
Abstract
BACKGROUND:
Contrast-enhanced ultrasound (CEUS) has been used as an additional imaging technique to conventional ultrasound in order to clarify gallbladder findings, CEUS is easy and fast to perform, overcomes the limitations of gray-scale ultrasonography and is a safe tool.
OBJECTIVE:
The aim of this retrospective mono-center analysis study is to evaluate the diagnostic performance of CEUS in the assessment of gallbladder disease by comparing its results with additional CT findings.
METHODS:
A total of 24 patients between 2009 and 2017 with unclear gallbladder appearance were retrospectively analysed. The contrast agent administered was a second-generation blood pool agent (SonoVue®, Bracco, Milan, Italy). Examinations were performed and interpreted by a single experienced radiologist with more than fifteen years’ experience.
RESULTS:
24 patients were successfully examined without any adverse reaction. CEUS presented a sensitivity of 75%, a specificity of 100.0%, a positive predictive value of 100.0% and a negative predictive value of 95%.
CONCLUSIONS:
In conclusion, the excellent results in this study acknowledged that CEUS is a feasible alternative tool to differentiate gallbladder pathologic alterations.
Introduction
Contrast-enhanced ultrasound (CEUS) of the gallbladder is recently being used as an additional imaging technique to conventional ultrasound (US) in order to elucidate B-mode US findings. CEUS is easy to perform and overcomes the limitations of gray-scale ultrasonography and color Doppler imaging [1]. When compared to contrast enhanced computed tomography (CE-CT), CEUS has some crucial advantages: It is an imaging method without the use of radiation, the contrast agent administered can be safely used in patients with renal function impairment and thyroid dysfunction because it has no renal, thyroid or cardiac toxicity [2–4]. Moreover, the occurrence of an allergic reaction has been described in the literature as 1 of 10.000 cases [5, 6].
The US contrast media enables vessel flow identification as small as 40μm [7] being able to display an enhancement pattern of the gallbladder in 2 vascular phases: arterial (10–20 seconds postinjection) and late parenchymal (31–180 seconds), different than the CEUS pattern of liver lesions [8–11].
The CEUS of the gallbladder is normally used to identify normal variants, differentiate sludge from neoplastic lesions, detect benign and malignant pathology as well as to demonstrate infection, wall rupture and hemobilia. Furthermore, it can also be used to show the biliary tree distinguishing benign and malignant tumours, metastases and cholangiocarcinoma. Although CEUS has been recently used as an additional imaging technique for gallbladder disease, its role has still not been compared to the CT imaging findings.
The aim of this retrospective mono-center analysis study is to evaluate the diagnostic performance of CEUS in the assessment of gallbladder disease by comparing its results with additional CT findings.
Materials and methods
This retrospective study received approval from the local institutional ethical committee of the institutional review board and authors followed the ethical guidelines for publication in Clinical Hemorheology and Microcirculation [5]. Oral and written informed consent of all patients was obtained after CEUS and CT examination have been carefully explained. All study data were collected in compliance with the principles expressed in the Declaration of Helsinki 2002.
A total of 24 patients between 2009 and 2017 with unclear gallbladder appearance who received CEUS and CT imaging were retrospectively analysed with a mean time between both examinations of 8 weeks. The mean age at the time of CEUS examination was 57 years (Min. 25; Max 89; SD±17.2 years).
All examinations were included due to their high-quality image.
Imaging series of CE-CT studies were based on standard scanning protocols with scanners used at the time of the examination (Siemens SOMATOM Force, Siemens SOMATOM Definition Flash, Siemens SOMATOM Definition AS).
CEUS examinations were completed with high-end ultrasound systems with up-to-date CEUS specific protocols available at the time of the examination (Siemens Acuson Sequoia and Siemens S2000, EPIQ 7, Philips Ultrasound). All the used transducers were required to be for abdominal use with a frequency ranged from 1.0 to 9.0 MHz, Siemens ultrasound system was used with C4-1 and C6-1 HD probes and Philips ultrasound system was used with the C9-2 probe. Each ultrasound system was configured with a low mechanical index (always <0.2), in order to avoid early microbubble-destruction.
All patients underwent fasting at least 6 h prior examination. Before CEUS, each patient underwent a baseline US examination of the gallbladder and the adjacent liver. In all evaluated patients, a second-generation blood pool agent (SonoVue®, Bracco, Milan, Italy) composed of phospholipid-stabilized shell microbubbles filled with sulfur hexafluoride gas was applied. In each patient, a dose of 1.5 to 2.4 mL SonoVue was administered as a bolus injection by using a 20–22-gauge cannula via antecubital vein, followed by a flush-injection of 5 to 10 ml of 0.9% NaCl.
After the application of contrast agent, cine loops of the examination acquired were archived in the picture archiving and communication system of our institution. Mean examination time ranged between 3–5 minutes.
Baseline B-mode US, color Doppler, power Doppler and CEUS were performed and interpreted by a single experienced radiologist with more than fifteen years’ experience in US and experience with CEUS since 2003.
The obtained CEUS results and matched CT examinations from each patient were retrospectively analysed for diagnostic accuracy by testing sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV).
Out of the 24 patients, CT imaging showed suspicious gallbladder appearance in 3 patients, 2 of them were also depicted using CEUS technique. In 10 patients CEUS demonstrated an inflammation of the gallbladder which was confirmed in CT. In one patient, CEUS displayed an adenomyomatosis pattern which was clarified and confirmed in additional imaging.
Results
All 24 patients were successfully examined by CEUS and CT, without any adverse reaction.
Mostly, one dose of 1.5 to 2.4 ml of contrast agent (SonoVue®) was used for each CEUS examination. If necessary, contrast media was repeatedly injected up to three times.
Although CEUS has been only an additional imaging tool for gallbladder findings, when matched to the CT technique, CEUS presented a sensitivity of 75%, a specificity of 100.0%, a positive predictive value (PPV) of 100.0% and a negative predictive value (NPV) of 95%.
Out of the 24 patients, two patients displayed a malignant appearance of the gallbladder in CEUS, which were also revealed in CT and pathologic verified as adenocarcinoma. Only one case reported a gallbladder malignancy in CT which was not depicted in CEUS. Moreover, CEUS displayed features of cholecystitis in 10 patients which were all reported in CT. In addition, CEUS revealed a malignant gallbladder pattern in one case, which was reported on CT as an infiltration of a malignant liver tumour.
Discussion
The introduction of real-time CEUS imaging in organs such as liver [8, 10], kidney [12, 13] pancreas [14] and blunt abdominal trauma [7] has led to a major breakthrough in diagnostic imaging, especially when compare to the conventional ultrasound. Although CEUS is a standard method for suspicious liver masses, its use for the gallbladder is unclear and still not widely broaden in the literature. Moreover, according to some publications, its role in gallbladder diseases has been controversial during the last years. However, it has become increasingly recognized during recent years [15–17].
The established diagnostic first line imaging of the gallbladder has mainly been assessed by the conventional ultrasound. Although, B-mode ultrasound imaging has an excellent spatial and temporal resolution and the ability of real-time imaging, its applicability is sometimes insufficient.
Normally, a gallbladder tumour is demonstrated in B-mode imaging as either a focal gallbladder polyp or a solid mass. Unfortunately, motionless biliary sludge can display US images evenly. Moreover, native ultrasonography is also limited in the differentiation between carcinoma and chronic cholecystitis with a thickened wall and has some difficulties in demonstrating some features such as destruction of the gallbladder wall beneath the lesion or infiltration to the adjacent liver tissue suggesting malignancy [18]. The additional power Doppler and color Doppler technique in conventional ultrasonography are insensitive to deeply located vessels as well as to depict slow flow.
As the additional contrast agent applied is able to show enhancement and perfusion of the target lesion in different phases, CEUS overcomes the limitations of conventional US, color or power Doppler. Therefore, the administration of contrast media increases the diagnostic confidence.
This retrospective study analysed the diagnostic performance of CEUS in gallbladder diseases and compared its results to the additional CT examinations.
In this study, the greyscale US demonstrated a mass and a thickened gallbladder wall. After contrast media administration, the mass displayed an irregular, tortuous arterial enhancement suspicious of carcinoma, also showed in other studies [19–21]. It is important to emphasize that the arterial enhancement of a mass followed by its early washout are not specific criteria to characterize a lesion as malignant. There are other important additional features for malignancy of a mass such as the presence of a disrupted wall, its tortuous-type vascularity and patient age that have to be considered [18].
In one patient CEUS displayed an adenomyomatosis pattern which was also confirmed in CT. Adenomyomatosis of the gallbladder is a focal, segmental, or diffuse benign hyperplasia of the gallbladder wall. It is relatively common and often an incidental finding. In the arterial phase, CEUS showed a “moth-eaten” enhancement pattern of the wall, simultaneously to the enhancement of the liver parenchyma. Sometimes the gallbladder wall enhances homogeneously and half of the wall might take a “hourglass” appearance [22, 23].
CEUS showed cholecystitis in 10 patients, all of them were confirmed in CT. Gray-scale US appearances of cholecystitis such as gallbladder wall thickening and edema are already known. On CEUS, the arterial phase displays homogeneous, fast, and intense enhancement of the thickened gallbladder wall. When untreated, this inflammation can lead to an abscess of the adjacent liver. The abscess wall shows an enhancement on CEUS whereas the internal content would not show any enhancement [24].
Finally, the sensitivity (75%), specificity (100.0%) and PPV (100.0%) calculated in this study demonstrated that CEUS is not only easy and fast to perform but also a feasible alternative to CE-CT imaging (Figs. 1–9). Moreover, it is a safe tool because CEUS examinations do not use radiation and the contrast agent applied has no renal, thyroid or cardiac toxicity [2, 25].
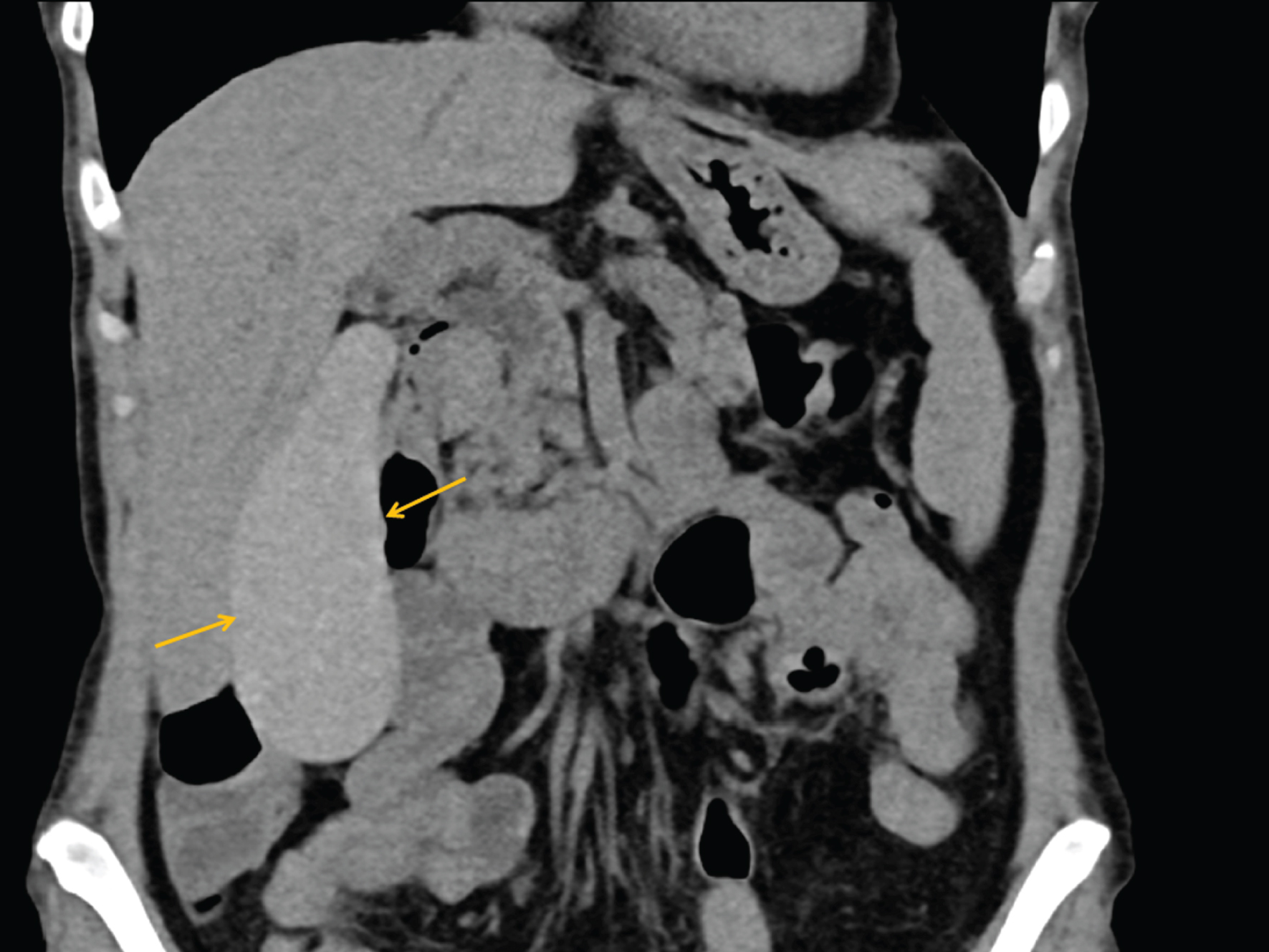
Coronal CT-image of a patient depicting a gallbladder showing hyperdense intraluminal material (yellow arrows).
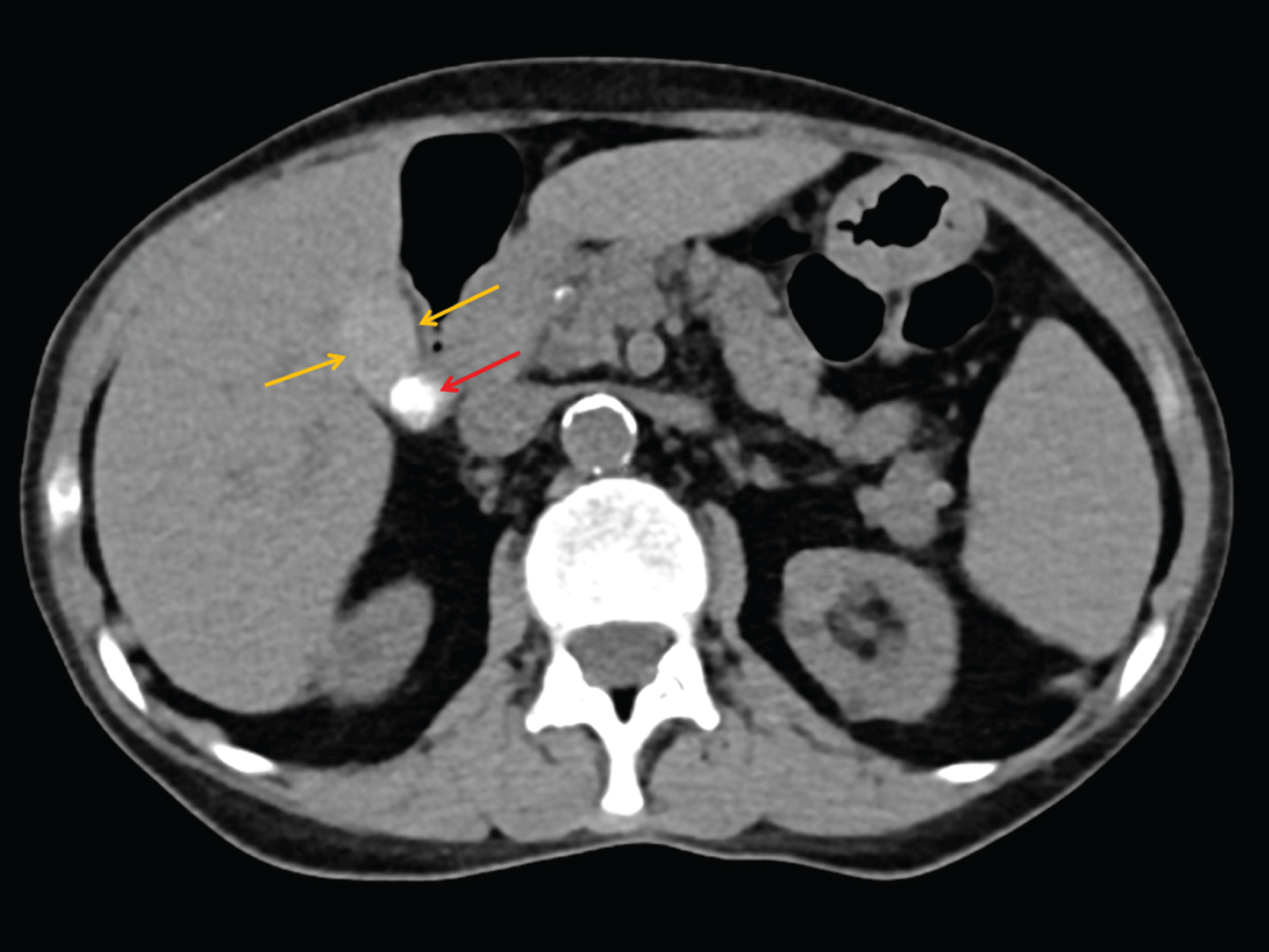
Same patient as in Fig. 1. Axial CT-imaging shows the gallbladder with hyperdense intraluminal fluid (yellow arrows) and a gallbladder stone (red arrow).
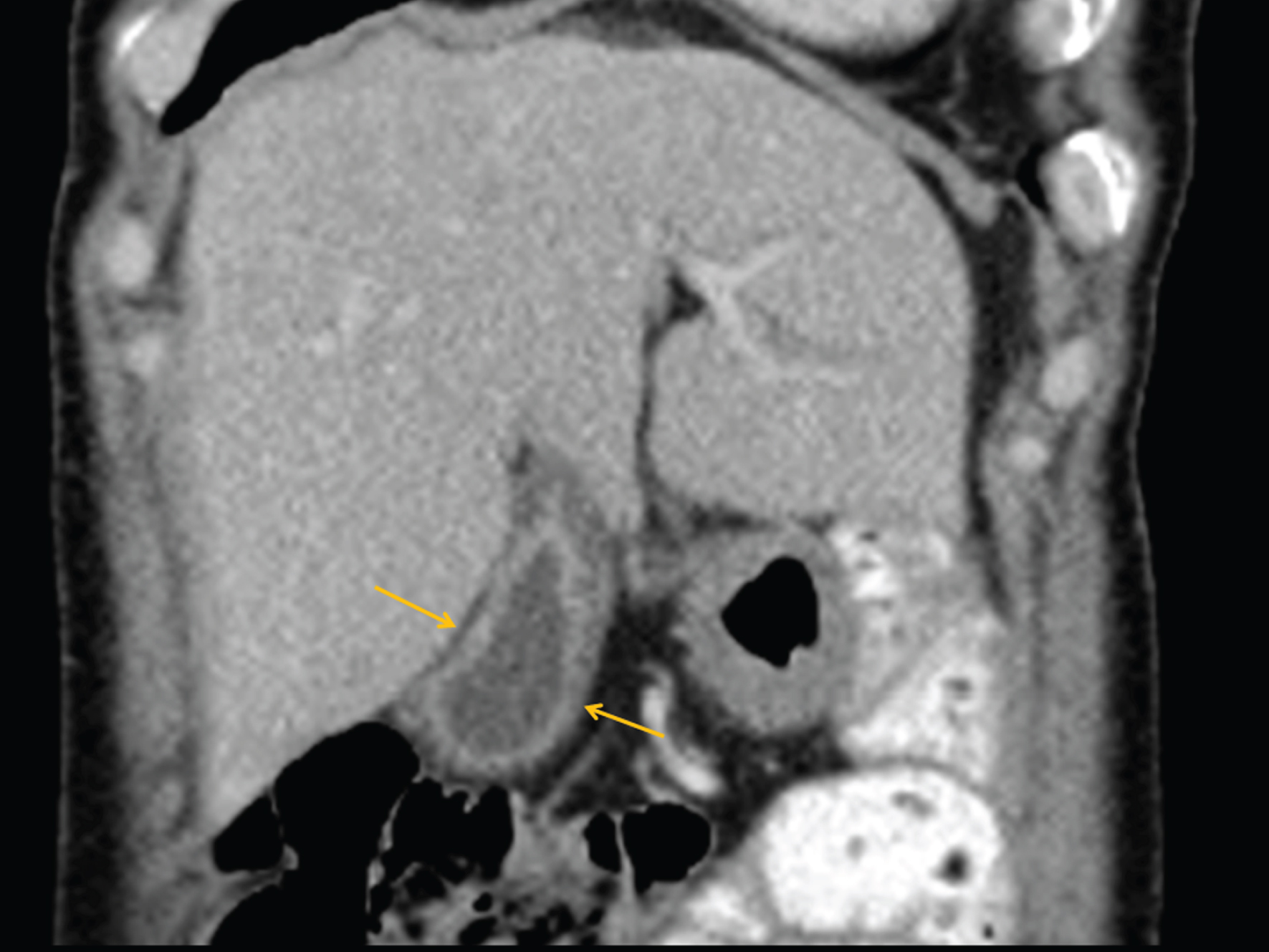
Coronal CT-image of a patient showing a thickened gall bladder wall suspicious of an adenomyomatosis of the gallbladder. The patient did not reveal any clinical palpable pain during examination.
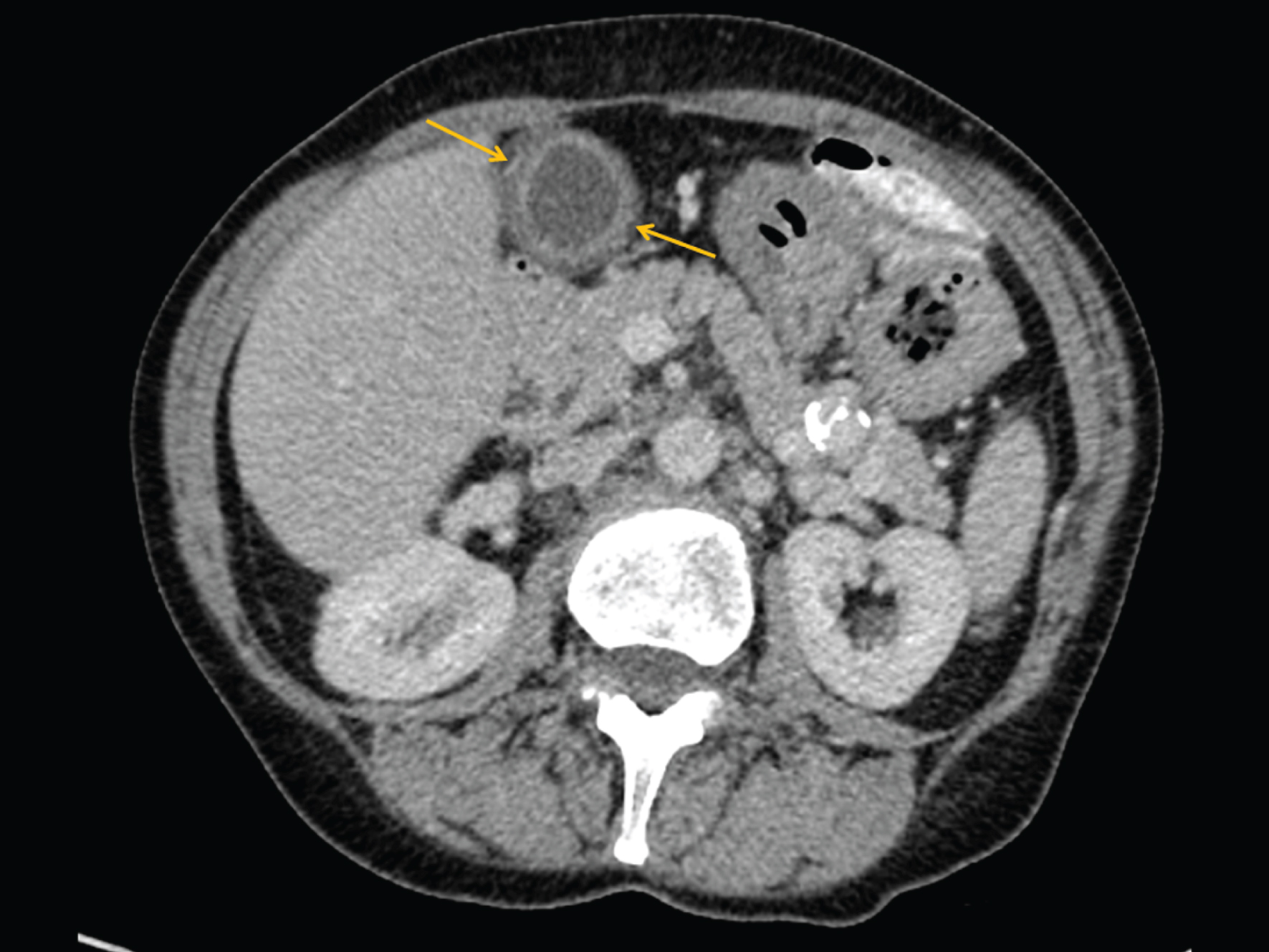
Same patient as in Fig. 6. The axial CT-image also shows the homogenously thickened wall of the gallbladder.
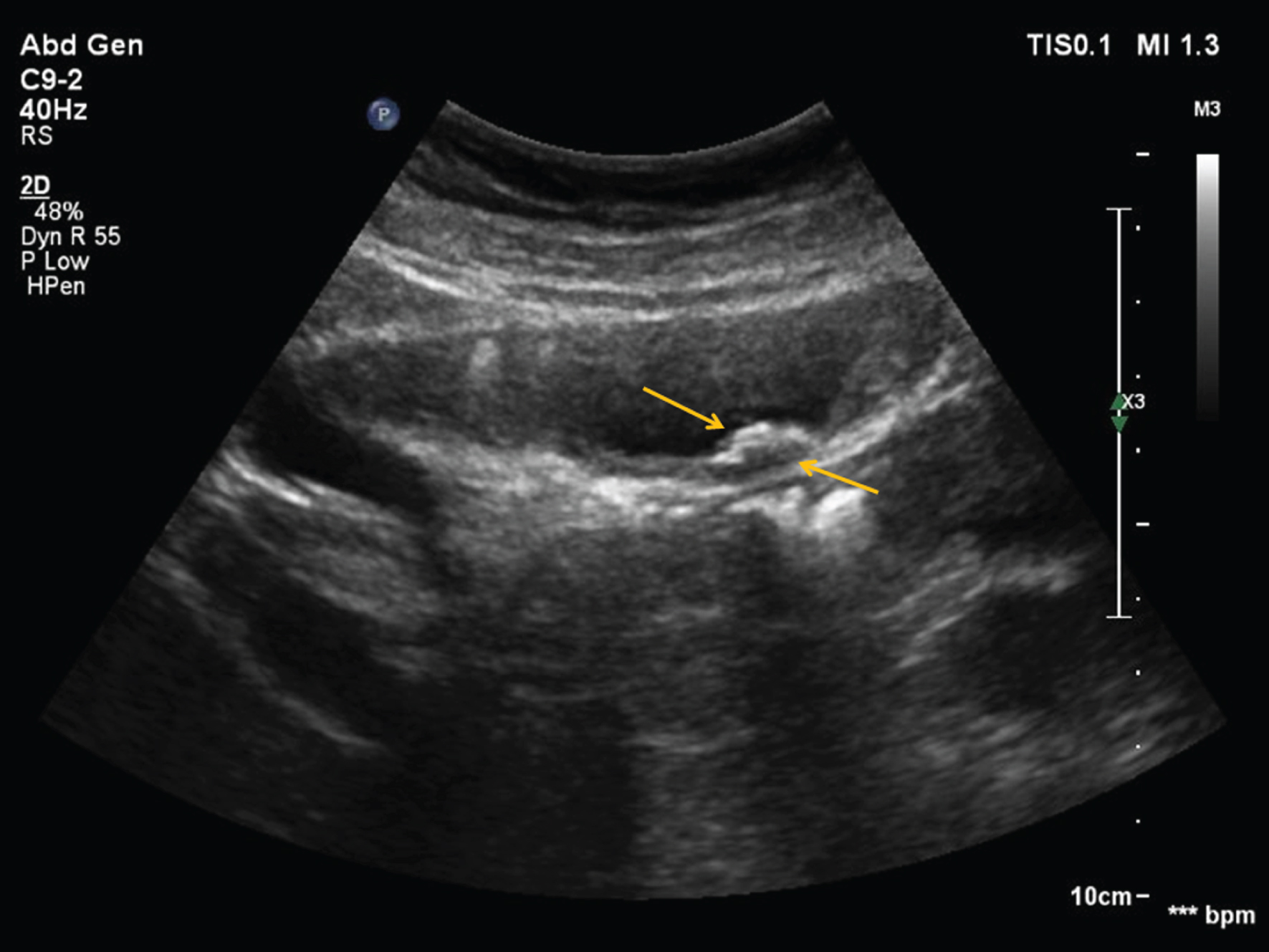
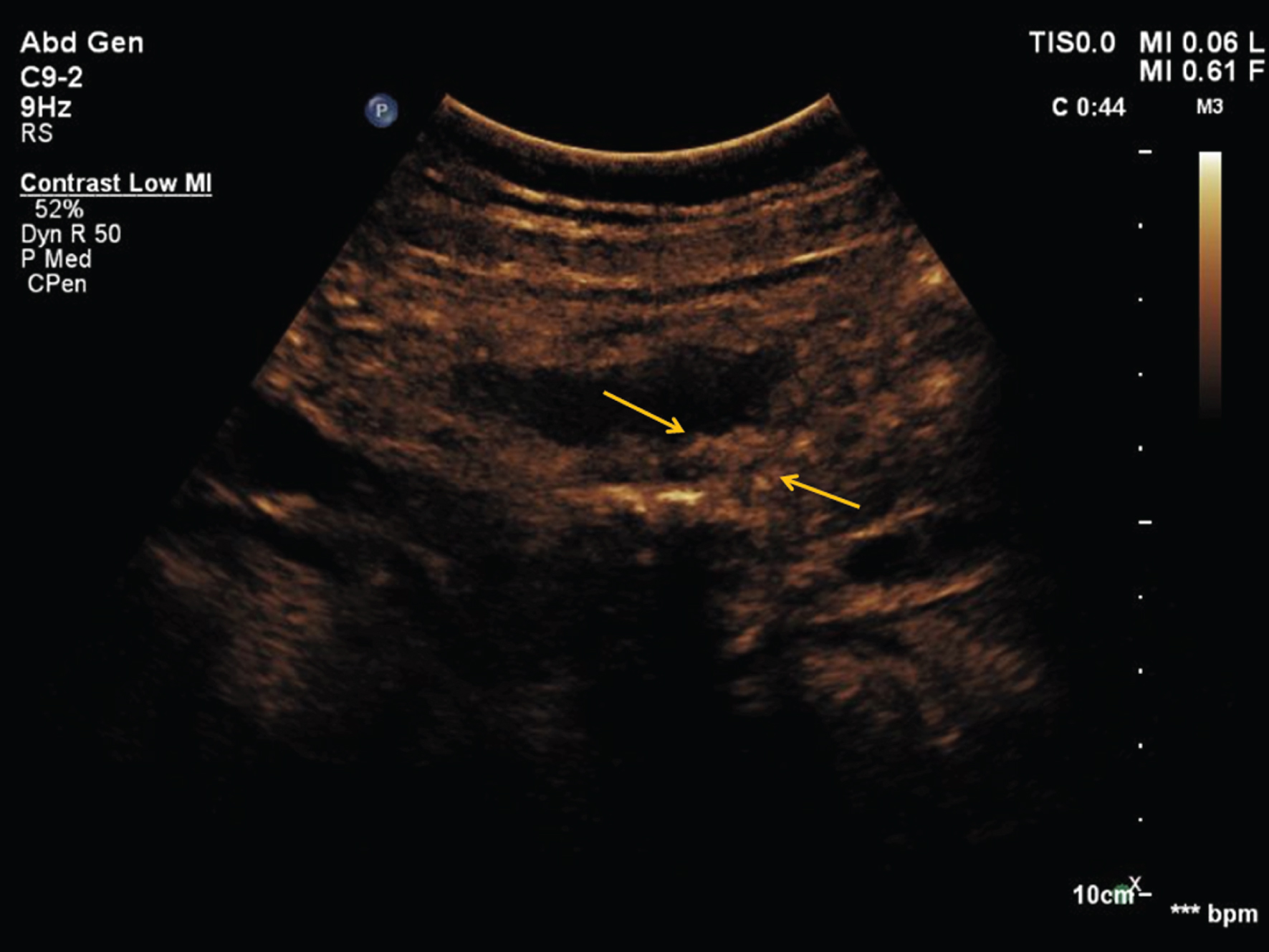
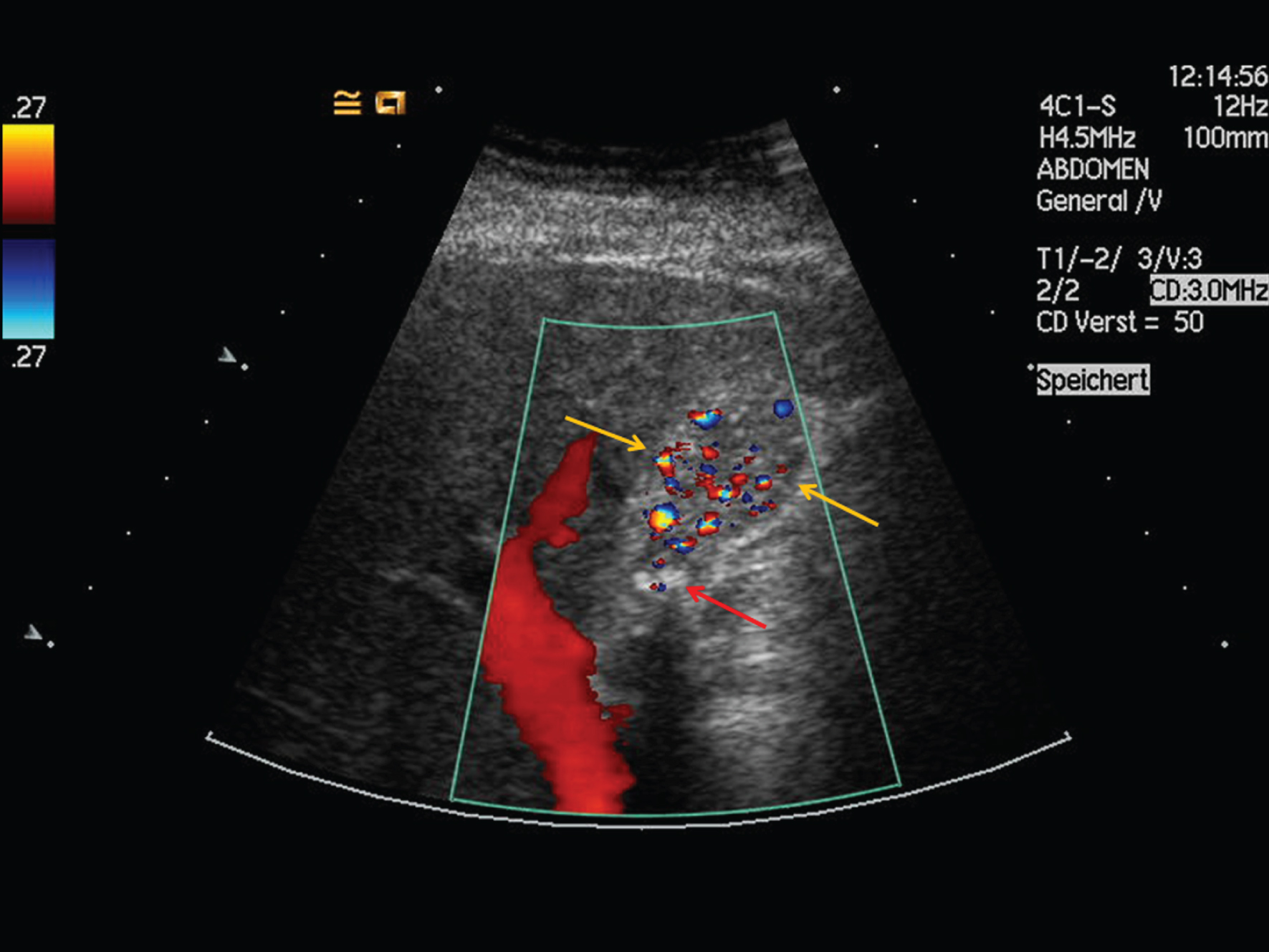
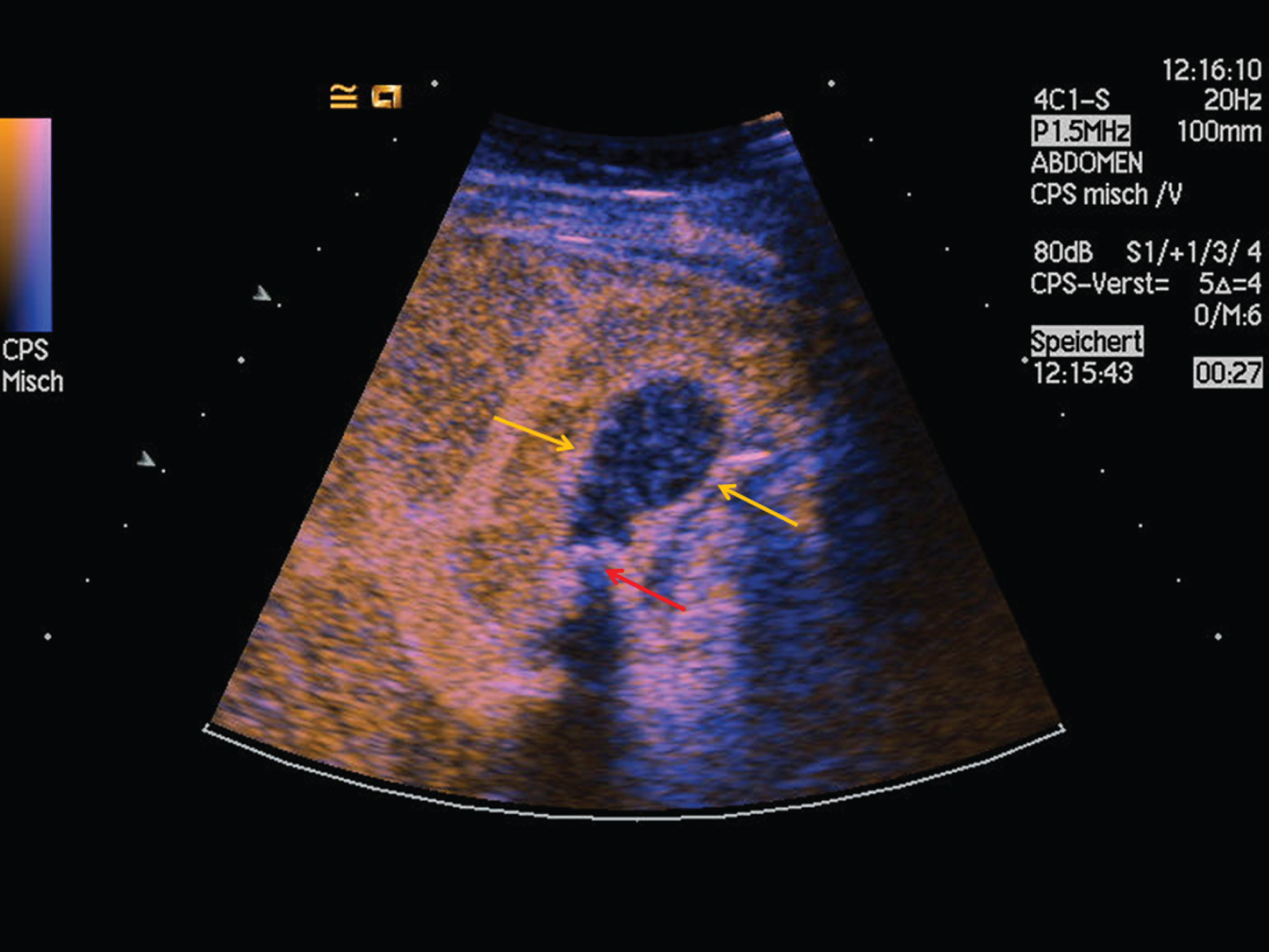
Same patient as in Figs. 6–8. Contrast-enhanced ultrasound (CEUS) shows a homogenous contrast uptake of the gallbladder wall. There were no signs of arterial hypervascularization or venous wash-out suggesting malignancy in line with sonographic features of an adenomyomatosis and in concordance to the CT findings.
In conclusion, the mono-center investigation of CEUS in gallbladder diseases acknowledged that CEUS is a feasible, valuable and safe additional diagnostic tool to differentiate gallbladder alterations such as benign or malign tumour, inflammation, sludge, polyps or anatomic perfusion variation. When compared to CT technique, CEUS shows a high diagnostic specificity and PPV not only in the detection of gallbladder pathology appearances but also in the diagnostic complementary information. Although this method has not been established as standard, patients with contraindications to CT or MRI imaging benefit from this method in the daily clinical routine.