
Abstract
OBJECTIVE:
To investigate the diagnostic value of core-needle biopsy (CNB) guided by contrast-enhanced ultrasound (CEUS) in cervical tuberculous lymphadenitis (CTL).
METHODS:
178 patients with pathological confirmation of CTL were retrospectively enrolled. All of them had undergone CNB prior to the final surgery. According to the different ways of puncture guidance, they were divided into two groups: conventional ultrasound (US) group (n = 81) and CEUS group (n = 97). The comparison of diagnostic efficacy between two groups was compared and analyzed.
RESULTS:
Among the 178 patients, 146 were directly diagnosed as CTL by CNB, including 59 patients in CEUS group and 87 patients in US group. The diagnostic accuracy were 89.7% (87/97) and 72.8% (59/81), respectively (P < 0.01). For subgroup analyses, differences among diagnostic efficacy ascribed to the different guiding methods were significant in medium size group (>2.0 cm and ≤3.0 cm) and large size group (>3.0 cm), 91.7% for CEUS group vs. 69.0% for US group (P < 0.05) and 84.4% for CEUS group vs. 57.7% for US group (P < 0.05), respectively.
CONCLUSIONS:
In the diagnosis of CTL, compared with the US-guided CNB, CEUS-guided CNB have certain advantages, especially for larger lymph nodes.
Introduction
Estimated by World Health Organization (WHO) in 2019, a population of 10 million fell ill with tuberculosis (TB) and 1.5 million people died from TB –made it the world’s top infectious killer, despite being a preventable and curable disease [1]. Mycobacterial infection was supposed to be an associated factor for mycobacterial lymphadenitis, which could occurred in any demographic features, whatever age, gender, race are. Tuberculous adenitis is considered to be an acknowledged cause of lymphadenopathy regionally, especially in China. Though cervical tuberculous lymphadenitis (CTL) was reported to be a common extrapulmonary tuberculosis by prior study [2], it still remains a serious of indeterminate points on diagnosis, since radiologists would be easily confused when mimicking lymphoma, solid malignancy, connective tissue disease or infections like brucellosis [3]. It was believed that any delayed diagnosis or misdiagnosis may lead to worse prognosis, including fistula formation and unhealing for a long time.
The lymph node biopsy could be mostly performed by excision, fine-needle aspiration (FNA) and conventional ultrasound (US) guided core-needle biopsy (CNB) [4, 5]. Although excision is regarded as the golden standard, it’s not accepted because of the trauma and scar sometimes [6]. US-guided CNB now has drawn worldwide attention for the less invasiveness and higher tolerability compared with excision in determining the nature of lymphadenopathy [7–9]. Otherwise, the tissue obtained by US-guided CNB is stay in the entirety of biological structure compared with FNA, which enables various immunostaining [3]. It was reported that the sensitivity of US-guided CNB to liver tumor is around 90% [10], but lower to cervical lymphadenitis.
In the prior decades, tremendous progress in needle design and ultrasound based techniques has been made by percutaneous biopsy [11], including color Doppler, power Doppler, navigation systems, imaging fusion and contrast-enhanced ultrasound (CEUS) [12–16]. According to prior studies, CEUS has been supposed to be a promising and less invasive method which is based on the application of intravenous contrast agent. In some cases, the nature of lesion could be predicted through the characterization of blood perfusion reflected by CEUS. Benefits gained in this way are wildly distributed in liver, kidney, lymph node and so on [17–21], nowadays in COVID-19 patients as well [22]. However, limited attention was focused on the contribution that CEUS-guided CNB made to the diagnosis of CTL. Consequently, the present study was aimed to investigate the role of CEUS-guided CNB played in the diagnosis for CTL.
Materials and methods
Patients
With relevant guidelines and regulations complied, the current study was approved by the Ethical Committee of Hangzhou Red Cross Hospital and informed consents were obtained from all patients. From January 2018 to December 2019, 178 patients (61 males, 117 females, aged from 18 to 71 years, mean 36.70±11.358 years) were retrospectively enrolled, and these patients were pathologically confirmed as CTL by surgery finally. Prior the resection of the lymph node, either US guided CNB or CEUS guided CNB was performed. The eligibility criteria for enrollment were: (1) Patients underwent either US-guided CNB or CEUS-guided CNB, and then resected the lymph node. (2) No therapeutic history. (3) Processing the most suspicious one if multiple lesions occurred in one patient. (4) Images and videos were complete, and clinical information was available in the institute medical record system. Pathological diagnosis resulted from excision paraffin section was referred as the golden standard in current study. The flowchart of the study is present in Fig. 1. Lesions were divided into 3 groups according to the size, including small size group (i.e. diameter was not larger than 2.0 cm), medium size group (i.e. diameter was between 2.0 cm and 3.0 cm with 3.0 cm included) and large size group (i.e. diameter was larger than 3.0 cm).
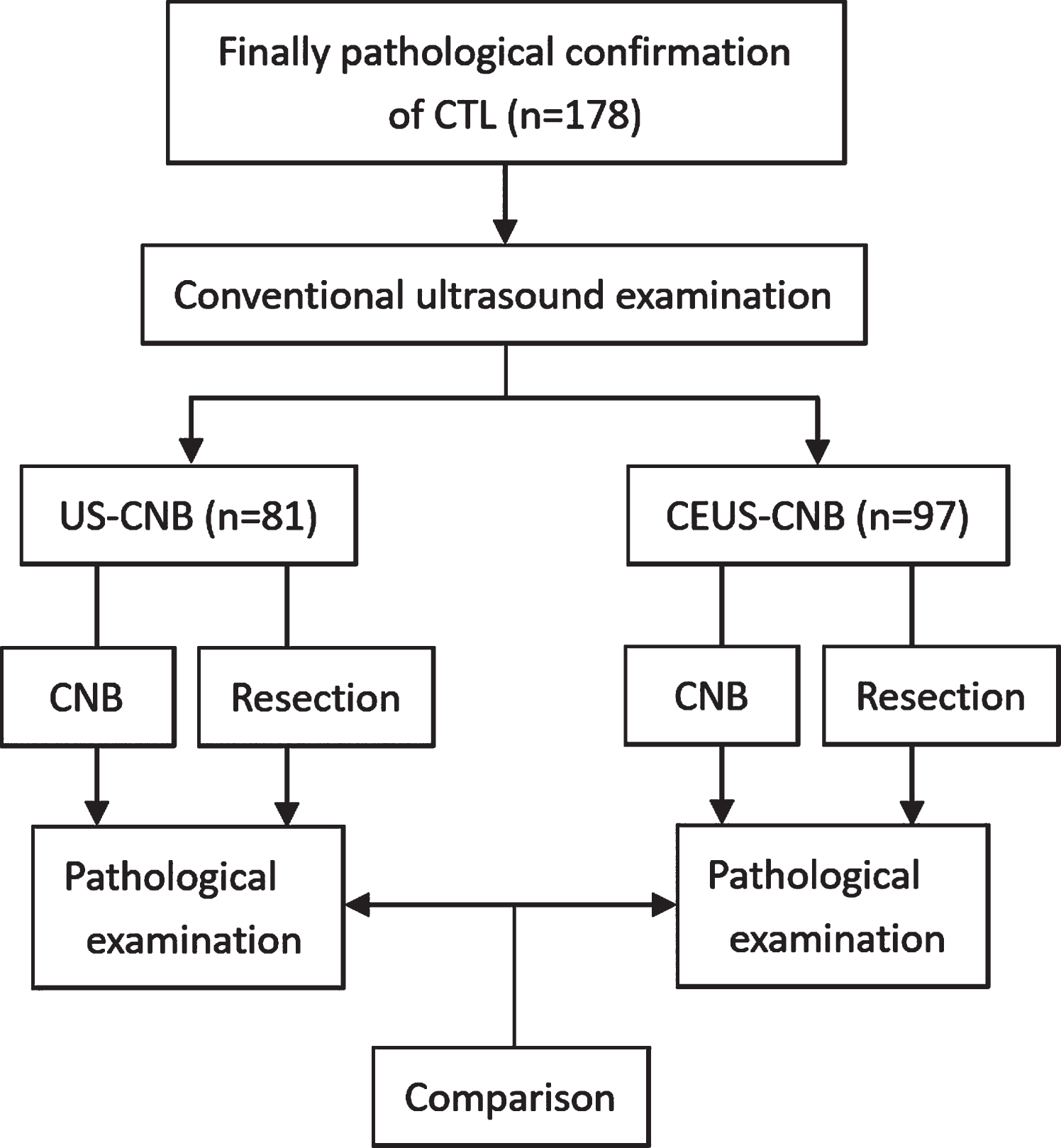
The flowchart.
In the current study, the same Philips IU22 Ultrasound machine (Philips, Amsterdam, the Netherlands) was used for the whole procedure, and a L12-5 linear array transducer (frequency range, 5.0–12.0 MHz) was applied in the conventional US and US-guided CNB. Firstly, with optimized machine setting and sufficient gel applied, high quality images were acquired by a board-certified radiologist in patients’ supine position, including grey scale images and color Doppler images. Both transverse and longitudinal US images for each target lesion were obtained, with maximal diameters of lesions measured on longitudinal plane. Secondly, with target lesion located, an appropriate biopsy path avoiding the main vascular structures was chosen under the color-Doppler US. The biopsy path was also supposed to be the maximum diameter of the lymph node, with necrotic component absent. Thirdly, the biopsy procedure was in an aseptic manner according to the guideline. With focal skin sterilized, local anesthesia using 2% lidocaine was performed. The biopsy was performed by the same prior board-certified radiologist who has more than 10 years of experience in US-guided interventional procedures using an automatic CNB sampling device (Bard, Cavington, USA) in its 18 G type (i.e. the diameter of cutting needle was 1.2 mm, the length of sampling notch was 2.0 cm) within a real-time monitor through conventional US. The tissue specimens were fixed in 10% formalin and then were sent to the department of pathology for histological examination by an experienced pathologist. Routinely, twice punctures were performed for each lesion. All patients were observed for 30 minutes after CNB in case of any complication.
CEUS and CEUS guided CNB
As for the CEUS-guided CNB, while a L9-3 linear array transducer (frequency range, 3.0–9.0 MHz) was applied in the CEUS-guided CNB, a real-time contrast imaging software named pulse inversion harmonic imaging (PIHI) was supported by the Philips Healthcare System, which allows contrast enhanced imaging with low acoustic power (Mechanical Index, MI is 0.06). A dose of 59 mg contrast agent (i.e. SonoVue lyophiled powder, Bracco Diagnostics Inc, Italy) was mixed with 5 ml 0.9% normal saline (NS). The contrast agent is a kind of phospholipid-stabilized microbubbles sized 8μm with an inclusion of sulfur-hexafluoride (SF6), which was disposed by pulmonary circulation. Regular CEUS was firstly carried out. With a dose of 2.4 ml contrast agent injected by a broad-certified nurse, CEUS was displayed on a split-screen mode by optimizing settings. Focus was placed under the level of lesion to minimize the destruction to microbubbles. The duration of CEUS display should be at least 3 minutes. A record of images and videos in the hard disk for further analyses was required for each patient. Immediately after the CEUS of the lesion, the CNB was performed according to the characteristics of the CEUS. Being discriminately addressed from the US-guided CNB, the path for CEUS-guided CNB was principally chosen for enhanced area on CEUS display. And any other procedure instruction in CEUS-guided CNB should be the same as that in US-guided CNB. The CEUS and CEUS-guided CNB were both performed by the same prior radiologist.
Statistical analysis
All statistical analyses were performed by the SPSS Statistics software (SPSS version 19.0; IBM Corporation, Armonk, NY). The continuous data were expressed as mean±standard deviation if they were a normal distribution. Comparisons of continuous variables were performed by independent t test while categorical variables were performed by chi-squared test. A two-tailed P < 0.05 indicated a statistical significance.
Results
The basic characteristics of patients and conventional US signs for target lesions were present in Table 1. No statistical significance was found in lesion size and conventional US characteristics (all P > 0.05).
Demographic distribution and US signs for lesions
Demographic distribution and US signs for lesions
N: number; US: ultrasound; CEUS: contrast enhanced ultrasound; CNB: core needle biopsy; PPD: purified protein derivative.
Among the 178 patients, 146 patients were directly diagnosed as CTL by CNB, including 87 patients in CEUS-guided CNB group and 59 patients in conventional ultrasound guided CNB group, while the rest of 32 patients were failed to be diagnosed by CNB.
In the CEUS-guided CNB group (Fig. 2), a diagnostic efficacy of 89.7% (87/97) was significantly higher than that in US-guided CNB (72.8%, 59/81) (P < 0.05). In subgroup analyses, statistical significance of diagnostic efficacy in CEUS-guided CNB group and US-guided CNB group were found in medium size group and large size group. The former was 91.7% for CEUS-guided CNB vs. 69.0% for US-guided CNB (P < 0.05), the latter was 84.4% for CEUS-guided CNB vs. 57.7% for US-guided CNB (P < 0.05). There was no significance found in small size group (93.1% for CEUS-guided CNB vs. 92.3% for US-guided CNB, P = 0.91) (Table 2, Fig. 3).
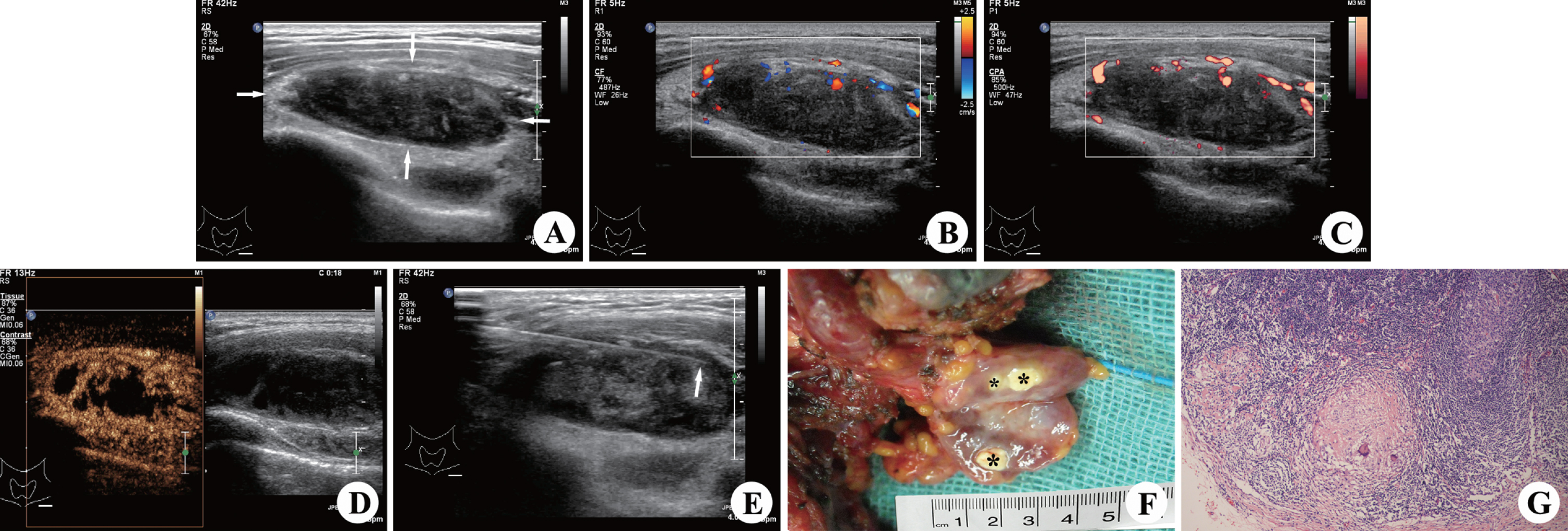
A 32-year-old female patient with cervical tuberculous lymphadenitis. At conventional US, a 3.7*1.2 cm lymph node lesion in region IV at left side neck appears to be heterogeneous hypoechogenicity, infiltrative margin, present of calcification and peripheral vascularity, absence of internal vascularity, (A), (B) and (C). CEUS shows the lesion with annular enhancement around and heterogeneous enhancement inner, and the non-enhancemenet area indicates caseous necrosis in the lesion (D). A puncture is performed after CEUS, avoiding via non-enhancemenet area (E). Macroscopic appearance shows caseous necrosis areas in the lymph node (*), which are corresponding with the non-enhancing areas on CEUS (F). Microscopic examination (×100; H&E stain) shows granulomas with caseous necrosis within the lymph node (G).
Diagnostic accuracy comparison in subgroups
US: ultrasound; CEUS: contrast enhanced ultrasound; CNB: core needle biopsy. * Indicates statistically significant difference. #p < 0.05 when it was compared with small size group.
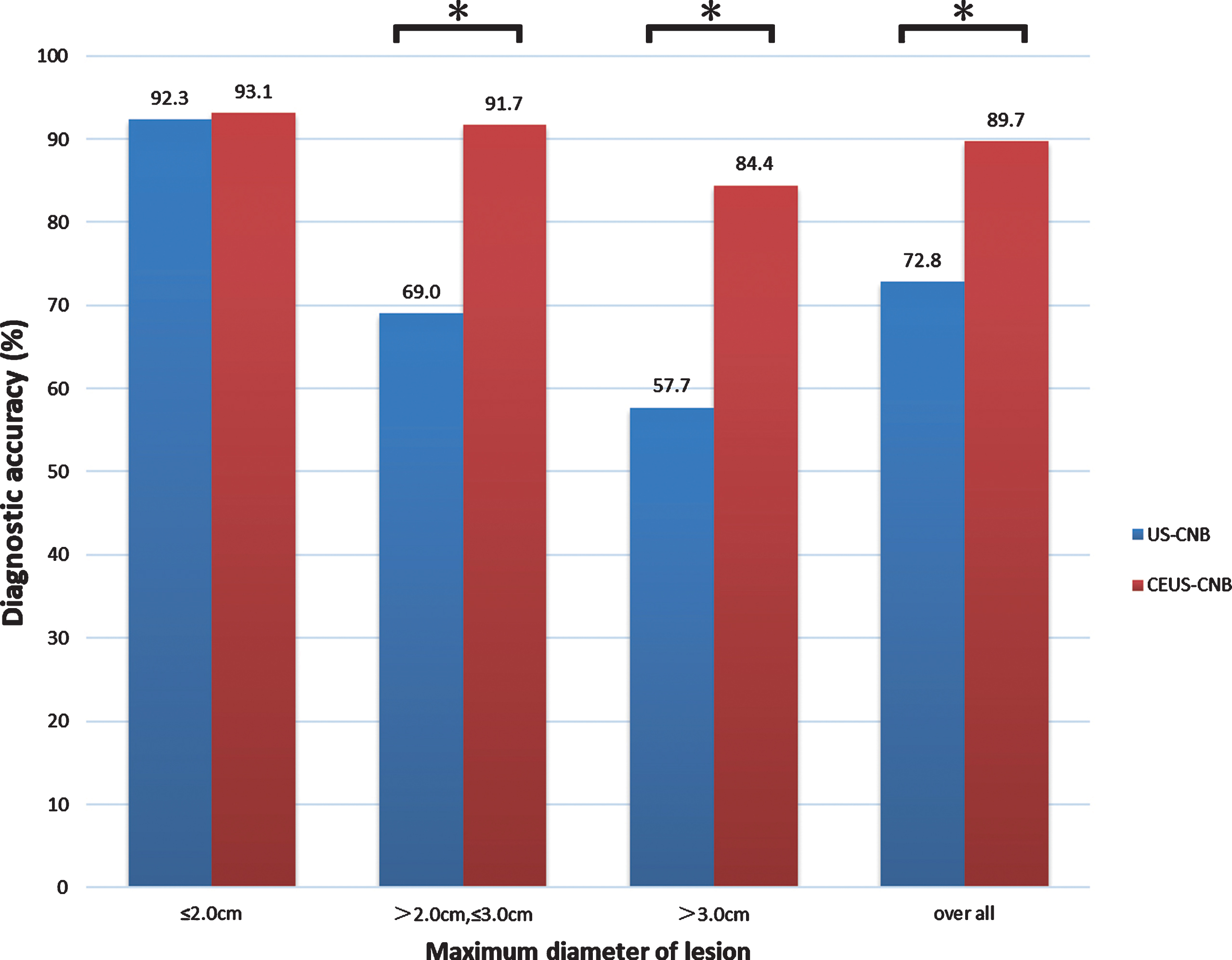
Diagnostic accuracy for conventional US-guided CNB and CEUS-guided CNB according to different lesion size. * Indicates statistically significant difference. US-CNB: conventional ultrasound guided core-needle biopsy; CEUS-CNB: contrast-enhanced ultrasound guided core-needle biopsy. US: ultrasound; CEUS: contrast enhanced ultrasound; CNB: core needle biopsy.
The US-guided CNB group present a diagnostic accuracy of 92.3% (small size group), 69.0% (medium size group) and 57.7% (large size group) with a significant decrease in accordance with the lesion size. In CEUS-guided CNB group, however, no significance was found between any two subgroups (i.e. 93.1% for small size group, 91.7% for medium size group and 84.4% for large size group, all P > 0.05) (Table 2).
CTL was reported to be the most common type of extrapulmonary tuberculosis [2]. In the present study, a female predominance (approximately 2:1) was observed, agreeing with prior study [23]. In initial stage of superficial lymph node involvement, progressive multiplication of the M.tuberculosis occurs. The onset of delayed hypersensitivity is accompanied by marked hyperemia, swelling, necrosis and caseation of the center of the nodes [24]. Their diagnosis and distinction need a high index of suspicion and application of a variety of diagnostic modalities. Because of the poor display on low-speed blood flow, conventional ultrasonography and color Doppler ultrasonography have disadvantages in displaying vascular characteristics of lymph nodes. Although shear-wave elastography guided CNB increased the diagnostic accuracy in breast lesions [25], it may have potential untruthful performance caused by necrosis in CTL. On the other hand, the hilar vascularity of the tuberculous lymph nodes may highly possible be destroyed by the necrosis and caseation, which induces perfusion defects in the CEUS [26]. Comparing with the conventional ultrasonography and color Doppler ultrasonography, low MI CEUS techniques further improved characterization of the lymph nodes [27], and Han reported that the characteristic CEUS image of tuberculous lymph nodes was the glasses-shaped appearance, including large no-enhancement area at the center (indicating caseous necrosis) and peripheral ring-shaped enhancement [28].
As pathological result is referred to be golden diagnosis standard of tuberculous lymphadenitis [29, 30], conventional US-guided CNB has become a promising sampling method thanks to the beneficial features of real-time monitoring, affordable price and non-radiation, despite the important roles CT, MRI and PET CT have played in the diagnosis and treatment for lymphoma [31–33]. In the present study, however, the diagnostic accuracy of US-CNB was hardly more than 72.8% totally. The reasons should be ascribed to the tissue obtained by puncture that was not useful for diagnosis, such as caseous necrosis, which hardly reached to the pathological confirmation.
In the present study, the diagnostic accuracy of CEUS-CNB was 89.7% totally. Furthermore, the accuracy of large lesions stayed above 80%. The underlying reasons were various. Firstly, CEUS was gifted an improved sensitivity in detecting the nonlinear signals produced by the insonation of microbubbles, which enables evaluating the microvasculature. Secondly, CEUS can sensitively detect the active tissue within the lesion through reflecting the regional microvascular. Highly enhanced area is supposed to be active tissue while non-enhancement area is supposed to be necrotic area. With the information CEUS indicated, active tissue could be directly located, and necrotic areas could be efficiently avoided. Therefore, in the recent years, CEUS has becoming a promising application not only for diagnosis, but also for guidance [16, 34–37].
Concerning the subgroup analyses in terms of lesion size, static significances regarding the different guiding methods were found in medium and large size group. However, no static significance was found within the small size group. Obviously, CEUS-guided CNB performed more efficiently in those lesions which was larger than 2.0 cm. Furthermore, there was a stable and moderate diagnostic efficacy in terms of sensitivity among all three groups, while conventional US-guided CNB showed a significant decrease of sensitives accompanying with the growth of lesion size. There are two underlying reasons being explained for what the present results. Firstly, the sampling length of needle (i.e. 2.0 cm) should be noticed. When the lesion size was larger than the sample length, the overall assessment of CEUS has showed a better efficacy in biopsy navigation than conventional US. Secondly, lesions smaller than 2.0 cm may stay in an early stage of the disease progress, and the active tissue within lesion may be in dominance. Thus, the likelihoods of obtaining active tissue were similar whatever the guiding method was applied.
Surely, there were several limitations in this study. First, the study was set to be retrospective, which may results in some biases in case selecting. Second, sample size of current study was relatively small, so further research needs a larger sample size. Third, limited assessment was made due to the lack of other medical imaging, such as CT or MRI. Forth, some emerging laboratorial techniques, such as Xpert MTB/RIF, were not assessed in the present study. Fifth, intra-observer consistency was not assessed, which may lead to the unclear retribution. Sixth, some novel/emerging transducer and technology such as eL18-4 ultra-broadband linear array with PureWave crystal technology were not used and studied, which may have a potential of batter performance in CTL.
Conclusions
In conclusion, CEUS is a more advanced guiding method for CTL lesions than traditional US-guided CNB, especially for lesions larger than 2.0 cm.
Conflicts of interest
All the authors certify that there is no actual or potential conflict of interests in this article.
Footnotes
Acknowledgments
This study was supported by grant LGF20H180003 from Basic public welfare research program of Zhejiang Province, and grant 2019KY511 from Zhejiang medical and health science and technology project.