
Abstract
OBJECTIVE:
This study was performed to investigate the accuracy of conventional ultrasound (US), contrast-enhanced US (CEUS), and dynamic contrast-enhanced magnetic resonance imaging (DCE-MRI) in assessing the size of breast cancer.
METHODS:
In total, 49 breast cancer lesions of 48 patients were included in this study. The inclusion criteria were the performance of total mastectomy or breast-conserving surgery for treatment of breast cancer in our hospital from January 2017 to December 2020 with complete pathological results, as well as the performance of conventional US, CEUS, and DCE-MRI examinations with complete results. The exclusion criteria were non-mass breast cancer shown on conventional US or DCE-MRI, including that found on CEUS with no boundary with surrounding tissues and no confirmed tumor scope; a tumor too large to be completely displayed in the US section, thus affecting the measurement results; the presence of two nodules in the same breast that were too close to each other to be distinguished by any of the three imaging methods; and treatment with preoperative chemotherapy. Preoperative conventional US, CEUS, and DCE-MRI examinations were performed. The postoperative pathological results were taken as the gold standard. The lesion size was represented by its maximum diameter. The accuracy, overestimation, and underestimation rates of conventional US, CEUS, and DCE-MRI were compared.
RESULTS:
The maximum lesion diameter on US, CEUS, DCE-MRI and pathology were 1.62±0.63 cm (range, 0.6–3.5 cm), 2.05±0.75 cm (range, 1.0–4.0 cm), 1.99±0.74 cm (range, 0.7–4.2 cm) and 1.92±0.83 cm (range, 0.5–4.0 cm), respectively. The lesion size on US was significantly smaller than that of postoperative pathological tissue (P < 0.05). However, there was no significant difference between the CEUS or DCE-MRI results and the pathological results. The underestimation rate of conventional US (55.1%, 27/49) was significantly higher than that of CEUS (20.4%, 10/49) and DCE-MRI (24.5%, 12/49) (P < 0.001 and P = 0.002, respectively). There was no significant difference in the accuracy of CEUS (36.7%, 18/49) and DCE-MRI (34.7%, 17/49) compared with conventional US (26.5%, 13/49); however, the accuracy of both groups tended to be higher than that of conventional US. The overestimation rate of CEUS (42.9%, 21/49) and DCE-MRI (40.8%, 20/49) was significantly higher than that of conventional US (18.4%, 9/49) (P = 0.001 and P = 0.015, respectively).
CONCLUSIONS:
CEUS and DCE-MRI show similar performance when evaluating the size of breast cancer. However, CEUS is more convenient, has a shorter operation time, and has fewer restrictions on its use. Notably, conventional US is more prone to underestimate the size of lesions, whereas CEUS and DCE-MRI are more prone to overestimate the size.
Keywords
Introduction
Accurately measuring the size of breast cancer lesions before surgery is not only an important factor in determining the operation method but also affects the patient’s prognosis. If the size of breast cancer lesions can be accurately measured, breast-conserving surgery can be considered for some patients with small breast cancer lesions. Surgeons can completely remove the breast cancer lesions while minimizing the loss of normal breast tissue and surrounding tissues. This will help to reduce the complications caused by an excessive resection range and improve the patient’s quality of life and cosmetic satisfaction.
The size of breast cancer tumors can be measured by palpation and imaging examinations such as mammography, ultrasound (US), and dynamic contrast-enhanced magnetic resonance imaging (DCE-MRI) [1–3]. DCE-MRI is reportedly the most accurate imaging method with which to assess the size of breast cancer. However, because of the risk of overestimation, the rate of mastectomy tends to increase with the use of DCE-MRI, and this does not improve the patients’ prognosis [3–9]. Conventional US is easy to perform and takes a short time. It is still the main method to assess the size of breast cancer. However, a disadvantage of US is that it underestimates the size of the tumor and increases the potential risk of incomplete tumor resection and positive margins, thereby increasing the chance of tumor recurrence [10–14].
Contrast-enhanced US (CEUS) is a pure blood pool imaging technique that provides richer diagnostic information than conventional US. It has a unique role in the perfusion and imaging of human microvessels and tissues; in particular, its ability to display tumor boundaries is better than that of conventional US. During the past few years, CEUS has been used to differentiate benign and malignant breast tumors, and many studies have shown that CEUS can optimize the BI-RADS classification, improve diagnostic efficiency, and reduce unnecessary biopsy [15–24]. However, few reports have described the accuracy of CEUS in evaluating the size of breast cancer. Determining whether CEUS is superior to conventional US and DCE-MRI requires further study.
Therefore, to provide a theoretical basis for surgeons to accurately evaluate the size of breast cancer lesions before surgery, we investigated the accuracy of tumor size assessment by conventional US, CEUS, and DCE-MRI in breast cancer compared with the pathological results.
Methods
Patients
This retrospective study was approved by the local institutional ethics committee (Code: 2021-P2-305-01), and the requirement for informed consent was waived. The inclusion criteria were the performance of total mastectomy or breast-conserving surgery for treatment of breast cancer in our hospital from January 2017 to December 2020 with complete pathological results, as well as the performance of conventional US, CEUS, and DCE-MRI examinations with complete results. The exclusion criteria were non-mass breast cancer shown on conventional US or DCE-MRI, including that found on CEUS with no boundary with surrounding tissues and no confirmed tumor scope; a tumor too large to be completely displayed in the US section, thus affecting the measurement results; the presence of two nodules in the same breast that were too close to each other to be distinguished by any of the three imaging methods; and treatment with preoperative chemotherapy.
We reviewed the data of 85 malignant breast nodules in patients who were treated in our hospital from January 2017 to December 2020 and met the inclusion criteria. We excluded 24 non-mass breast cancer nodules, 2 nodules that were too large for CEUS and could not be accurately measured by conventional US, 2 nodules that were close in proximity and could not be distinguished by DCE-MRI, and 8 nodules in patients who received preoperative chemotherapy. Finally, 49 nodules of 48 patients were included. All patients were women ranging in age from 31 to 83 years (mean age, 58.6±10.7 years). In order to ensure that the three imaging methods evaluate the same lesion, it must be ensured that the lesion is in the same quadrant of the ipsilateral breast, and the relative positional changes caused by different body positions during ultrasound and DCE-MRI should be fully considered, and further confirmation by the anatomical level is required.
Observation indicators
The lesion size was represented by its maximum diameter, and the maximum diameter of the postoperative lesion tissue was the gold standard. The maximum diameter of the lesion estimated by conventional US, CEUS, and DCE-MRI was compared with the maximum diameter of the postoperative lesion tissue, and if the error range was within 2 mm (including 2 mm), the lesion size was accurately estimated. If the error range was >2 mm, the lesion size was overestimated or underestimated. In present study, the maximum lesion diameter on US, CEUS, DCE-MRI and pathology in this study were 1.62±0.63 cm (range, 0.6–3.5 cm), 2.05±0.75 cm (range, 1.0–4.0 cm), 1.99±0.74 cm (range, 0.7–4.2 cm) and 1.92±0.83 cm (range, 0.5–4.0 cm), respectively.
Imaging methods
Conventional US examination of the breast was performed using the Hitachi Arietta 70 (Hitachi Medical Corporation, Tokyo, Japan) before CEUS with an 18- to 5-MHz linear phased-array transducer (L64; Hitachi Medical Corporation). The tumor features and size on conventional US were recorded. CEUS imaging was performed with a lower-frequency (7–3 MHz linear phased-array transducer (L34; Hitachi Medical Corporation). Ultrasonic microbubbles were prepared by mixing 59 mg of sulfur hexafluoride powder (Bracco Imaging SpA, Naples, Italy) with 5 ml of sterile saline and vigorously shaking for at least 15 seconds. The patient was placed in the supine position, and the examination site was fully exposed. The probe was placed lightly on the lesion site, and the imaging mode was adjusted to better display the lesion. A 4.8-ml microbubble suspension was injected through the cubital vein mass followed by administration of a 5-ml physiological saline flush, and the images were stored. The contrast-enhanced images were analyzed by two experienced sonographers. The lesion size was measured using the image in which the boundary of the lesion was most clear.
DCE-MRI was performed using a GE Discovery 750W superconducting 3.0T MR instrument with an 8-channel special coil for the breast surface (GE Healthcare, Chicago, IL, USA). The patient was placed in the prone position with both mammary glands hanging naturally in the coil. Fat in plain scan was successively collected to inhibit T2-weighted imaging (T2WI), T1-weighted imaging (T1WI), diffusion-weighted imaging (DWI), axial dynamic enhanced T1WI, and delayed fat suppression T1WI in the sagittal position. The imaging parameters were as follows. Fat suppression on T2WI: TR, 4585 ms; TE, 85 ms; layer thickness, 5 mm; turn angle, 90°; matrix, 320×256; and field of view, 32×32 cm. DWI: TR, 2450 ms; TE, 68 ms; layer thickness, 5 mm; matrix, 128×160; field of view, 32×32 cm; and B = 0, 1000 s/mm2. Axial dynamic enhanced T1WI: The volume imaging sequence of mammary gland assessment was used. The first-phase mask was collected, and Gd-DTPA was then injected at 0.2 mmol/kg body mass with a flow rate of 3.0 mL/s using a double-cylinder high-pressure syringe, followed by injection of 10 mL of normal saline. The interval dynamic enhanced scan was performed immediately: TR, 4.9 ms; TE,1.9 ms; rotation angle, 10°; matrix, 288×192; field of view, 32×32 cm; layer thickness, 2 mm; total of eight phases; and scanning time of 55 seconds.
Pathologic analysis
All patients in this study underwent mastectomy or breast-conserving surgery. The specimen was sectioned every 5 mm, and the maximum size was measured by sampling the tissue from the largest section. The tumor size on the final pathologic report was considered as a standard reference. Histologic diagnoses were made by two pathologists with 10 and 13 years of experience in breast histological evaluation, respectively.
Statistical analysis
Continuous variables are expressed as mean±standard deviation, and categorical variables are presented as frequency and percentage. The maximum nodule sizes estimated with conventional US, CEUS, and DCE-MRI were compared with the pathological sizes using the paired t test. Bland-Altman plot was used to demonstrate the consistency between conventional US, CEUS, DCE-MRI, and pathological size. It also used to demonstrate the consistency of the two sonographers who evaluated the CEUS image. The correlation between the maximum diameter on conventional US, CEUS, and DCE-MRI and the maximum diameter of pathological tissue was evaluated by Pearson’s correlation analysis. The accuracy, overestimation, and underestimation rates of conventional US, CEUS, and DCE-MRI were compared by the chi-square test. All statistical analyses were performed using SPSS software version 17.0 (SPSS Inc., Chicago, IL, USA). A P value of <0.05. was considered statistically significant. When making pairwise comparisons, the Bonferroni correction test level was used (α= 0.017).
Results
Pathologic types
Among 49 malignant nodules, 34 (69.4%) were invasive ductal carcinoma, 9 (18.4%) were ductal carcinoma in situ, 1 (2.0%) was mucinous carcinoma, 1 (2.0%) was solid papillary carcinoma in situ, 1 (2.0%) was solid papillary carcinoma with invasion, 1 (2.0%) was invasive lobular carcinoma, 1 (2.0%) was enveloping papillary carcinoma, and 1 (2.0%) was medullary carcinoma (Table 1).
Pathological types of breast cancer
Pathological types of breast cancer
Bland-Altman plot all showed good agreement of the size between the two sonographers who evaluated the CEUS image, and between the three image methods and pathological results. The mean difference of the two sonographers was 0.07 cm and the 95% confidence interval (95% CI) was –0.26∼0.40 cm. Only two cases were not in the 95% CI (Fig. 1). The mean difference of conventional US and pathological results was –0.31 cm and the 95% CI was –1.47∼0.85 cm. Two cases were not in the 95% CI. The mean difference of CEUS and pathological results was 0.13 cm and the 95% CI was –0.97∼1.27 cm. Three cases were not in the 95% CI. The mean difference of DCE-MRI and pathological results was 0.07 cm and the 95% CI was –1.30∼1.44 cm. Two cases were not in the 95% CI (Fig. 2).

Bland-Altman plot of the lesion size between the two sonographers who evaluated the contrast-enhanced ultrasound image.
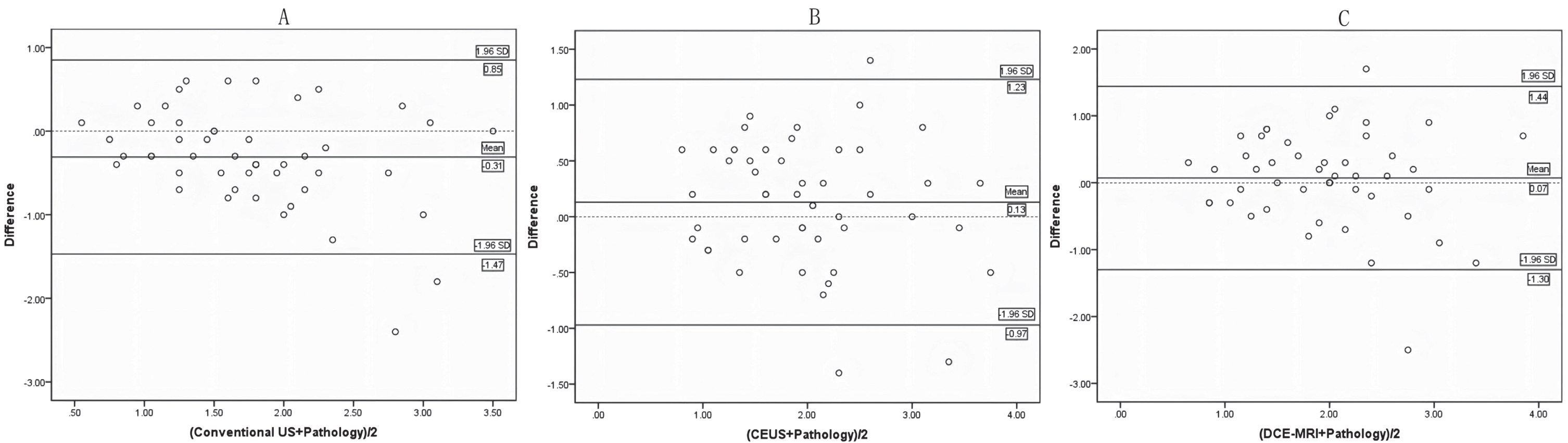
Bland-Altman plot of the lesion size between the three image methods and pathological results. CEUS = contrast-enhanced ultrasound; Conventional US = Conventional ultrasound; DCE-MRI = dynamic contrast-enhanced magnetic resonance imaging.
The maximum lesion diameter on CEUS had the best correlation with the maximum diameter of pathological tissue (correlation coefficient r = 0.756, P < 0.001). The correlation coefficient between the maximum diameter on conventional US and the maximum diameter of pathological tissue was 0.705 (P < 0.001). The correlation coefficient between the maximum diameter on DCE-MRI and the maximum diameter of pathological tissue was 0.605 (P < 0.001) (Fig. 3).

A showed the correlation between breast cancer size measured by CEUS and the postoperative pathological results, r = 0.756. B showed the correlation between breast cancer size measured by conventional US and the postoperative pathological results, r = 0.705. C showed the correlation between breast cancer size measured by DCE-MRI and the postoperative pathological results, r = 0.605. CEUS = contrast-enhanced ultrasound; Conventional US = Conventional ultrasound; DCE-MRI = dynamic contrast-enhanced magnetic resonance imaging.
The maximum lesion diameter on US, CEUS, DCE-MRI and pathology were 1.62±0.63 cm (range, 0.6–3.5 cm), 2.05±0.75 cm (range, 1.0–4.0 cm), 1.99±0.74 cm (range, 0.7–4.2 cm) and 1.92±0.83 cm (range, 0.5–4.0 cm), respectively. The lesion size on US was significantly smaller than that of postoperative pathological tissue (P < 0.05). There was no statistically significant difference between the lesion size on CEUS and DCE-MRI and the lesion size of postoperative pathological tissue (P > 0.05) (Table 2).
Breast cancer size measured by conventional US, CEUS and DCE-MRI compared to pathological results
Breast cancer size measured by conventional US, CEUS and DCE-MRI compared to pathological results
The lesion size was represented by the maximum diameter. Conventional US = Conventional ultrasound; CEUS = contrast-enhanced ultrasound; DCE-MRI = dynamic contrast-enhanced magnetic resonance imaging; a = P value compared with conventional US and pathology results; b = P value compared with CEUS and pathology results; c = P value compared with DCE-MRI and pathology results.
The underestimation rate of conventional US was significantly higher than that of CEUS and DCE-MRI (P = 0.009, P = 0.015). The overestimation rate of conventional US was lower than that of CEUS and DCE-MRI (P < 0.001, P = 0.002). The accuracy of CEUS and DCE-MRI was consistent and higher than that of conventional US, but the difference was not statistically significant (Table 3, Fig. 4).
Comparison of the accuracy of conventional US, CEUS and DCE-MRI in measuring the size of breast cancer
Comparison of the accuracy of conventional US, CEUS and DCE-MRI in measuring the size of breast cancer
Conventional US = Conventional ultrasound; CEUS = contrast-enhanced ultrasound; DCE-MRI = dynamic contrast-enhanced magnetic resonance imaging; a = conventional US compared with CEUS, P = 0.009; b = conventional US compared with DCE-MRI, P = 0.015; c = conventional US compared with CEUS, P < 0.001; d = conventional US compared with DCE-MRI, P = 0.002.

A left breast mass of a 73-year-old female patient, which was pathologically encapsulated papillary carcinoma. Figures A, B and C were conventional US, CEUS and DCE-MRI imaging respectively. The maximum diameter of the mass measured by three imaging methods was 1.3 cm, 1.9 cm and 2.0 cm, respectively. The maximum diameter of the postoperative pathology was 2.0 cm. CEUS and DCE-MRI were accurate, and conventional US underestimated the maximum diameter of the mass.Conventional US = Conventional ultrasound; CEUS = contrast-enhanced ultrasound; DCE-MRI = dynamic contrast-enhanced magnetic resonance imaging.
The size of a breast cancer lesion determines the T stage in the TNM staging system, which is the basis of breast cancer staging. Tumor size has an important influence on the surgical method and the cosmetic effect after breast-conserving surgery [25]. In addition, breast cancer size is a risk factor for postoperative ipsilateral breast recurrence and distant metastasis [26, 27]. For every 1-mm underestimation, the odds ratio of incomplete tumor resection will increase by 1.4 [28]. Accurate knowledge of tumor size can help the surgeon to preserve more healthy tissue after removing the tumor completely.
High-frequency US has the advantages of convenience and lack of radioactivity, and it is an important imaging method for breast examination. However, some studies have shown that the breast cancer size measured by US is underestimated, which increases the risk of postoperative tumor residue [10–13]. Farrokh et al. [10] defined accurate measurement as absolute consistency between the US measurement value and the pathological tissue size. In their study, that 65.7% of breast cancer lesions were underestimated. van Esser et al. [13] applied CEUS to evaluate the accuracy of the preoperative tumor size in patients with invasive ductal carcinoma, and the measurement accuracy was defined as error of within 2 mm. The results showed that conventional US underestimated the tumor size in 67% of cases, and the accuracy was only 22%. Among the three imaging methods used in this study, the greatest difference in the maximum diameter was found between conventional US and the pathological results. A maximum value of >2 mm smaller than the pathological result was defined as an underestimation. The results showed that the accuracy was 26.5%, and US underestimated the tumor size in 55.1% of cases. This is consistent with the results of previous studies. The reasons for underestimation on US may be as follows. First, US usually only measures the low-echo part of the tumor, excluding the surrounding high-echo halo. Joekel et al. [29] showed that the size of the pathological tissue was more accurate when the high-echo halo was included in the measurement than when the high-echo halo was not included. Second, conventional US is affected by the homogeneity of the breast background and other factors, and the identification of tumor boundaries is not accurate [30]. Third, under the influence of the tumor itself, the tumor size is more likely to be underestimated in tumors of >20 mm [31]. In addition, the pathological type of tumor may be a potential factor.
DCE-MRI as an imaging method for evaluating breast tumors is reportedly superior to mammography, US, and clinical examination in the evaluation of breast tumor size [32]. A paramagnetic contrast agent in DCE-MRI is used to examine the distribution of blood vessels and new blood vessels in tumors [33, 34]. DCE-MRI has unique advantages when applied to multiple lesions, large lesions, and simultaneous display of the contralateral mammary glands. However, it also has limitations, such as high cost, contraindications for the use of contrast agents (renal toxicity, allergic reaction), and inapplicability for patients with a cardiac pacemaker or metal in other parts of the body [35].
The US contrast agent used in this study is composed of sulfur hexafluoride microbubbles; thus, it is highly reflective and does not extravasate from the vascular lumen. It is a pure blood pool contrast agent and can effectively reveal the blood vessel diameter at the capillary level. Compared with DCE-MRI, CEUS has the advantage of no renal toxicity, very low incidence of severe allergic reactions, low cost, convinient, and can be used in patients with cardiac pacemaker and metal in other parts of the body and claustrophobic patients. Studies have shown that this technique can reliably display neovascularization in and around tumors and may be used to identify tumor boundaries and pathological features [36, 37]. Lee et al. [38] performed CEUS and DCE-MRI examinations on 30 patients with breast cancer undergoing neoadjuvant chemotherapy before surgery and then performed a comparative analysis with the maximum diameter of postoperative pathological tissue. The results showed that the correlation coefficient between CEUS and the pathological results was 0.75 and that the correlation coefficient between DCE-MRI and the pathological results was 0.42. CEUS was more closely correlated with the pathological results. This is consistent with the results of the present study, which showed that CEUS had the best correlation with the maximum diameter of the actual pathological tissue (r = 0.756), followed by conventional US (r = 0.705) and DCE-MRI (r = 0.605). Otherwise, Bland-Altman plot demonstrated good agreement when evaluated lesion size between the three imaging methods (conventional US, CEUS, DCE-MRI) and pathological results. Only 2 or 3 cases of total 49 were not in the 95% CI. For the two sonographers who evaluated CEUS imaging, the consistency was excellent with the mean difference of 0.07 cm and 95% CI of –0.26∼0.40 cm.
Relevant studies have shown that CEUS is superior to conventional US in identifying the size of malignant breast lesions [13, 39]. Although there was no significant difference between CEUS and conventional US in identifying breast cancer in this study, CEUS accuracy was nearly consistent with DCE-MRI accuracy (36.7%), and both were superior to conventional US (26.5%). The underestimation rate of CEUS was 20.4% and that of DCE-MRI was 24.5%, and both were significantly lower than that of conventional US (55.1%). In addition, the difference between the three measurement methods and the actual maximum diameter of pathological tissue was largest for conventional US, while the difference between CEUS and DCE-MRI and the maximum diameter of the pathological results was not statistically significant. The results of this study showed that CEUS and DCE-MRI had almost the same accuracy in estimating the size of malignant breast lesions. However, both CEUS and DCE-MRI showed high overestimation rates of 42.9% and 40.8%, respectively. Several studies have shown that DCE-MRI often overestimates the size of lesions, with some indicating an overestimation rate as high as 70% [6–9]. Previous studies have also shown that normal breast tissue shows high enhancement on DCE-MRI; this may conceal malignant lesions or cause difficult identification of malignant lesion boundaries, resulting in inaccurate tumor size measurement [40–44]. CEUS may overestimate the size of the tumor for the following two reasons. First, CEUS is a blood pool imaging agent, and tumor cells may not be involved in the location of abnormal blood flow imaging. Second, the measurement range is too large because of the overflow of contrast agent.
Computed tomography (CT) and positron emission tomography (PET) data were not included in this study. Generally, computed tomography (CT) is not used to evaluate breast lesions because it delivers high radiation dose to the breast, and breast tissue is often confused as breast masses on CT scan. But CT may occasionally find some breast lesions or lumps in other areas associated with breast cancer [45, 46]. Positron emission tomography/computed tomography (PET/CT) was not a routine recommendation for breast examination, but it was helpful in evaluating breast cancer axillary lymph node metastasis, distant metastasis and recurrence [47–49]. There were few reports on the measurement of breast cancer size by PET/CT. Park SH et al. reported a peri-tumoral halo uptake layer method (PHL) of the 18F-FDG PET/CT scan to measure breast cancer size. They suggested that this method showed more accurate than MRI [50]. Further, Wu Y et al. reported that the 18F-FDG PET/CT-based PHL method was superior to breast ultrasound and MRI, and that it provided sufficient reliability and high accuracy for measuring tumor size in patients with breast cancer [51]. The above opinion needs to be further confirmed, and concerns about radioactivity limit the widespread application of PET technology in breast diseases.
This study had several limitations. First, it was a retrospective study at a single institution, inevitably resulting in selection bias. Second, the sample size was not sufficient to evaluate differences between histologic types. Among the 49 lesions, 34 (69.4%) were invasive ductal carcinoma, 9 (18.4%) were ductal carcinoma in situ, and 6 were other malignant histologic types. We were also unable to further analyze the differences in tumor sizes because of the limited sample size. Finally, although the size of pathological tumors is the gold standard, tumors may be deformed or shrink when surgical specimens are removed and fixed.
In conclusion, CEUS and DCE-MRI show similar performance when evaluating the size of breast cancer, and both tend to be slightly better than conventional US in terms of accuracy. However, CEUS is more convenient, has a shorter operation time, and has fewer restrictions on use. Notably, conventional US is more prone to underestimate the size of lesions, whereas CEUS and DCE-MRI are more prone to overestimate the size.
Data availability statement
The raw data required to reproduce these findings cannot be shared at this time as the data also forms part of an ongoing study.
Conflicts of interest
None of the authors have any financial or scientific conflicts of interest with regard to the research described in this manuscript.
Funding statement
Beijing Municipal Administration of Hospital’s Ascent Plan, Code: DFL20180102.