ill-defined lesion (white arrow) measuring 6.2 cm × 3.5 cm × 5.5 cm in segment IV of the liver with a patch-like macrocalcification (arrow-head) in the lesion which showed posterior acoustic shadowing. (D) Arterial phase (24 sec) on CEUS: the lesion (white arrow) appears as ill-defined, peripheral irregular hypo-enhancement in comparison with adjacent liver tissue. (E) Portal phase (75 sec) on CEUS: the lesion (white arrow) appears as an area of slight hypo-enhancement decreasing gradually. (F) Late venous phase (341 sec) on CEUS: Microbubbles wash out from the lesion and the lesion appears hypo-enhancement. (G) Pathological gross liver resection specimen: There were periphery hemorrhage of lesion (white arrow), exactly where CEUS contrast agent started to diffuse into the tumor. Fibrotic focus (hyalinization), which is whitish in color, is notable in the central area of the lesion (arrow-head), exactly where non-enhancement was present on CEUS, and calcification measured 1.5 cm inside(black arrow).
The patient was subject to partial hepatectomy and the surgery was uneventful. On gross pathology, a greyish white lesion measured 6 cm×3.5 cm×3 cm was seen in a liver specimen of 9 cm×6 cm×4 cm. The mass abutted on the liver surface. The lesion showed a gray-red margin, with a poorly defined boundary and hard texture. There were fibrosis and hyalinization in the central, and calcification measured 1.5 cm inside. In addition, tumor embolus in vessels of gallbladder’s section was seen. A greyish white lymph node measured 1.5 cm was seen beside the gallbladder neck and was proved to be a metastatic lymph node.
Microscopically, tumor was characterized by the spindle-shaped cells, which demonstrated vascular formation. Degree of cellular differentiation quite varied, and some showed an epithelioid appearance. These vascular structures lined with neoplastic cells displayed a wide spectrum of patterns, ranging from dilated sinusoidal spaces to slit-like, freely anastomosing vascular channels.
Immunohistochemical studies showed that the neoplastic cells were positive for CD34, CD31, Factor VIII Ag, VEGF, P53, whereas the cells were negative for S-100, Keratin AE1-AE3, Keratin CAM 5.2, CK7, CK8/18, CK19, CK20, VILLIN, HEPA-1, CGA, SYN, SMA. Ki-67 was positive in up to 15% of the cells. The immunohistochemical findings supported vascular differentiation with high-grade morphology, and epithelioid morphology characteristic of an epithelioid angiosarcoma.
Discussion
PHA is a rare and rapidly progressing tumor liver in clinical practice. It usually affects the elderly but is also known to occur in younger patients [8]. And it commonly is more frequent in males than in females (ratio 3 : 1) [2]. PHA’s association with environmental carcinogens is exposure to vinyl chloride monomer, thorium dioxide, inorganic copper, arsenic and anabolic steroids, but in more than 70% of patients, the pathogenesis is unknown [16]. Takashi et al. [16] found that hematologic abnormalities, including hemolytic anemia, disseminated intravascular coagulation, and thrombocytopenia, were more frequently associated with PHA. About 15–27% of PHA patients present spontaneous tumor rupture, which is a potentially fatal complication [5, 27]. The most common site of metastases is the lung, followed by the spleen5. In this study, the patient had a history of three and a half-year’s exposure to vinyl chloride. He had a long natural history of PHA closing to two years. Jessica et al. [6] reported a PHA case with five years’ follow-up. The long natural history may represent the possibility of malignant transformation of a lower grade vascular neoplasm, such as hepatic epithelioid hemangioendothelioma to an angiosarcoma.
However, for the majority of clinicians or radiologists, their experience for this entity is limited. The initial clinical symptoms are usually unspecific. There appear no specific tumor markers for sarcoma in the serum. Additionally, many reports have described cases of PHA mimicked benign hemangioma [13, 25]. Because of these issues, an early diagnosis is extremely difficult, causing a dismal prognosis. As a result of a high recurrence rate and poor surgical outcomes, liver transplantation, as a form of therapy for PHA, is no longer performed [4]. And traditional radiotherapy and chemotherapy also fail to reach a conclusive benefit on survival of PHA. No formal guidelines are presented for the treatment of PHA at present [5]. Currently, the best treatment option for PHA is partial surgical resection of liver to remove the tumor. Early diagnosis and surgical resection with a curative intent provides patients the best chance of survival.
PHA showed a variety of findings on CECT and CEMRI images. Some PHAs are difficult to differentiate from cavernous hemangioma. The enhancement pattern of PHA on CT and MR images often demonstrates progressive peripheral enhancement toward the center of the tumor that is similar to that of cavernous hemangioma [13, 25]. In the present case, the enhancement pattern observed was similar on CEMRI. This patient was initially diagnosed as atypical hemangioma.
Conventional US has been reported as a nonspecific imaging modality that small lesions often show isoechoic and clearly demarcated, while large lesions show hypoechoic and poorly demarcated. Moreover, all lesions were inhomogeneous [20]. In this case, the patient showed an inhomogeneous hypoechoic and ill-defined lesion, but appearing a patch-like macrocalcification in the lesion, which was atypical from common liver masses and mimicked ICC.
Using CEUS, it is possible to distinguish most benign and malignant liver lesions and to differentiate typical FLL types, by analyzing the feature of the arterial, the portal venous and the late phases [7, 23]. In the present case, features of CEUS were atypical from the common liver masses. The lesion manifested peripheral irregular arterial enhancement with various amount of central unenhanced area. Peripheral enhancement declined gradually in portal phase, and washed out entirely in late phase. There are little literatures on CEUS characteristics of PHA. In a recent study of Trojan et al. [19], 4 PHAs were evaluated on CEUS. In the arterial and portal phases, the tumors displayed nodular peripheral enhancement in three patients and diffuse chaotic enhancement in one patient. In late phase, the tumors were hypo-enhanced compared to surrounding liver parenchyma in all patients, while peripheral nodular enhancement was still detectable in three patients. Wang et al. [20] reported 3 cases of PHA were evaluated with CEUS. All the lesions were characterized by remarkable central non-enhancement and peripheral irregular enhancement in the arterial and portal phase, and complete wash-out in the late phase. Non-enhancement on contrast-enhanced imaging often indicates cell-poor regions, such as hemorrhage, necrosis or fibrosis. Non-enhancement in the central area of CEUS as the special structure of PHA, fibrotic tissues with tumor cells were revealed under microscopy that may be associated with the very low velocity of blood flow in the central zone of tumors.
The patient was initially misdiagnosed as ICC with CEUS. Xu et al. [23] found that some nodules showed inhomogeneous enhancement during the arterial phase. Irregular and rim-like hyper-enhancement was found at the periphery of the tumors, and hypo-enhancement was found in the center of the tumors. The contrast agent in the nodules washed out from portal to late phase so that nodules displayed hypo-enhancement during these phases. The CEUS enhancement pattern of this SOL somewhat assembled ICC. The ill-defined margin and macrocalcification in the lesion are also apt to result in a diagnosis of ICC [10, 24]. Besides ICC, Liver metastases should also be considered as differential diagnosis. On CEUS, the appearance of liver metastases in arterial phase depends on the extent of arterial perfusion. Hypo-vascular metastases, usually originating from lung, breast, colonic or pancreatic primaries, may manifest rim enhancement. The quick and complete hypo-enhancement, or wash-out in portal and late phases is the most common characteristic of liver metastases on CEUS [12]. In this patient, no malignancy history was documented thus the possibility of liver metastasis was excluded.
Imaging modalities such as US, CT, and MRI, are helpful for detecting and locating tumors, while definite diagnosis is hardly achievable for the rare PHA. Radiologically, PHA may show variable appearances, so that a definite diagnosis needs histopathologic examination. PHA at pathologic assessment is characterized by the appearance of remarkable hemorrhage, necrosis and fibrosis. Grossly, the tumor displays four types of growth patterns: multiple nodules, a large solitary mass, mixed patterns of a dominant mass with nodules, and, rarely, a diffusely infiltrating micro-nodular tumor [15]. Typically, PHA is a multifocal tumor, followed by a large solitary mass. Microscopically, PHA is characterized by the spindle-shaped cells that form vascular channels. These channels display a wide spectrum of patterns, ranging from dilated sinusoidal to slit-like, freely anastomosing vascular channels. Fibrosis and deposition of hemosiderin are often encountered in solid portions of the tumor. Immunohistochemical staining can be used to prove the histological findings that vascular tumors derive from endothelial cells. Endothelial markers such as factor-VIII-related antigen, vimentin, CD 31, and CD 34 are essential for diagnosis. And the Ki-67 proliferative index >10% also a useful clue for PHA [21].
As a result of lacking of sufficient knowledge of this tumor and low incidence in clinical practice, definitive diagnosis is hard to achieve. Imaging findings will offer a critical time window during which surgical resection can be performed, which will be able to prolong patient survival time. When a markedly enlarged size, progressive enhancement pattern or other abnormal signs on MRI, CEUS may be useful as a reliable diagnostic test, particularly in suspect of PHA. CEUS could well depict PHA with some common characteristics, which provide worthy clues in diagnosis of this rare disease. Particularly the patient presents a long history of exposure to chemicals, no history of hepatitis or cirrhosis, and serum tumor markers are negative. In addition, Hackl et al. [11] found that High Resolution Ultrasound including Molecular Ultrasound Imaging using the targeted Contrast Agent BR55 could improve detection of preclinical Colorectal Liver Metastases. For further study, it might be meaningful to concentrate on the research on the diagnostic accuracy of PHA with liver specific contrast agents.
Footnotes
Acknowledgments
The scientific guarantor of this publication is Hui-Xiong Xu. The authors of this manuscript declare no relationships with any companies whose products or services may be related to the subject matter of the article. This work was supported in part by Grant SHDC12014229 from Shanghai Hospital Development Center, Grants 14441900900 and 15411969000 from Science and Technology Commission of Shanghai Municipality, and Grants 81401417 and 81501475 from the National Natural Science Foundation of China. One of the authors has significant statistical expertise. Institutional Review Board approval was obtained. Written informed consent was obtained from all subjects (patients) in this study.