
Abstract
BACKGROUND:
Conventional ultrasound and MRI are very important techniques for the detection of gallbladder alterations. In the past years, studies showed that the additional use of contrast media to the conventional ultrasound allows the early depiction of pathological microvessels and their flow elucidating suspect findings stipulating the prompt therapy approach.
OBJECTIVE:
The study aims to evaluate the performance of CEUS in gallbladder diseases and compare it to MR imaging using histopathological findings as a gold standard.
MATERIAL AND METHODS:
The retrospective mono-center study analysed 18 patients with gallbladder alterations between 2009 and 2017. All patients underwent CEUS and MRI examinations and all results were confirmed in the pathology. CEUS images were performed and interpreted by a single experienced physician.
RESULTS:
CEUS imaging results compared to MR imaging of the gallbladder demonstrated a sensitivity of 100%, specificity of 93%, a positive predictive value of 67% and a negative predictive value of 100%.
CONCLUSION:
CEUS enables the depiction and characterization of important vascularization’s patterns facilitating the early differentiation between malignant and benign findings. In this study, CEUS displayed a better diagnostic accuracy than MRI proving to be a valuable additional tool to the established imaging modalities.
Introduction
Ultrasound (US) is a very important tool in the early diagnosis of gallbladder carcinoma for the prompt therapy management [1]. The real-time conventional ultrasonography has an excellent spatial and temporal resolution enabling the detection of pathological alterations of the gallbladder. Moreover, this method is easy to perform, has no radiation and is cost-effective. However, in some cases, it is insufficient in clarifying suspicious US findings. Therefore, the application of a contrast agent has been used as an additional tool.
The contrast-enhanced ultrasound (CEUS) has been widely used in the last years as an established method for the assessment of suspicious lesions in organs such as kidney [2, 3], liver [4–8] and pancreas [9]. CEUS has been also used for displaying vascular pathologies such as flow velocity, aneurysms, leaks, critical stenosis or even dissections in small vessels [10, 11]. Different than the liver perfusion with a 3-phase vascularization [4], CEUS can demonstrate the vascularization pattern of the gallbladder during 2 phases: arterial (10–20 seconds postinjection); and late phase (31–180 seconds after contrast agent injection) because the blood supply of the gallbladder is provided entirely by the cystic artery and not by branches of the portal vein [12–16]. These two phases allow the vasculature depiction and characterization of suspicious masses, polyps and inflammatory reactions. However, as well as the conventional ultrasound, obese patients, patients with meteorism or noncompliant patients can decrease the validity of the examination.
The magnetic resonance imaging (MRI) is a very used technique that can assist the diagnosis of gallbladder diseases just like conventional US and CEUS. However, MRI cannot always be performed because of contraindications such heart pacemaker, metallic foreign body (metal sliver) and kidney impairment.
CEUS on the other hand, it is a safe tool because the contrast media applied has no renal or cardiac toxicity and can be performed in patients with renal and thyroid glands dysfunction [17, 18] as it does not contain iodine. Additionally, studies revealed the severe allergic responses are very rare - 1 in 10.000 cases [18, 19]. However, it is a foreign material and can produce a hypersensitivity reaction when recognized as so by the immune system [13, 14]. In large scale studies with CEUS, the reaction of hypersensitivity was reported with an incidence of ca. 0.002% [18, 19], reported as less than an examination with the use of an iodine contrast agent in computerized tomography (CT) and similar than the contrast agent used in MRI (gadolinium chelate). As any other contrast agent, SonoVue has also some contraindications such as: clinically unstable ischemic cardiac disease or recent acute coronary syndrome, severe pulmonary hypertension, right-to-left shunts, uncontrolled systemic hypertension and adult respiratory distress syndrome.
This retrospective mono-center analysis study aims to evaluate gallbladder diseases on CEUS and compare it with MRI.
Materials and methods
This study analysis was approved by the local institutional ethical committee of the institutional review board (IRB). Additionally, all authors respected the ethical guidelines for publication in Clinical Hemorheology and Microcirculation.
A total of 202 patients between 2009 and 2017 with gallbladder alterations were referred for CEUS examinations in our department after conventional ultrasound. Out of 202 patients, a subgroup of 18 patients underwent additional MRI examinations for diagnosis comparison. This retrospective study analysed 18 patients with CEUS and MRI examinations. CT was additionally performed in 3 patients. Out of 18 patients, 11 (61 %) were male and 7 (39%) were female. Mean age of patients was 59 years old (SD±19 years old), ranging in age from 25 to 89 years.
All results were histopathologic confirmed. In this study all CEUS examinations were included due to the excellent imaging quality acquired. Histopathologic analysis of a specimen as well as MRI were performed according to the valid techniques, protocols and classifications at the time of the examination. All 18 patients signed an oral and a written informed consent prior to each CEUS and MRI examination.
This study used several ultrasound systems (Siemens Acuson Sequoia and Siemens S2000, EPIQ 7, Philips Ultrasound), all high-end systems with CEUS specific protocols. Siemens ultrasound systems provided C4-1 and C6-1 HD probes for the examinations and Philips ultrasound system provided C9-2 probe. Each high-end ultrasound system was configured with a low mechanical index (always <0.2) in order to circumvent early destruction of microbubbles.
Fasting of at least 6 h prior each examination was necessary for a better interpretation of the gallbladder. A baseline greyscale US examination of the gallbladder and the adjacent liver was performed at first. Then, after the conventional evaluation of the gallbladder, a second-generation blood pool agent (SonoVue®, Bracco, Milan, Italy) was applied. The second-generation blood pool agent consists of phospholipid-stabilized shell microbubbles filled with sulfur hexafluoride gas. SonoVue® was administered as a bolus injection with an individual dose of 1.5 to 2.4 mL through a 20-gauge cannula placed in the antecubital vein. A flush-injection of 5–10 ml saline solution was followed. Normally, a single dose of contrast media was sufficient.
Cine loops of the study obtained were archived in the picture archiving and communication system (PACS) of our institution. Mean study time ranged between 3–5 minutes. During these 18 examinations, no adverse reactions were observed.

Native B-mode ultrasound of a male patient demonstrating an intraluminal mainly echogenic mass formation with irregularly shaped borders (yellow arrows).
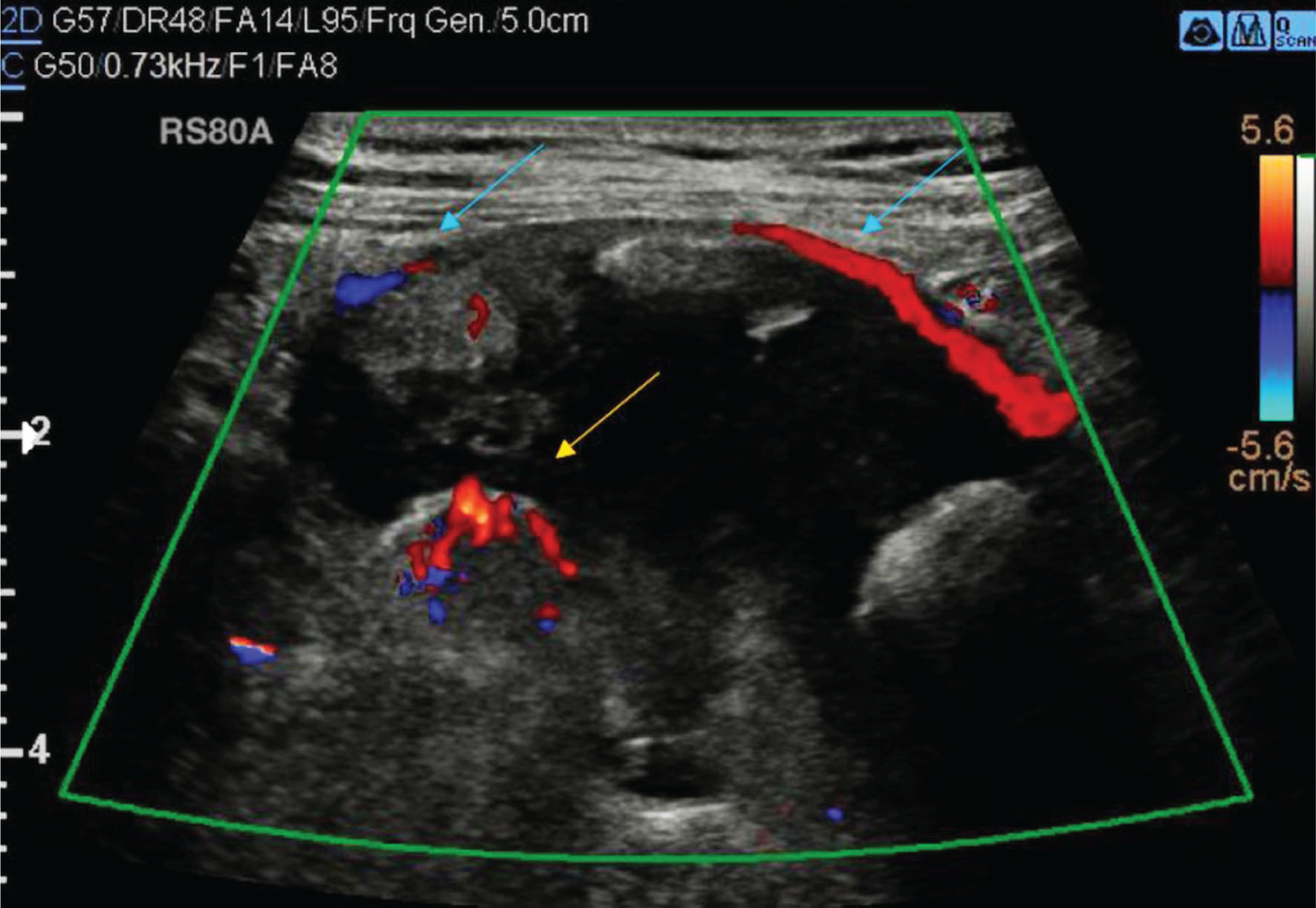
Same patient as in Fig. 1. Color Doppler shows the mass hypervascularization (yellow arrow) and the hypervascularization of the gallbladder wall (light blue arrows).

Same patient as in Figs. 1 and 2. CEUS shows an arterial hyperenhancement of the suspicious intraluminal mass of the gallbladder.


Native B-mode ultrasound of a female patient demonstrating an intraluminal echogenic oval shaped mass formation adjacent to the gallbladder wall (yellow arrows).

Same patient as in Fig. 5. Color Doppler shows no major hypervascularization of the gallbladder mass (yellow arrow).

CEUS, MRI and histopathological results of the study
A single proficient radiologist with more than fifteen years’ experience in conventional sonography and experience with CEUS since 2003 performed and interpreted all baseline B-mode US and CEUS studies. Senior radiologist that performed and interpreted all ultrasound examinations was blinded to MRI and pathology results. MRI examinations were also read by senior radiologists, with similar experience to the CEUS radiologist. All examinations were performed in a high-field-strength (1.5 Tesla) with phased array coils for signal reception. Despite protocol deviations, all patients received a routine clinical imaging protocol of the gallbladder with sequences before and after administration of contrast agent.
For this retrospective analysis, archived images and documentation files of all patients were retrieved from the PACS of our institution for the evaluation of gallbladder diseases on CEUS and for the comparison with MRI by testing sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV).
CEUS when compared to MRI results and histopathological findings presented a sensitivity of 100% and specificity of 93%, PPV of 67% and NPV of 100% (Table 1). CEUS and MRI demonstrated 2 cases of a suspicious malignant gallbladder alteration that were confirmed as adenocarcinoma (Figs. 1–7). In one case, suspicious malignant patterns of the gallbladder were depicted on CEUS and defined in MRI as a malignant infiltration of a liver tumor, which was confirmed in the histopathology as hepatocellular carcinoma (HCC).
CEUS was able to depict two cases with a focal benign hyperplasia of the gallbladder wall that was first suspected and afterwards pathologic confirmed as an adenomyomatosis of the gallbladder. However, MRI results was could only depict one of two adenomyomatosis of the gallbladder.
Moreover, CEUS depicted a gallbladder polyp in two cases which were also confirmed in the pathologic results but not sufficient demonstrated in the MRI. In the other patients CEUS and MRI displayed a cholecystitis pattern which was acknowledged in the pathology after cholecystectomy.
Discussion
When comparing the performance of CEUS and MRI in this study, the analysis showed a higher diagnostic accuracy of CEUS. Due to the real-time imaging method and the additional contrast media applied, CEUS displays the vascularization of a target lesion in two different phases (arterial and venous) increasing the diagnostic confidence. Moreover, the contrast agent administered overcomes the limitations of greyscale US displaying flow information of microvessels and demonstrating features such as gallbladder wall destruction or infiltration [20, 21]. The supplementary Color Doppler tool is not always able to depict vessel slow flow or deeply located vessels being more insensitive than CEUS.
This CEUS advantage allows the differentiation between a normal or a suspicious gallbladder alteration such as hypervascularizated focal or diffuse mass, thickened wall, irregular surface, irregular contrast enhancement. Additionally, CEUS can distinguish a focal mass from sludge or polyp.
CEUS of gallbladder alterations has already been compared to CT in a previous study with 24 patients presenting a sensitivity of 75% and a specificity of 100.0% [11]. As 3 patients of the previous study with CT [16] also had an MRI, MRI results were evaluated in this study summing a total 18 patients.
Although this study is a limited study because of the small number (n = 18) of patients with gallbladder alterations, the performance of CEUS in the depiction and classification of gallbladder alterations has already been demonstrated in other studies [22–27]. Moreover, it is important to note that the results of this study might be biased in favor of CEUS because single proficient radiologist performed and interpreted all the examinations. However, there is no other alternative for the recruitment of patients with gallbladder alterations in the routine. Furthermore, interpretation of exams requires a senior radiologist with long term expertise as this field is very limited, with no available other physicians inside our department.
This study was able to show that CEUS when compared to MRI demonstrated a higher diagnostic performance. Both methods (CEUS and MRI) were able to depict a suspicious malignant mass in the gallbladder with features of malignancy such as irregular surface, tortuous arterial enhancement [22–24] and its early washout, which is alone not a specific criterion for malignancy as already proved in previous studies [18–20]. Additional features such as disrupted wall, tortuous-type vascularity and patient age have also to be cogitated as criteria for malignancy [22–24]. However, results might differ depending on the physician that performs the CEUS examination, the size of the alterations and not specific malignant features [22, 23].
After cholecystectomy, histopathologically results confirmed the imaging results by reporting the suspicious tumor as an adenocarcinoma of the gallbladder (Figs. 1–7). As the prognosis for gallbladder carcinoma has a low overall prevalence [24], its early recognition is essential.
In one case, CEUS and MRI also demonstrated suspicious features of malignancy such as tortuous-type vascularity, disrupted wall and arterial enhancement and pathological results clarified the alterations as an infiltration of a malignant liver tumor. In this case, MRI was able to show the liver mass and its infiltration.
Adenomyomatosis is a benign alteration of the gallbladder that is described a thickened gallbladder wall with small avascular cystic spaces. CEUS is normally performed when this pathology cannot be clarified in the native B-mode US. MRI should be performed if CEUS still have unclear results. CEUS displays the adenomyomatosis pattern as a focal, segmental, or diffuse hyperplasia of the gallbladder wall with anechoic cysts. As the cysts are avascular and sometimes bile-filled, CEUS shows in the arterial phase a “moth-eaten” enhancement of the gallbladder wall, simultaneously to the parenchyma enhancement of the liver [25]. MRI, missed one case of adenomyomatosis in this study because the signal intensity of the avascular cystic spaces varies widely depending on their content despite its extremely high sensitivity. Normally, the intramural cystic spaces are hypointense on T1-weighted images, hyperintense on T2-weighted images and nonenhancing [26, 27]. In some cases, intraluminal calculi appear differently, they show signal voids due to their mineral content [26, 27].
Cholecystitis and its inflammatory pattern were depicted on CEUS and in MR without any difficulties. The inflammatory pattern of the gallbladder wall on CEUS consists of a homogeneous, fast, and intense enhancement of the thickened gallbladder in the arterial phase.
Finally, it is also important to emphasize that patients with contraindications to other cross-sectional modalities such as MRI benefit from CEUS because it is a safe technique as it has no radiation and the contrast media used has no renal, thyroid or cardiac toxicity [17–19].
Conclusion
Ultrasound is the imaging modality of choice for the conventional evaluation of gallbladder alterations. The additional use of a contrast agent in US enables the depiction and characterization of important patterns of vascularization that allows the early differentiation between malignant and benign findings accelerating the recommended therapy management.
In this study, CEUS displayed a better feasibility and diagnostic accuracy than MRI proving to be a valuable additional tool to the established imaging modalities.