
Abstract
OBJECTIVE:
To evaluate and optimize the additional diagnostic value of Doppler imaging for malignant NMLs detected by US.
MATERIALS AND METHODS:
The characteristics of 233 NMLs in Doppler imaging were analyzed, and different Adler grades of intralesional vessels were selected as the diagnostic cutoffs on Doppler imaging: grade 1 in the full cohort and in women < 40 years, and grade 0 in women ≥40 years. The diagnostic performance of US and US + Doppler imaging were calculated and compared with that of mammography.
RESULTS:
The AUC of US + Doppler was larger than that of US alone in each group (P < 0.001). In the full cohort, addition of Doppler imaging increased specificity of US, but decreased sensitivity. However, by use of different diagnostic cutoffs in the two subgroups, it was possible to achieve high sensitivity and specificity simultaneously, which were 100% and 75.8% in women < 40 years, 94.7% and 69.5% in women ≥40 years, respectively. The AUC + Doppler was comparable to that of mammography in the full cohort and in women ≥40 years. In women < 40 years, the AUC of the combination was larger than that of mammography (P < 0.001).
CONCLUSION:
Doppler imaging, with different Adler grades used as cutoffs in older versus younger women, can improve the specificity of US for the diagnosis of malignant NMLs without losing sensitivity. In younger women, US + Doppler imaging may be better than mammography.
Introduction
Mammography and ultrasound (US) imaging are the two main imaging modalities for breast cancer screening [1–4]. According to the Breast Imaging Reporting and Data System (BI-RADS) published by the American College of Radiology [5], in addition to masses, breast abnormalities detected on mammography can be described as calcifications, architectural distortion, and focal asymmetric density. However, the BI-RADS still has no standardized description for non-mass breast lesions (NMLs) detected on two-dimensional US. Radiologists generally use the terms hypoechoic area, architectural distortion, and ductal changes to describe these lesions [6–9]. NMLs—irrespective of whether they are benign or malignant—usually present in US images with irregular shape and ill-defined margins. US, therefore, has a high false-positive rate (60% –90%) in the diagnosis of malignant NMLs [9–12]. Although advanced US techniques (contrast-enhanced US or elastosonography) can improve diagnostic efficiency [11–14], their application is limited by nonavailability of equipment and lack of physicians’ experience. Considering the importance of US in breast cancer screening, especially in developing countries with scarce medical resources [15–17], it is necessary to find an economical and convenient method to optimize its diagnostic efficiency.
Doppler imaging is a noninvasive technique to study the blood flow characteristics of lesions, and most US scanners come equipped with the facility. Moreover, new Doppler techniques such as Glazing flow and high-resolution flow have proved to be useful for evaluating hemodynamic changes and can even capture very low-velocity blood flow [18]. Over the past three decades, a series of researches have proved that Doppler imaging is a valuable supplement to US for the diagnosis of breast cancer; however, the diagnostic value of Doppler imaging in malignant NMLs has not been fully investigated [19, 20]. In this study, we assessed whether addition of Doppler imaging to US could improve diagnosis of malignant NMLs and whether the diagnostic performance could be optimized by age grouping. We also compared the diagnostic performance of US + Doppler with that of mammography.
Materials and methods
Patients
Approval for this retrospective study was obtained from our institutional review board (No. 2019KY055). Informed consent was not required because of the retrospective nature of the study.
We searched our hospital database for all US examinations performed between January 2017 and December 2020 and identified 314 patients who underwent breast US for suspected NMLs. Patients were eligible for inclusion in this retrospective analysis if 1) NML was diagnosed on US; 2) there was no previous history of breast surgery, biopsy, chemotherapy, or radiotherapy; and 3) diagnosis had been confirmed by biopsy or surgical pathology or, alternatively, with no suspicious findings on mammography, US, or MRI after follow-up for > 2 years. A total of 216 patients (with 223 NMLs) met these criteria and were included in the study.
US protocol and interpretation
US examinations were performed by one of four dedicated breast radiologists, each with 8–12 years’ experience. High-resolution US systems equipped with high-frequency linear transducers (5–14 MHz) were used: either Logiq E9 (GE Medical Systems, USA) or Aplio 500 (Toshiba Medical Systems Corporation, Japan). US was first performed on both breasts. When a lesion was detected, the size (maximum diameter) and morphological characteristics were observed and evaluated. NMLs were classified according to the 5th edition of BI-RADS-US [5]. The evaluation indicators were lesion sharpness (round/oval/irregular), lesion margin (clear/indistinct/speculated/angular), aspect ratio (≥1/< 1), posterior features (attenuation/enhancement/no change), and calcifications (present/absent).
Color and power Doppler imaging were then performed to observe the blood-flow signals inside and in the periphery of the lesions. The machine settings for optimized imaging were: wall filter, medium; color scale preset to a low velocity (≤4 cm/s); and color sampling frame surrounding the lesion and peripheral normal breast tissue without angulation. Multi-site sampling was performed when the lesion was large. The probe was placed gently on the breast surface to prevent compression of small blood vessels in the lesion. The color gain was first increased until background noise appeared and then reduced until the noise just disappeared; this was performed so as to obtain maximum sensitivity for blood flow signal. The following qualitative characteristics of NMLs in Doppler imaging were evaluated: Intralesional vessels within NMLs, which were graded according to the Adler classification as: Grade 0 = no blood flow signals. Grade I = one to two punctate or small rod-shaped vessels (diameter < 1 mm). Grade II = three to four punctate vessels or one long vessel (with length approaching or exceeding the radius of the lesion). Grade III = more than four punctate vessels or two long vessels [21]. The blood-flow signals distribution, which was classified as central, peripheral, or both peripheral and central Presence or absence of penetrating vessels, which were defined as vessels extending from outside into the body of the lesion [22].
Spectral Doppler imaging was then used to measure the peak systolic velocity and resistivity index of the arteries in the NML. The angle between the US beam and blood flow direction was ≤60°. The measurement was performed on all vessels in hypovascular NMLs (grade I/II) and on at least three vessels in hypervascular (grade III/IV) NMLs; the maximum value was included.
For this study, all US images were retrospectively reviewed by two radiologists, each with more than 12 years’ experience in breast US; discordant interpretations were discussed till a consensus was reached. Both radiologists were blinded to the findings of other imaging modalities and the pathologic diagnosis. Lesions without space-occupying effect on US images were recognized as NMLs.
Mammography examination and interpretation
Of the 233 patient in this study, 55 did not receive mammography examination; the reasons included age < 40 years (29 patients), nipple discharge (8 patients), and refusal of mammography due to fear of pain (18 patients). All mammographic images were acquired with a full-field digital system (Senographe DS; General Electric Medical Systems, USA). The examinations were carried out by one of two qualified technicians, each with more than 5 years’ experience in mammography. For each breast, the images of two standard views (mediolateral oblique and craniocaudal) with local pressure were obtained through fully automated exposure control. For this study, two radiologists with 8-years’ and 10-years’ experience, respectively, in mammography retrospectively interpreted the images in consensus. They were blinded to all information from other imaging modalities and the pathology findings. Breast density and abnormalities (mass, asymmetry, architectural distortion, and calcifications) were assessed according to the criteria of the 5th edition of BI-RADS-MG [23].
Statistical analysis
Quantitative variables were summarized as means±standard deviation and compared between groups using the independent t-test. Categorical variables were summarized as percentages and compared using the chi-square test or Fisher exact test. The sensitivity, specificity, and area under the receiver operating characteristics curve (AUC) for diagnosis of malignant NMLs were calculated separately for US, US + Doppler imaging, and mammography. The McNemar test was used to compare sensitivities and specificities of the three methods, and the Z test to compare the AUCs. SPSS 20.0 (IBM Corp., Armonk, NY, USA) was used for data analysis. P < 0.05 was considered statistically significant. BI-RADS category 1–3 were considered benign NMLs and BI-RADS category 4-5 as malignant NMLs.
Results
Lesions
Of the 233 NMLs, 150 (64.4%) were benign and 83 (35.6%) were malignant. More than 85% of women with malignant NMLs were above the age of 40 years. The benign NMLs included adenosis (n = 67), inflammation (n = 21), sclerosing adenosis (n = 8), intraductal papilloma (n = 9), and duct ectasia (n = 6). The most common malignant NML was ductal carcinoma in situ (DCIS; n = 31), followed by invasive ductal carcinoma (IDC; n = 21), IDC + DCIS (n = 23), invasive lobular carcinoma (n = 3), intraductal papillary carcinoma (n = 2), mucinous carcinoma (n = 1), and solid papillary carcinoma (n = 2).
US findings
Table 1 summarizes the US features of the 233 NMLs. In US images, one NML was hyperechoic, while all others were hypoechoic. Malignant NMLs were significantly more likely than benign NMLs to display calcifications (49.4% vs. 4.7%, P < 0.001) and posterior features (22.9% vs. 10.7%, P = 0.034). In Doppler imaging, high Adler grades of the intralesional vessels (87.9% vs. 42.7%, P < 0.001) and penetrating vessels (28.9% vs. 8.0%, P < 0.001) were more common in malignant NMLs. The resistivity index was higher for malignant NMLs than for benign NMLs (0.72 vs. 0.61, P < 0.001).
Ultrasound findings in benign versus malignant non-mass lesions
Ultrasound findings in benign versus malignant non-mass lesions
Data are presented as mean±standard deviation and number (percentage). Independent t test was used to compare quantitative variables, and the chi-square test or Fisher exact test to compare categorical variables.
To optimize the additional diagnostic value of Doppler imaging for malignant NMLs, we analyzed the influence of patient age (< 40 years and ≥40 years) and lesions size (maximum diameter < 20 mm and ≥20 mm) on the distribution of benign and malignant NMLs in different Adler grades (Fig. 1). We observed that, among all 233 NMLs, with the exception of Adler grade 0, the proportion of benign and malignant NMLs in other Adler grades overlaps strikingly. Moreover, this overlapping was seen even after the lesions were grouped by size. However, after age grouping, we found that all NMLs in Adler grade 0 were benign lesions in the group < 40 years, and that the proportion of benign and malignant NMLs overlapped less in Adler grade I.

Distribution of benign and malignant NMLs in different Adler grades: subgroup analysis according to age and lesion size.
Table 2 summarizes the mammography findings for 178 NMLs detected on US. Dense breasts were more frequent than non-dense breasts (57.3% vs. 42.7%), but the proportion with dense breasts was comparable between patients with benign and malignant lesions (P = 0.727). While 103 NMLs detected on US presented non-mass appearance in mammography, 24 NMLs presented as masses; the remaining 51 NMLs did not show any abnormalities on mammography. Calcifications were the most common finding in mammography in both benign and malignant NMLs (24.2% vs. 34.5%, P = 0.218). Calcifications with asymmetry or architectural distortion were more common in malignant NMLs (21.7% vs. 1.1%, P < 0.001) (Figs. 2 and 3).
Mammography findings in benign versus malignant non-mass lesions
Mammography findings in benign versus malignant non-mass lesions
Mammography findings were available for 95 benign and 83 malignant non-mass lesions.
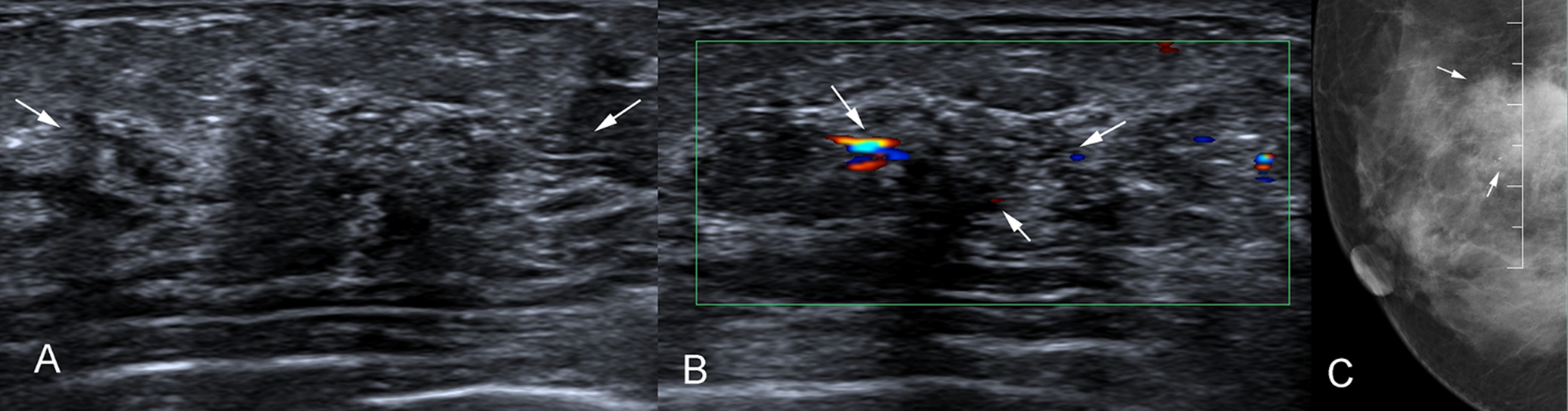
A 44-year-old woman with invasive ductal carcinoma of the breast shows hypoechoic area with calcifications in ultrasound (A). Doppler image shows intralesional hypervascularity, which was classified as Adler grade III (arrows, B). Mammography shows heterogeneously dense breast with calcifications and asymmetry (arrows, C).

A 53-year-old woman with adenopathy and ductal epithelial hyperplasia of the breast shows ductal changes in ultrasound image (A). Doppler image shows intralesional hypovascularity, which was classified as Adler grade 0 (arrows, B). Mammography shows scattered fibroglandular breast tissue with asymmetry (arrows, C).
In Doppler imaging, Adler grade I has generally been used as the cutoff for classifying blood supply in lesions as low or abundant [11, 25]. We therefore used Adler grade 1 as the cutoff to reclassify the BI-RADS US category of NMLs in the whole sample of 233 patients. The BI-RADS US category was upgraded when the Adler grade was more than grade I, otherwise it was downgraded. However, because age grouping changed the proportion of benign and malignant NMLs in different Adler grades, we used Adler grade 1 as the cutoff in the < 40 years age-group and Adler grade 0 as the cutoff in the ≥40 years age-group.
Table 3 summarizes the diagnostic performance of US versus US + Doppler imaging. On US, 164 NMLs were assessed as BI-RADS 4a; however, 133 (81.1%) of these lesions were actually benign. US had extremely high sensitivity (83/83, 100%) but very low specificity (13/150, 8.7%) for the diagnosis of malignant NMLs. More than 50% of the NMLs rated as BI-RADS 4 on US were re-rated as BI-RADS 3 by the combination of US + Doppler imaging. In the total study population, the specificity of US + Doppler was significantly higher than that of US alone (75.3% vs. 8.7%, P < 0.001), but the sensitivity was significantly decreased (79.5 % vs. 100%, P < 0.001). However, in subgroup analysis, the increased specificity was not accompanied by significant decrease in sensitivity in either the < 40 years group or the ≥40 years group (P > 0.05). The AUC of US + Doppler imaging was significantly higher than the AUC of US alone in both age-groups (P < 0.001).
Diagnostic performance of ultrasound alone and ultrasound + Doppler imaging for malignant non-mass lesions
Diagnostic performance of ultrasound alone and ultrasound + Doppler imaging for malignant non-mass lesions
US, ultrasound; BI-RADS, Breast Imaging Reporting and Database System.
The diagnostic accuracy of US alone, US + Doppler imaging, and mammography were compared in the subset of 178 patients who had undergone all three examinations (Table 4). BI-RADS 4a was the most common category of NMLs (57.7% and 50%) in the total sample of 178 patients and in the ≥40 years group, but not in the < 40 years group. US had a higher sensitivity than mammography for diagnosis of malignant NMLs (100% vs. 73.5%, P < 0.001) but it had much lower specificity (5.3% vs. 73.4, P < 0.001). In the total sample, the AUC of US was smaller than the AUC of mammography (0.526 vs. 0.725, P < 0.001), but the AUC of US + Doppler imaging was comparable to the AUC of mammography (P > 0.05). In the < 40 years group (with Adler grade 1 as the cutoff), the AUC of US + Doppler imaging was larger than the AUC of mammography in (0.824 vs. 0.629, P < 0.001); but in the ≥40 years group, the AUC of US + Doppler imaging was not significantly different from the AUC of mammography (0.763 vs. 0.767, P = 0.926).
Diagnostic performance of ultrasound alone and ultrasound + Doppler imaging, and mammography for malignant non-mass lesions
Diagnostic performance of ultrasound alone and ultrasound + Doppler imaging, and mammography for malignant non-mass lesions
US, ultrasound; AUC, area under the curve; BI-RADS, Breast Imaging Reporting and Data System.
US has been recommended as a supplement or alternative to mammography in breast cancer screening because of its low cost and the absence of radiation exposure [4, 27]. Consistent with previous studies [9–12], we found that US has high sensitivity but low specificity for diagnosis of malignant NMLs. In our study cohort, 90% of benign NMLs were overestimated as BI-RADS 4; such overestimation could result in a large number of unnecessary biopsies. For cancer screening, high sensitivity is desirable, but low specificity can limit the clinical usefulness of the test, especially when it results in invasive procedures [28].
Neovascularization is essential for tumor growth, infiltration, and metastasis, and so evaluation of neovascularization in imaging examinations is important for diagnosis, treatment monitoring, and prognosis prediction. Doppler imaging and contrast-enhanced US (CEUS), as traditional and advanced US techniques, respectively, can both detect blood flow signals. Unlike Doppler imaging, which cannot detect low-velocity blood flow, CEUS, which uses gas-filled microbubbles as blood pool agents, can sensitively display macro- and microcirculation in the target lesion in real time. Numerous studies have confirmed the value of CEUS in the diagnosis and treatment of malignant tumors. In smaller tumors, the addition of CEUS can be crucial for diagnosis [29–31]. However, due to nonavailability of experienced medical personnel and costs, CEUS is less often used than Doppler imaging. In the present study, we attempted to investigate whether addition of Doppler imaging could improve the diagnostic accuracy of US for NMLs.
In previous studies, due to the different Doppler parameters (vessel morphology, vessel density, and resistivity index) used as diagnostic criteria, the sensitivity and specificity of Doppler imaging in the diagnosis of breast cancer has varied widely (62.0% –90.5% and 56% –95%, respectively) [32–34]. In this study, we found that malignant NMLs tended to have abundant blood supply, more penetrating vessels, and higher resistivity index than benign NMLs; this is similar to the differences seen between malignant and benign breast masses [35–37]. To reduce subjective differences in interpretation of Doppler imaging and simplify workflow, we used only the Adler grades of intralesional vessels as the diagnostic criterion for Doppler imaging of malignant NMLs. We found that when Doppler imaging was added to US, and Adler grade 1 was used as the cutoff in the total cohort, the diagnostic specificity for malignant NMLs increased from 8.7% to 75.3%, but it was accompanied by a decrease in sensitivity from 100% to 79.9%. This is in contrast with the results of Li et al. [20] who reported that the combination of Doppler imaging and US increased sensitivity for the diagnosis of malignant NMLs, with minimal impact on specificity. The differences between the studies may be due to the different assessment methods used for intralesional vessels. Moreover, Li et al. used BI-RADS 4b as the cutoff to distinguish malignant from benign NMLs, with the result that the sensitivity of US alone was just 84.8% in their study. Using the same diagnostic criteria, Choi et al. [19] also showed that the diagnostic specificity of US for malignant NMLs increased with decrease of sensitivity after the addition of Doppler imaging.
To optimize the additional diagnostic performance of Doppler imaging, we further observed the distribution characteristics of benign and malignant NMLs in different Adler grades by age or size grouping. We found that, in the overall study population, the proportion of benign and malignant NMLs overlapped greatly in Adler grade 1, resulting in reduced sensitivity. However, in different age-groups, the Adler grades with more overlap between benign and malignant NMLs were different (grade 2 in < 40 years and grade 1 in ≥40 years groups). Thus, we used different Adler grades as the diagnostic cutoffs (grade 1 and grade 0) in the two age-groups and effectively improved both sensitivity and specificity of US + Doppler imaging. The AUC of the combination was significantly larger in both age subgroups than the AUC in the total study cohort (P < 0.001).
Mammography is irreplaceable for detecting calcifications in breast cancer and is the recommended first-line screening test for breast cancer in many countries. In this study, 178 NMLs underwent both US and mammography; the agreement rate for diagnosis of NMLs was 57.9%. Calcifications were the most prominent sign of NMLs in mammography, with the detection rate on mammography being about twice than that on US (46.4% vs. 22.5%). Consistent with previous studies [11, 37], we found no significant difference in the prevalence of simple calcifications between benign and malignant NMLs (P = 0.218); however, calcifications with asymmetry or architectural distortion were more often seen in malignant NMLs (P < 0.001). Thus, in addition to calcifications, which is an important sign in breast cancer, asymmetry or architectural distortion of the breast gland on mammography are useful indicators of malignancy.
Many studies have shown that breast density is the main cause of decreased sensitivity of mammography for diagnosis of breast cancer [37–39]. In our study, 12 malignant NMLs correctly identified by US were not identified on mammography due to high breast density. This resulted in decreased sensitivity of mammography for diagnosis of malignant NMLs, particularly in the < 40 years age group, which had a high proportion (73.8%) of patients with dense breasts; however, the specificity of mammography remained high. The AUC of mammography was higher than that of US (P < 0.001). When Doppler imaging was added to US, the AUC was comparable to that of mammography in the total study cohort and in the ≥40 years group (P > 0.05); however, in the < 40 years group, the AUC of US + Doppler imaging was higher than that of mammography (P < 0.001) due to both high sensitivity and specificity. This further confirmed that using different diagnostic cutoffs on Doppler imaging in different age-groups is an effective method for improving diagnosis of malignant NMLs.
Our study has several limitations. First, this was a retrospective study with a limited sample size; the findings need to be verified in large prospective studies. Second, penetrating vessels and resistivity index are important parameters in Doppler imaging, but their diagnostic value for NMLs was not analyzed in this study. Third, we did not calculate interobserver and intraobserver variability in the interpretation of US and mammography; however, the final diagnosis for malignant NMLs was based on consensus. Fourth, Doppler imaging is difficult to optimize in low flow areas and angle depending, and the results depend greatly on the examiner’s experience.
Conclusion
Doppler imaging is a convenient and feasible additional diagnostic tool for US, and can improve the specificity of US for diagnosis of malignant NMLs, but it may cause a decrease in sensitivity. However, this can be overcome by using different diagnostic cutoff Adler grades on Doppler imaging as the diagnostic criteria in older (≥40 years) and younger (< 40 years) women. The combination of US and Doppler imaging may be better than mammography for diagnosis of malignant NMLs in younger women.
Footnotes
Acknowledgments
This work was supported by the National Natural Science Foundation of China (Grants Nos.82071931, 82130057), the Program for Shanghai Outstanding Medical Academic Leaders (2019LJ18), the interdisciplinary program of Shanghai Jiaotong University (ZH2018ZDA17), and the Program from Science and Technology Commission of Shanghai Municipality (No. 20Y11912400).