
Abstract
PURPOSE:
To assess the value of conventional ultrasound (US), contrast-enhanced ultrasound (CEUS) and mammography in the diagnosis of breast lesions with calcifications.
METHODS:
A total of 87 breast lesions with calcification were subjected to US, CEUS and mammography and divided into 3 groups: Group A (all cases), Group A1 (31 cases who underwent US and CEUS first followed by mammography), and Group A2 (56 cases who underwent mammography first followed by US and CEUS). A receiver operating characteristic (ROC) curve analysis was performed to evaluate the diagnostic efficacy of different methods in different groups.
RESULTS:
In Group A, the area under the ROC curve (AUROC) of CEUS were 0.937, which were significantly higher than that of mammography (p < 0.05). In Group A1, the AUROC of CEUS were 0.842, which were not significantly different from that of US and mammography (p > 0.05). In Group A2, the AUROC of CEUS were 0.987, which were significantly higher than that of mammography and US (p < 0.05).
CONCLUSION:
Based on the mammography results, the combination of US and CEUS might improve the diagnostic efficacy in breast lesions with calcification.
Introduction
Breast cancer is a major cause of death in women worldwide [1]. Comprehensive breast cancer control involves early detection, diagnosis, and treatment, and early detection is the cornerstone in breast cancer control. Previous studies have shown that the detection of irregular microcalcifications are of great significance in preoperative evaluation of lesion extent and in the posttreatment surveillance of breast cancer patients [2, 3]. Calcifications involve mineral deposits presenting in both benign and malignant breast masses, but these two types of lesions differ in size and distribution [4].
Mammography mainly helps reduce the rate of death from breast cancer, with extreme sensitivity to calcification [5, 6]. Most Chinese women possess relatively dense breast tissues, and a microlesion or lesion in the overlapping part may be overlooked in imaging diagnosis, thereby resulting in complications in the interpretation of mammography images [7, 8]. In addition, a lesion that is located at the edge of a small breast is easily misdiagnosed.
Conventional ultrasonography (US) is another established clinical diagnostic method that is inferior to mammography for detecting microcalcifications [9]. Fischer et al. suggested that sonographic detection of microcalcifications with a 14 MHz probe in stereotactic biopsy specimens could correlates well with digital mammography [10]. US is useful in estimating lesion appearance, but its sensitivity is relatively low with respect to the detection of flow in tiny vessels.
Contrast-enhanced ultrasond (CEUS) as a significant method to visualise the microcirculation and overcomes the disadvantages of conventional US, that is becoming an increasingly popular imaging method in the diagnosis of breast cancer [11–16]. CEUS is good at observe angiogenesis and microcirculation which play an important role in the local growth, invasion, and distant metastasis of cancer [17, 18]. CEUS-guided biopsy increases the accuracy of tumour diagnosis by targeting hyperperfused viable area-inner lesions, which are usually invisible or poorly visible on US [19, 20]. Moreover, CEUS is radiation-free and free from positioning limitations. Some studies found that combining US with CEUS could improve the diagnostic sensitivity and efficacy of breast lesions [21–24]. Shao SH et al. reported that incorporation of CEUS to re-evaluate lesions can improve the diagnostic efficacy comparing to mammography (MG) or US alone [25]. These studies focused on the breast lesions regardless of calcification. Hardly seen that research focused on the breast lesions with calcification in CEUS due to difficulties in observation of the calcification, but CEUS could benefit the discovery of the microcirculation around the calcifications. Compare to mammography, US and CEUS could directly locate the lesion more accurately. Because the scanning posture is the same as the posture when patient is on the operational table.
Based on the respective advantages of mammography, US, and CEUS, this study aimed to evaluate the value of multimodality imaging in the differentiation of breast lesions with calcification found on both mammography and US.
Patients and methods
Patients
From April 2009 to September 2017, 87 breast lesions with calcification obtained from 85 patients (mean age 44 years; range 26–74 years) were included in the final data analysis. As the Breast Imaging Reporting and Data System (BI-RADS) is a widely used classification system to classify benign and malignant breast lesions and to guide surgical treatment by sorting US or mammography results into categories from 0 to 6. The inclusion criteria were as follows: breast lesions with calcification having been originally classified as BI-RADS 3, 4A, 4B, 4C, or 5 with US and patients undergoing CEUS and mammography at the same time. The following patients were excluded from the study: those who were pregnant, breastfeeding, previously treated, or had an interventional diagnosis (BI-RADS 6). All cases were followed up for one year. A total of 87 lesions were divided into three groups: Group A, 87 total cases; Group A1, 31 cases that underwent US and CEUS first, followed by mammography; and Group A2, 56 cases that underwent mammography first, followed by US and CEUS.
Written informed consent was obtained from all patients, and the approval from the Institutional Ethics Committee of the hospital for this study was waivered.
US examination
An IU22 (Philips Medical Systems, Bothell, WA, USA) ultrasonic scanner was used to perform the 2D ultrasonographic examination (using a 12-5 MHz linear transducer) and CEUS (using a 9-3 MHz linear transducer). The contrast agent SonoVue (Bracco SpA, Milan, Italy) was used in CEUS. Side-by-side image mode was selected to locate the lesion accurately during the CEUS procedure, and B-mode pulse inversion harmonic imaging was used for CEUS.
The mechanical index was set at 0.06. The imaging depth varied from 3 to 5 cm depending on the size and location of the lesions in the breast. The contrast agent suspension consisted of 59 mg of SonoVue powder mixed with 5 mL of saline; it was administered into the antecubital vein via a 20-gauge cannula. CEUS was performed immediately after a bolus injection of 4.8 mL of contrast agent followed by a 5 mL saline flush via the intravenous cannula. Real-time images were recorded up to 90 s for further analysis.
Mammography examination
Routine bilateral digital MG (Giotto Image; IMS, Bologna, Italy) was performed and consisted of at least the mediolateral oblique and craniocaudal views of the breast. Additional views or spot compression views were obtained where appropriate.
Image analysis
Ultrasonography and mammography US imaging data were independently analysed by two ultrasonographers who had >10 years of experience in US and 5 years in CEUS. Mammography images were read by two radiologists, both with >10 years of experience in breast radiology. All image readers were blinded to the pathological information, clinical histories, and other imaging findings. When image readers had different opinions on suspected cases, they reached a consensus. In accordance with the BI-RADS lexicon, the 87 lesions were divided into five categories (3, 4A, 4B, 4C, and 5) in US and seven categories (1, 2, 3, 4A, 4B, 4C, and 5) in mammography. BI-RADS 1, 2, 3, and 4A in US, CEUS, and mammography were considered benign lesions with high probability (BI-RADS 4A is a critical point with a very low suspicion of malignancy that needs follow-up), and BI-RADS 4B, 4C, and 5 were considered malignant lesions with high probability. In addition, US and CEUS characteristics were analysed between benign and malignant lesions.
CEUS CEUS uses a rule for reclassified US BI-RADS scores through CEUS, which referenced the “rerated BI-RADS” method [23, 24]. Table 1 shows how CEUS reclassifies US BI-RADS categories 3–5 to become CEUS BI-RADS: for US BI-RADS 3 or 4A: (1) when the lesion is not enhanced or shows iso- and synchronous enhancement without a clear outline in CEUS or is earlier enhanced in size or smaller than that in the 2-D image, then the lesion categories remain unchanged to CEUS BI-RADS 3 or 4A; (2) when the lesion is earlier enhanced and larger than that in the 2-D image, then the US BI-RADS categories should increase by one level to CEUS BI-RADS 4A or 4B; and (3) when the lesion is earlier enhanced and larger than that in the 2-D image with heterogeneous enhancement or a typical crab claw-like enhancement, then the US BI-RADS categories should be increased by two levels to CEUS BI-RADS 4B or 4C. Similarly, the reclassified rule for US BI-RADS 4B, 4C, and 5 is the same as that described in Table 1.
Rules for reclassification of US BI-RADS scores through CEUS
Rules for reclassification of US BI-RADS scores through CEUS
BI-RADS = Breast Imaging Reporting and Data System; CEUS = contrast-enhanced ultrasonography; US = conventional ultrasonography.
Histologic confirmation was made by the use of a core needle biopsy or surgical excision after examinations by US, CEUS, and mammography. The pathological findings were used to confirm the diagnosis.
Statistical analysis
SPSS 22.0 software (SPSS, Inc., Chicago, IL, USA) was used for recording data and statistical analyses. McNemar’s test was used to examine the diagnostic accuracy, specificity, and sensitivity of US BI-RADS, CEUS BI-RADS, and mammography BI-RADS. A Z-test was conducted to compare the areas under the receiver operating characteristic curve (AUROCs). A chi-square test was used to examine the patterns of US and CEUS.
Results
Characteristics of breast lesions with calcification
There were 87 lesions with calcification detected by US from 85 patients, of which 35 were breast carcinomas and 52 were benign breast lesions (mean diameter 1.65 cm±1.25 cm). Among the carcinomas, 29 (82.9%) were invasive ductal carcinomas, and 6 (17.1%) were ductal carcinomas in situ. Among the benign lesions, 18 (34.6%) were fibroadenomas, 21 (40.4%) were fibrocystic mastopathies, 8 (15.4%) were intraductal papilloma, 3 (5.8%) were chronic mastitis, 1 (1.9%) was sclerosing adenosis, and 1 (1.9%) was invasive syringomatous adenoma. Among the 52 benign breast lesions, 33 had microcalcification, 18 had macrocalcification, and 1 had mixed calcifications (both microcalcification and macrocalcification). Among the 35 breast carcinomas, 32 had microcalcification, and three had mixed calcification. Tables 2 and 3 summarise the image patterns of US and CEUS between the benign and malignant breast lesions with calcification, with two representative cases shown in Figs. 1 and 2.
US patterns of benign and malignant breast lesions
US patterns of benign and malignant breast lesions
†Of the 87 breast lesions, six benign lesions with calcifications did not demonstrate clear solid mass in US and were excluded in the US pattern analysis, leaving 46 benign lesions. US = conventional ultrasonography.
CEUS patterns of benign and malignant breast lesions
†In the total 87 breast lesions, six benign lesions with calcifications did not demonstrate clear solid mass in US and were then excluded in the US pattern analysis, leaving 46 benign lesions. ‡In the remaining 81 breast lesions, four benign lesions were non-enhanced in CEUS which could not be analysed and were then excluded. CEUS = contrast-enhanced ultrasonography; US = conventional ultrasonography.
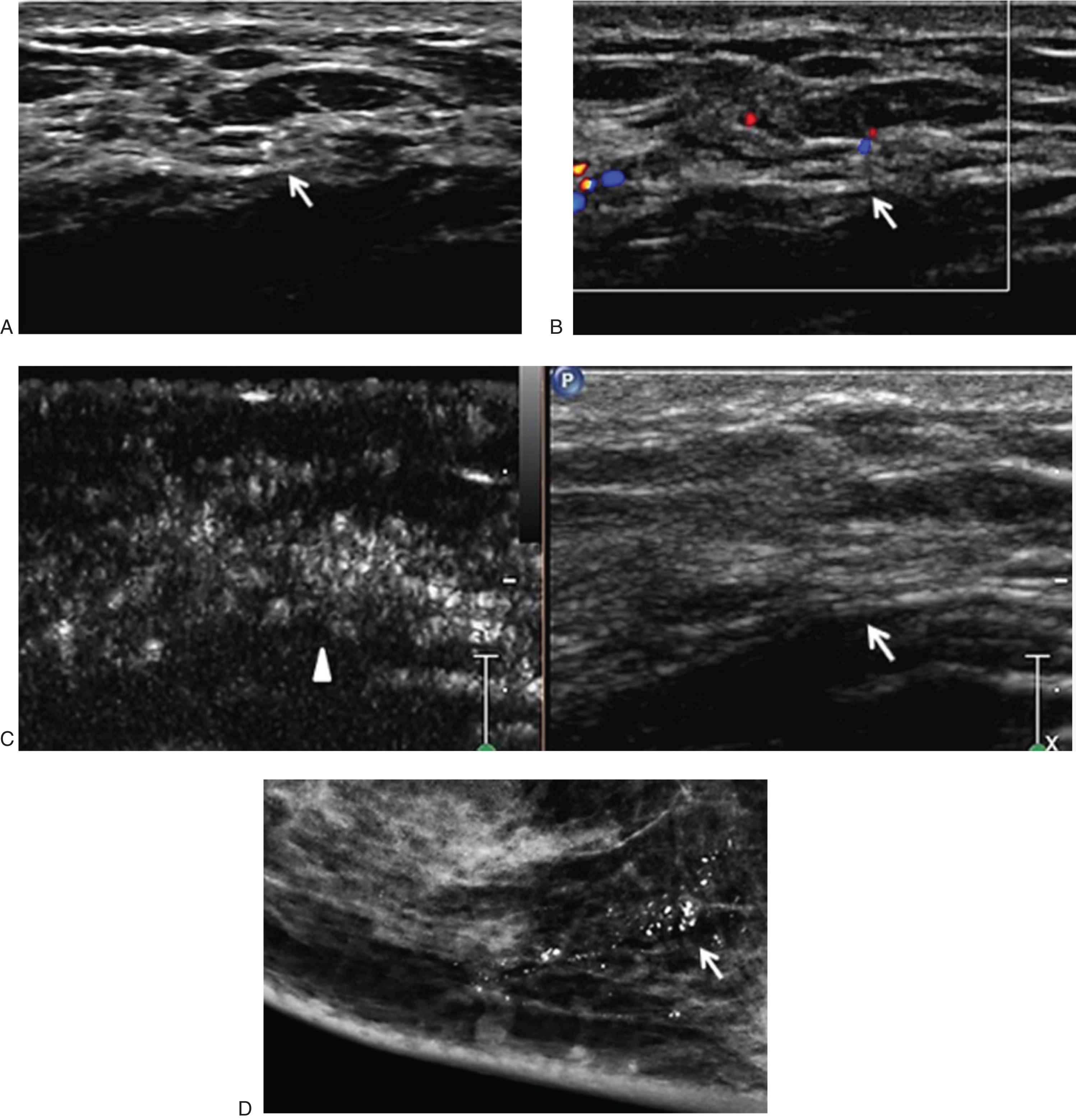
A 39-year old woman was found to have calcifications in the right breast in a medical check-up. US of the breast lesion categorized as BI-RADS 4A (Fig. 1A and 1B). It was reclassified as CEUS BI-RADS 4A (Fig. 1C). It was categorized as BI-RADS 4B by mammography (Fig. 1D). The pathology of the lesion was fibrocystic mastopathy with hyaline change (lesion marked with white ‘↑’, CEUS enhancement range marked with white ‘▴’). BI-RADS = Breast Imaging Reporting and Data System; CEUS = contrast-enhanced ultrasonography; US = conventional ultrasonography.

A 53-year-old woman was found to have mass in the right breast for 1 month. US scan of the breast lesion categorized the lesion as BI-RADS 4A (Fig. 2A and 2B). It was reclassified as CEUS BI-RADS 4C (Fig. 2C). It was categorized as BI-RADS 5 by mammography (Fig. 2D). The pathology of the lesion was invasive ductal carcinoma (lesion marked with white‘↑’, CEUS enhancement range marked with white ‘▴’). BI-RADS=Breast Imaging Reporting and Data System; CEUS = contrast-enhanced ultrasonography; US = conventional ultrasonography.
ROC curves were constructed to reflect the diagnostic efficacy of US, CEUS, and mammography in the differentiation of benign and malignant breast lesions with calcification in the three groups (Fig. 3). The corresponding sensitivity, specificity, accuracy, and AUROC of the three methods in the three groups are shown in Tables 4 and 5.
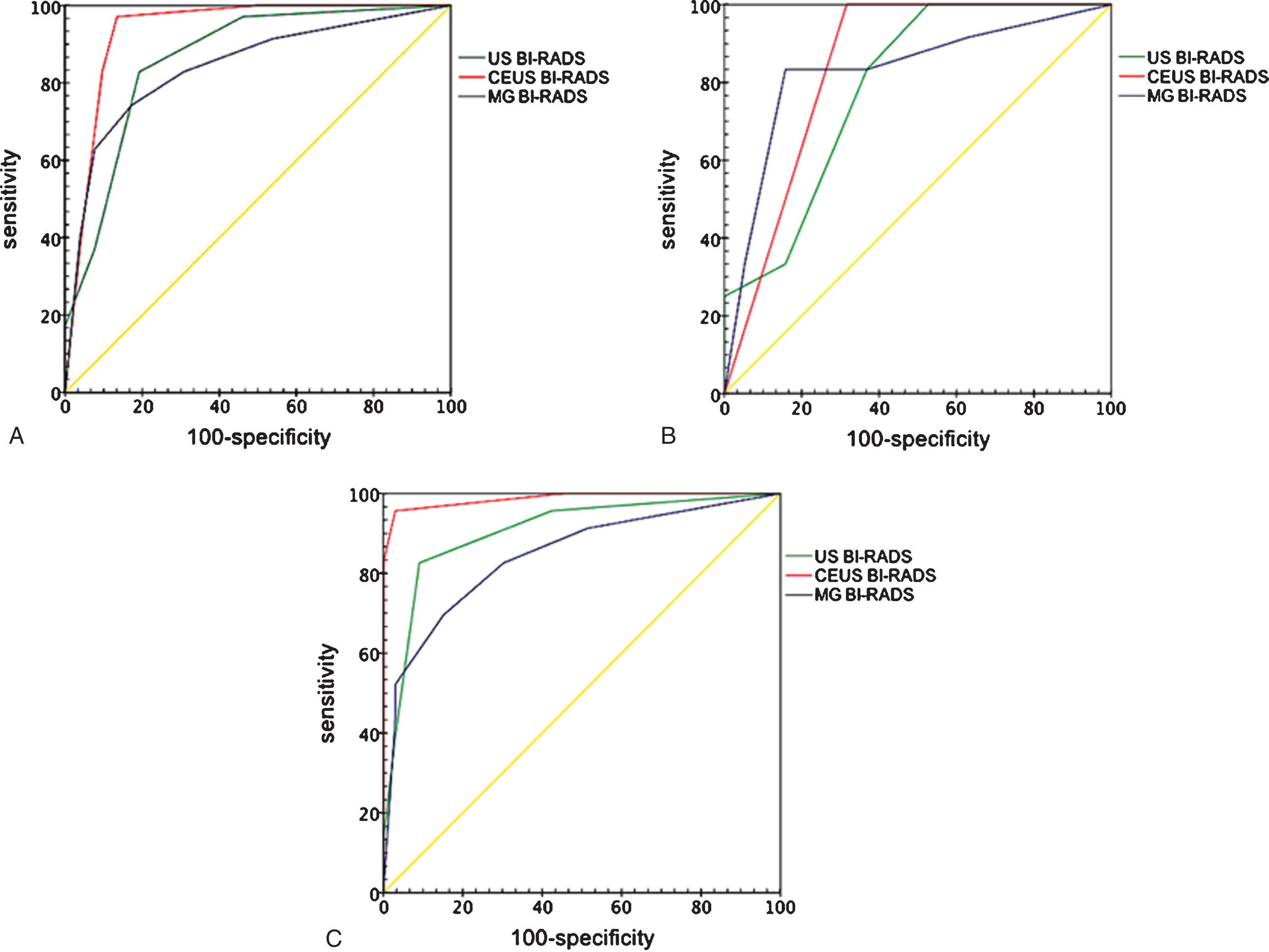
ROC curves representing the diagnostic efficacy of US, CEUS, and MG in three groups. The AUROC for US, CEUS, and MG were 0.863, 0.937, and 0.842 in Group A (Fig. 3A), and 0.787, 0.842, and 0.829 in Group A1 (Fig. 3B), and 0.905, 0.987, and 0.844 in Group A2 (Fig. 3C). AUROC = area under the receiver operating characteristics curve; BI-RADS = Breast Imaging Reporting and Data System; CEUS = contrast-enhanced ultrasonography; MG = mammography; US = conventional ultrasonography.
Diagnostic performance of the three methods in the differentiation of benign and malignant breast lesions with calcification in Group A
avs. US BI-RADS p < 0.05; bvs. MG BI-RADS p < 0.05. AUROC = area under the receiver-operating characteristics curve; BI-RADS = Breast Imaging Reporting and Data System; CEUS = contrast-enhanced ultrasonography; MG = mammography; US = conventional ultrasonography.
Diagnostic performance of the three methods in the differentiation of benign and malignant breast lesions with calcification in Group A1 and Group A2
e vs. f (McNemar’s test), p = 0.012; j vs. i (Z-test), p = 0.034; j vs. k (Z-test), p = 0.006; e vs. a (Mann-Whitney U test), p = 0.015, Z = –2.426; g vs. b (Mann-Whitney U test), p = 0.015, Z = –2.421; h vs. c (Mann-Whitney U test), p = 0.004, Z = –2.876. j vs. d (Z-test), p = 0.024. BI-RADS=Breast Imaging Reporting and Data System; CEUS = contrast-enhanced ultrasonography; MG = mammography; US = conventional ultrasonography.
In Group A, the diagnostic specificity, sensitivity, accuracy, and AUROC of CEUS were 86.5%, 97.1%, 90.8%, and 0.937, respectively. The accuracy was remarkably higher than that of US (p < 0.05), while the sensitivity, accuracy, and AUROC were significantly higher than those of mammography (p < 0.05). In Group A1, the diagnostic specificity, sensitivity, accuracy, and AUROC of CEUS were 68.4%, 100%, 80.6%, and 0.842, respectively, which were not significantly different from those of US and mammography (p > 0.05). In Group A2, the diagnostic specificity, sensitivity, accuracy, and AUROC of CEUS were 97.0%, 95.7%, 96.4%, and 0.987, respectively. The accuracy and AUROC were significantly higher than those of mammography, and the AUROC was significantly higher than that of US (p < 0.05). The diagnostic specificity, accuracy, AUROC of CEUS, and diagnostic specificity of US were increased remarkably in Group A2 compared with those in Group A1 (p < 0.05).
The diagnostic accuracy of CEUS BI-RADS for lesions falling into BI-RADS category 4 (especially 4A) was higher than that of US alone in Group A. As shown in Table 6, of the 19 lesions in US BI-RADS 4A, five malignancies were misdiagnosed and upgraded to CEUS BI-RADS 4B after CEUS scans; of the 22 US BI-RADS 4B lesions, 6 benign lesions were over diagnosed, and 3 were downgraded to CEUS BI-RADS 3 or 4A after CEUS scans.
This study employed US, CEUS, and mammography to assess breast lesions with calcification and assessed whether the combination of US, CEUS, and mammography could observably improve the diagnostic efficacy in breast lesions with calcification. The study showed that under the guidance of mammography results, the combination of US and CEUS (CEUS BI-RADS) could observably improve the diagnostic efficacy in breast lesions with calcification.
US is highly useful in estimating tumour size, shape, echogenicity, perfusion, macrocalcification, and other characteristics [26]. An irregular shape, indistinct margin, posterior shadowing, and rich vascularity were more likely to indicate malignant lesions, as shown in Table 2. US is also able to detect most microcalcifications (with a maximum diameter of 1 mm), which are often an important signal indication of breast cancer [27]. The diagnostic sensitivity of calcification with US is inferior to that of mammography, and US is unable to reveal the distribution patterns of calcification, which can help distinguish between benign and malignant lesions. This study showed that approximately 63% of benign lesions had microcalcifications, indicating that microcalcifications exist in both benign and malignant breast lesions. In addition, the microvasculature of breast lesions is undetectable by colour Doppler due to the low velocity and breathing or heart beat artefacts of the patient [28]. Therefore, the US diagnosis of a breast lesion with calcification is limited.
Generally, magnetic resonance imaging (MRI) is the normal examination for contrast imaging in breast, and is a label use after the results of many multicenter studies. The paramagnetic contrast medium enables clear visualization of breast mass vascularization and tumour angiogenic bed [22]. Although CEUS is not the standard examination in breast cancer, this study focused on using CEUS to differentiate between benign and malignant lesions which had found calcification in both US and mammography. In CEUS examination, a patient in the supine position could simulate the surgical position and makes surface marker more precisely, which has greater advantage in nonpalpable breast tumor. In addition, CEUS is more convenient, real-time dynamics, and patients are more tolerant of.
In CEUS, malignant breast lesions are characterised by an enlarged enhancement range, heterogeneous hyper-enhancement, perfusion defect, indistinct margins, and radial or penetrating vessels, as shown in Table 3. The CEUS contrast agent, which is confined to the vascular lumen, improves colour Doppler signals, especially in the microvasculature [29, 30]. The microvasculature between the benign and malignant breast lesions is different. Vessels in benign breast lesions are singular and circumferential, with a regular and tapering course. Vessels in malignant breast lesions are tortuous, with more peripheral vessels than benign breast masses. Therefore, the scope of the malignant lesion is markedly larger in CEUS than the scope indicated in US [17]. Although there are many new vessels in the tumour tissue, the tortuosity and irregularity of new vessels and the fast growth of the malignant tumour destroy the tissue structures, including blood vessels [18]. Therefore, the disturbed tissue structure usually leads to the formation of necrotic centres and calcifications, which present as perfusion defects in CEUS. The calcification is unobservable in CEUS; hence, this is a limitation for the diagnosis of breast lesions with calcification by CEUS only.
The microvasculature, size, and distribution of calcifications are all important in the differentiation of benign and malignant breast lesions. We therefore combined US and CEUS based on reclassified US BI-RADS scores through CEUS. The results showed that CEUS BI-RADS improved the diagnostic value in 87 breast lesions with calcification, especially CEUS BI-RADS 4A and 4B lesions, which was well-matched with previous study [31]. As shown in Table 6, of the 19 4A lesions classified by US BI-RADS, five are actually malignancies and further reclassified as 4B by CEUS BI-RADS. In these five malignancies, US showed microcalcifications with suspicious shapes, and CEUS characterised the malignant features of an enlarged enhancement range and perfusion defects. Of the 22 US BI-RADS 4B lesions, six benign lesions were overdiagnosed, and three were rectified to CEUS BI-RADS 3 or 4A. These overdiagnosed lesions had microcalcifications and mimicked malignant patterns in US, such as indistinct margins, a heterogeneous internal echo, and an irregular shape, and one lesion grew vertically. Because three of the six overdiagnosed US BI-RADS 4B lesions were not enhanced or showed no change in the enhancement range in CEUS, the lesions were reclassified as US BI-RAD 3 or 4A (benign lesions).
Diagnostic performance of US BI-RADS scores re-classified by CEUS in Group A
BI-RADS = Breast Imaging Reporting and Data System; CEUS = contrast-enhanced ultrasonography; US = conventional ultrasonography.
Mammography is better than US in determining the morphological types and distribution patterns of breast calcifications [2, 32]. The distribution of calcifications between benign and malignant breast lesions is significantly different. Benign calcifications commonly appear as regional distribution, with diffuse or scattered distribution, while patients with calcifications distributed along the ducts, grouped or clustered, or with linear and segmental distributions are at a significantly increased risk of malignancy [33, 34]. In Group A, the diagnostic sensitivity, accuracy, and AUROC of CEUS were significantly higher than those of mammography in the 87 breast lesions with calcification. In order to explore whether mammography affect the diagnosis of CEUS, we divided Group A into two groups according to the checking order: Group A1 underwent US and CEUS first, followed by mammography, and Group A2 underwent mammography first, followed by US and CEUS. In Group A1, no significant difference was found in the diagnostic specificity, sensitivity, accuracy, or AUROC between US, CEUS, and mammography. In Group A2, the diagnostic accuracy and AUROC of CEUS were significantly higher than those of mammography, and the diagnostic specificity, accuracy, and AUROC of CEUS were increased remarkably compared with those in Group A1. In addition, the diagnostic specificity, sensitivity, accuracy, and AUROC of mammography were not significantly different between Group A1 and Group A2. This finding indicates that the combination of US and CEUS might increase the diagnostic performance of US under the guidance of mammography and significantly benefit more patients, but US did not help improve the diagnostic performance of mammography, which showed no advantage to patients. Because US represents real-time dynamics, ultrasonographers can find the lesions more accurately based on the location of the calcification in mammography, storing high-quality and specific images, which could facilitate good performance of retrospective studies. Mammography images are fixed and overlapping and do not obviously help radiologists, even with information on the location of the lesion on US images. In general, in China, US is regarded as a routine screening method for breast diseases, but mammography is not. Hence, mammography screening should be recommended first, followed by US, which is more meaningful.
Nevertheless, it is challenging to diagnose some unusual breast lesions even with multimodality imaging. Misdiagnosis of chronic inflammatory disease is common. Chronic inflammatory diseases usually present with an irregular shape, indistinct margin, scattered calcifications, and rich blood supply. The inflammation often extends into adjacent interlobular and peripheral tissue and causes liquefaction necrosis that is revealed as an enlarged range of enhancement and perfusion defects in CEUS [35]. Syringomatous adenoma of the nipple (SAN) is an extremely rare benign tumour and does not metastasise. It is an infiltrative but noninvasive neoplasm histologically and generally appears as a high-density mass in the subareolar region that is extremely similar to a malignant neoplasm in terms of its shape in mammography [36]. In this study, SAN was misdiagnosed and regarded as a malignancy with hypoecho, irregular shape, unclear margin, scattered microcalcifications, rich blood supply, and enlarged range of enhancement.
In addition, nonparallel orientation is considered, in general, one of the typical sonographic features of breast malignancy [37]. However, no correlation was found between nonparallel orientation growth and the risk of malignancy according to this study (Table 2). This result could be due to the small study sample size. No difference was found in CEUS enhancement order of centripetal, centrifugal or diffuse. Even it may be difficult to accurately observe such enhancement order of CEUS in small lesions, but CEUS is useful to differentiate benign from malignant small breast lesions (size less than 10 mm) [38]. For more lesions, CEUS is relatively weaker because it is difficult to observe all the lesions at the same plane, and MRI would be more suitable [39]. Liu GF et al. found that the accuracy (71.05%) of triple negative subtypes by CEUS was lower than other subtypes, and could be improved remarkedly (81.58%) combined with diffusion-weighted MRI [40]. CEUS could greatly improve diagnostic accuracy for non-mass breast lesions with microcirculation, but the lesions without neovascularization may not be detected [41]. Therefore, CEUS could be an appositional tool but not the only contrast imaging method for detection of breast tumors in an early stage. Furthermore, digital breast tomosynthesis (DBT) has a higher resolution and is more sensitive than mammography [42]. Shear wave elastography (SWE) could measure the stiffness of lesion and significantly improve the diagnostic performance of US [43]. Hence, in certain circumstances other imaging modality might be more appropriate.
This study has a few limitations. The number of cases and types of breast lesions were limited. Second, some unusual breast lesions were difficult to classify even with multimodality imaging. Third, this is a single centre study, which may have influenced the results. Fourth, MRI, SWE and DBT were not involved in the research. Therefore, more cases, further multicenter studies, MRI, SWE and DBT exam accessions are required.
Under the guidance of mammography, the location and distribution of calcification might be more accurately identified, then apply the combination of US and CEUS to observe the profile of the lesion and especially the microcirculation. The combination of these three image modalities improves the diagnostic efficacy in breast lesions with calcification. In addition, it could reduce unnecessary trauma caused by core needle biopsy or surgery.
Footnotes
Acknowledgments
The work was supported by National Natural Science Foundation of China (81530055).