
Abstract
OBJECTIVES:
To present a method combining ultrasound (US) and contrast-enhanced ultrasound (CEUS) features for differential diagnosis of cervical tuberculous lymphadenitis (CTL) and primary lymphoma.
METHODS:
A total of 155 patients with CTL (n = 49) and lymphoma (n = 106) who underwent US and CEUS were retrospectively included. The features extracted from US and CEUS and the significant clinical data were created three models using the least absolute shrinkage and selection operator and logistic regression analysis. The diagnostic performance of the models was assessed using the area under the curve (AUC).
RESULTS:
The combined model outperformed US model and CEUS model in distinguish CTL from lymphoma achieved favorable performances in training set and validation set with AUCs of 0.958 and 0.946 as well as high accuracies (91.7% and 87.2%), sensitivities (95.9% and 84.4%) and specificities (82.4% and 93.3%). Delong’s test showed that among the three models, combined model was significantly different from the other two models in training set (p = 0.011 and 0.029, respectively) and validation set (p = 0.018 and 0.001, respectively).
CONCLUSIONS:
A combination of US and CEUS achieved good diagnostic performance in differentiating lymphoma and CTL, which might aid in clinical decision-making.
Introduction
Patients with lymphoma and cervical tuberculous lymphadenitis (CTL) often present with palpable neck lymph nodes (LNs). Studies have shown that lymphomas have imaging characteristics similar to those of nonmalignant LNs [1, 2]. CTL is the most common extrapulmonary manifestation of disseminated pulmonary tuberculosis [3], and clinical studies have documented that cervical node involvement predominates in more than two-thirds of patients with tuberculosis adenitis [4, 5]. Excisional biopsy is considered highly sensitive for diagnosing CTL, however, this method is invasive.
Ultrasound (US) has been widely used in the diagnosis of superficial LNs, which characterizes the morphology and internal structure of LNs and the distribution of vascularity within the LNs. One research showed that concordant results in PET/CT and US were found in 83% of patients with nodal findings [6]. However, a routine PET-based diagnosis may not be achievable for all head and neck disease as PET resources may be limited, while the advantages of US diagnostics are the quick implementation, real time, low costs, lack of radiation exposure and the possibility of direct interventional biopsy [7]. US features of CTL, such as poorly defined anechoic areas with or without sinus, have high sensitivity and negative predictive values but low specificity [8]. US appearance of lymphoma is more variable, partially overlapping with inflammatory, reactive and metastatic LNs, and atypical manifestations complicate differentiation [9]. The US features of CTL overlap with those of lymphoma and usually exhibit heterogeneous echogenicity, making the differential diagnosis difficult using US. Therefore, the ability of US to differentiate between lymphomas and CTL may sometimes be challenging in daily clinical practice.
Contrast-enhanced ultrasound (CEUS) provides real-time visualization of the microvascular status and blood supply to LNs [10, 11]. An analysis of LN perfusion after an intravenous injection of microbubble contrast media is helpful in assessing the nodal internal structure and identifying avascular areas to detect necrosis and tumor deposits [12, 13]. To date, multiple studies have shown that CEUS has better performance in diagnosing benign cervical lymphadenopathy and tumor LN metastases, with higher accuracy than conventional US [14–16]. Studies have also reported the application of CEUS in the differential diagnosis of cervical lymphoma and malignant cervical LN cancer [15] or cervical LN metastasis and CTL [17]. However, the value of CEUS in distinguishing CTL from primary lymphoma has never been discussed. We propose that establishing specific imaging criteria to distinguish CTL from lymphoma will be valuable for the accurate diagnosis of the disease.
In this study, we hypothesized that CEUS would distinguish CTL from primary lymphoma based on differences in vascularity and internal structure. We aimed to establish a method utilizing US and CEUS to evaluate the diagnostic performance between CTL and lymphoma.
Materials and methods
Patients
This retrospective single-center study was approved by the institutional review board of our hospital (No. SQ2016-049-01), and informed consent was waived. The inclusion criteria were as follows: i) patients with a histopathological diagnosis of CTL or lymphoma, ii) aged 18-80 years, and iii) pretreatment involving US and CEUS examinations. The following patients were excluded: i) pediatric patients and pregnant or lactating women, ii) patients who had a severe allergic reaction, and iii) patients who underwent tumor surgery, chemotherapy, or radiotherapy.
US examination
Patients with hyperextended necks underwent a conventional US examination with 5-12 MHz linear phased-array transducers (iU-22 or iU-Elite; Philips Medical Systems). Clinical data were reviewed, including age, sex and type of lesions. The cervical LNs were then scanned. The ultrasound features, including long and short diameter, short axis/long axis ratio (S/L ratio), vessel(s) entering nodule(s), peripheral hyperechogenicity, shape, LN distribution, homogenicity, calcification, cystic changes, grid hyperechogenicity, hilum, echogenicity, vascularity and border of the largest slice LNs, were recorded [18, 19].
CEUS examination
CEUS imaging was performed using an L9-3 linear array transducer (iU-22 or iU-Elite; Philips Healthcare, USA) by three ultrasound specialists with at least 6 years of experience in the field. SonoVue (Bracco, Milan, Italy) was added to 5 ml of a 0.9% NaCl solution and shaken thoroughly to obtain a suspension of the contrast agent before the examination. Boluses of contrast agent were injected manually at a dose of 2.4 ml, followed by a flush with 5 ml of a saline solution. During the CEUS procedure, the timer was started on the US machine, and whole images (2 min) were digitally stored as raw data for the analysis. The region of the lesion and the surrounding normal tissue were included in the selected plane. After the examination was completed, two head-and-neck radiologists played the video back to observe and record the enhancement patterns of the LNs.
The CEUS features of the LNs were analyzed offline. The enhancement direction was classified as centripetal, centrifugal, or chaotic. Centripetal perfusion enhancement was defined as contrast agent filling from the periphery to the center. Centrifugal perfusion referred to divergent perfusion from one point due to centrifugation. Chaos perfusion enhancement was defined as the inability to determine the direction of enhancement. Compared with adjacent tissues around the LN region at peak enhancement, the degree of enhancement was divided into hype-enhancement, hypoenhancement, isoenhancement, and nonenhancement. The enhancement type was classified into 4 types [2, 13]: homogeneous, spotty, separated-like, and rim-like. Homogeneous enhancement is defined in the early arterial phase, showing a snow-like, dotted pattern that merges into bright spots that eventually form homogeneous enhancement in the late phase without perfusion defects. Spotty enhancement is defined in the early arterial phase and shows a snow-like, dotted pattern that merges into bright spots that eventually form heterogeneous enhancement in the late phase, with small perfusion defects. Separation-like enhancement indicates that the interior appears as honeycomb or compartment-like perfusion defects. Rim-like enhancement is defined as borderline or peripheral enhancement, with the most central perfusion defects. The nonenhanced area referred to the absence of contrast agent perfusion in the LNs at all times. The border and degree of the nonenhanced area were assessed in a slice that showed the largest nonenhanced area.
The degree of the nonenhanced area was categorized with a simple visual scoring system as follows [20]: 0, no perfusion defects; 1, the area of perfusion defects is < 1/4 of the whole area of the representative LN; 2, area of perfusion defects≥1/4 and < 2/4; 3, area of perfusion defects≥2/4 and < 3/4; and 4, area of perfusion defects≥3/4. We performed simple visual scoring of the nonenhanced area instead of quantifying the data because an intuitive estimation rather than counting is performed in practice. CEUS enhancement patterns were determined by two radiologists who were blinded to pathological findings and had 12 and 15 years of experience in diagnosing LN diseases. The two radiologists independently diagnosed and analyzed the data and then discussed the results to achieve a consensus.
US-guided core needle biopsy and polymerase chain reaction
The nodal US-core needle biopsy (CNB) was performed immediately after US and CEUS examination by two experienced radiologists (with 10 and 20 years of neck imaging experience, respectively) on the representative LN using a disposable 16-gauge gun biopsy needle (Stericut with a coaxial guide, TSK Stericut; TSK Laboratory, Soja, Japan). The cortex of the LN was obtained after local anesthesia with 1% lidocaine. After CNB, each sample was mounted onto a glass slide immediately. Specimens were fixed in 95% ethanol and sent for cytologic analysis, while remaining puncture specimens were used for pathological diagnosis or polymerase chain reaction (PCR) examination. PCR examination was performed by electrochemical luminescence immunoassay using the Elecsys automated system (Roche, Mannheim, Germany). Samples with abnormal PCR titers were considered tuberculosis positive.
Construction of the diagnostic models
Each disease group was stratified by random sampling into the training set (70%) and the validation set (30%) to assess the diagnostic performance of the models. The least absolute shrinkage and selection operator (LASSO) and logistic regression analyses were used to create three models for the differential diagnosis of CTL and lymphoma. LASSO algorithm has built-in cross validation technology, which can further enhance the stability of features when it is applied to feature screening. LASSO methods coded 0 for CTL and 1 for lymphoma. First, the US features and clinical data were used by LASSO algorithm and 11 features were selected, then logistic regression was used to establish the US model. Similarly, the CEUS features and clinical information were used and 8 features were used to obtain the CEUS model. Next, the US and CEUS features and their weighted coefficients were filtered out and integrated by the LASSO algorithm to form the US score and the CEUS score, respectively. Finally, the combination of US score, CEUS score and clinical data was used for further feature screening with the LASSO algorithm, and 5 features (sex, age, type of lesions, US score and CEUS score) were obtained to build the combined model. Additionally, to translate the diagnostic value of combined model into clinical application, a combined model nomogram, including the clinical data, US score and CEUS score of patients evaluated by using logistic regression analysis, was developed for differential diagnostic the two diseases.
Statistical analysis
Statistical analyses were performed using R software (version 4.0.3, https://www.r-project.org/) and the SPSS statistical package (23.0, Chicago, IL, USA). Statistical analyses were performed using pathological results as the reference standard. Clinical data, US and CEUS features were compared between the two groups. Pearson’s chi-square test or Fisher’s exact test was used to compare the differences in categorical variables. The t test or Mann—Whitney U test was used to analyze the numerical variables according to its normality. The diagnostic performance of the models was assessed by using receiver operating characteristic (ROC) curve analysis, in which the areas under the curve (AUCs), accuracies, sensitivities, and specificities were established, and differences between models were assessed using DeLong’s test. R software was used for the LASSO method and logistic regression analysis to build models by using the R packages named “glmnet”, “pROC” and “rms”. In all cases, two-sided P values less than 0.05 were considered statistically significant.
Results
Patients
From January 2020 to December 2022, a keyword search was performed to identify patients with histopathologically confirmed lymphoma or granulomatous lymphadenitis who underwent US-CNB for cervical lymphadenopathy at our hospital. Patients with no CEUS examinations (n = 47), poor image quality (n = 6), and no immunohistochemical or PCR examination results (n = 22) were excluded. Using the machine learning method and random stratified sampling method, patients were divided into the training set (70%, 108/155) and the validation set (30%, 47/155). The flowchart for patient inclusion and exclusion is shown in Fig. 1.

Flowchart overview of patient inclusion and exclusion. US-CNB, ultrasound-guided core needle biopsy; CEUS, contrast-enhanced ultrasound; PCR, polymerase chain reaction; HD, Hodgkin.
Forty-nine patients with CTL (26 males and 23 females, 50.49±12.90 years) were investigated. The maximum diameter of the mass ranged from 7 to 57 mm, with an average diameter of 21.27±9.90 mm. The final diagnosis was based on a histological biopsy of CTL using US-CNB and a positive tuberculosis PCR test.
One hundred and six untreated patients with lymphoma (65 males and 41 females; 57.09±14.19 years) were investigated. The maximum diameter of the mass ranged from 12 to 120 mm, with an average diameter of 35.94±18.20 mm. Nine patients had Hodgkin lymphoma, and 97 had non-Hodgkin lymphoma. Lymphoma was diagnosed based on histological findings on US-CNB.
The US diagnostic features of both groups are summarized in Table 1. In this study, the two groups showed differences in age (p = 0.006), while a statistically significant difference in sex was not observed between the two groups. US showed significant differences between the two groups in the maximum and short diameter, type of lesions, peripheral hyperechogenicity, cystic changes, grid hyperechogenicity, hilum and vascularity (p < 0.05). Lymphoma typically was associated with grid hyperechogenicity in 68.9% of patients in the lymphoma group compared with only 18.2% of the patients in the CTL group (p = 0.000). Lymphomas presented primarily with mixed vascularity (46.2%), whereas CTL primarily presented with a peripheral (59.2%) structure or an avascular (32.7%) structure. The long and short diameters were significantly longer in the lymphoma group (mean values of 35.94±18.20 mm and 20.73±10.20 mm, respectively) than in the patients with CTL (mean values of 21.27±9.90 mm and 11.65±5.06 mm, respectively) (p = 0.000). Lymphoma appeared as multiple nodules in 98.1% of patients compared to the detection of solitary nodules in 16.3% of patients with CTL (p = 0.002). Lymphoma with hilum was observed in 17.9% of patients, but this feature was only detected in 2.0% of patients with CTL (p = 0.006). Peripheral hyperechogenicity and cystic changes were significantly more frequent in patients with CTL than in patients with lymphoma (p = 0.000).
Clinical data and US features in patients with CTL and lymphoma
Clinical data and US features in patients with CTL and lymphoma
US: ultrasound, CTL: cervical tuberculous lymphadenitis, LN: lymph node.
Table 2 lists several significant differences in CEUS features between the two groups. The data showed that 55.7% of the cases characterized by spotty enhancement were in the lymphoma group, while 65.3% of the cases with rim-like enhancement were in the CTL group (P = 0.000) (Fig. 2). Regarding the direction of enhancement, lymphoma typically appeared as chaotic enhancement in 81.1% of patients (Fig. 3 a-b); however, CTL usually showed centripetal enhancement in 87.7% of patients (Fig. 3 c-d) (P = 0.000). Regarding the enhancement degree, lymphomas mainly exhibited hyperenhancement (94.3%), while CTL was diverse, with approximately half of cases showing hyperenhancement (46.9%) (P = 0.000). Most of the patients in the two groups had nonenhanced areas. Notably, a well-defined border of nonenhancement was observed in 80.0% of the patients with CTL, while an ill-defined border was observed in 84.0% of the patients with lymphoma (P = 0.000). A score of 1 for the nonenhanced area was recorded for 50.9% of the patients with lymphoma, on the other hand, a score of 4 was recorded for the nonenhanced area in 49.0% of patients with CTL (P = 0.000).
Comparison of CEUS features of CTL and lymphoma
Comparison of CEUS features of CTL and lymphoma
Enhancement type: homogeneous enhancement is defined in the early arterial phase and shows a snow-like, dotted pattern that merges into bright spots that eventually form homogeneous enhancement in the late phase without perfusion defects. Spotty enhancement is defined in the early arterial phase and shows a snow-like, dotted pattern that merges into bright spots that eventually form heterogeneous enhancement in the late phase, with small perfusion defects. Separation-like enhancement indicates that the interior appears as honeycomb or compartment-like perfusion defects. Rim-like enhancement is defined as borderline or peripheral enhancement, generally appearing as central perfusion defects. Degree of nonenhanced area (visual scoring): 0, no perfusion defects; 1, the area of perfusion defects is < 1/4 of the whole area of the representative LN; 2, area of perfusion defects≥1/4 and < 2/4; 3, area of perfusion defects≥2/4 and < 3/4; and 4, area of perfusion defects≥3/4. CEUS: contrast-enhanced ultrasound, CTL: cervical tuberculous lymphadenitis, LN: lymph node.

Images present the general appearance of CTL and lymphoma based on CEUS imaging patterns. Homogeneous enhancement is defined in the early arterial phase and shows a snow-like, dotted pattern that merges into bright spots that eventually form homogeneous enhancement in the late phase without perfusion defects (
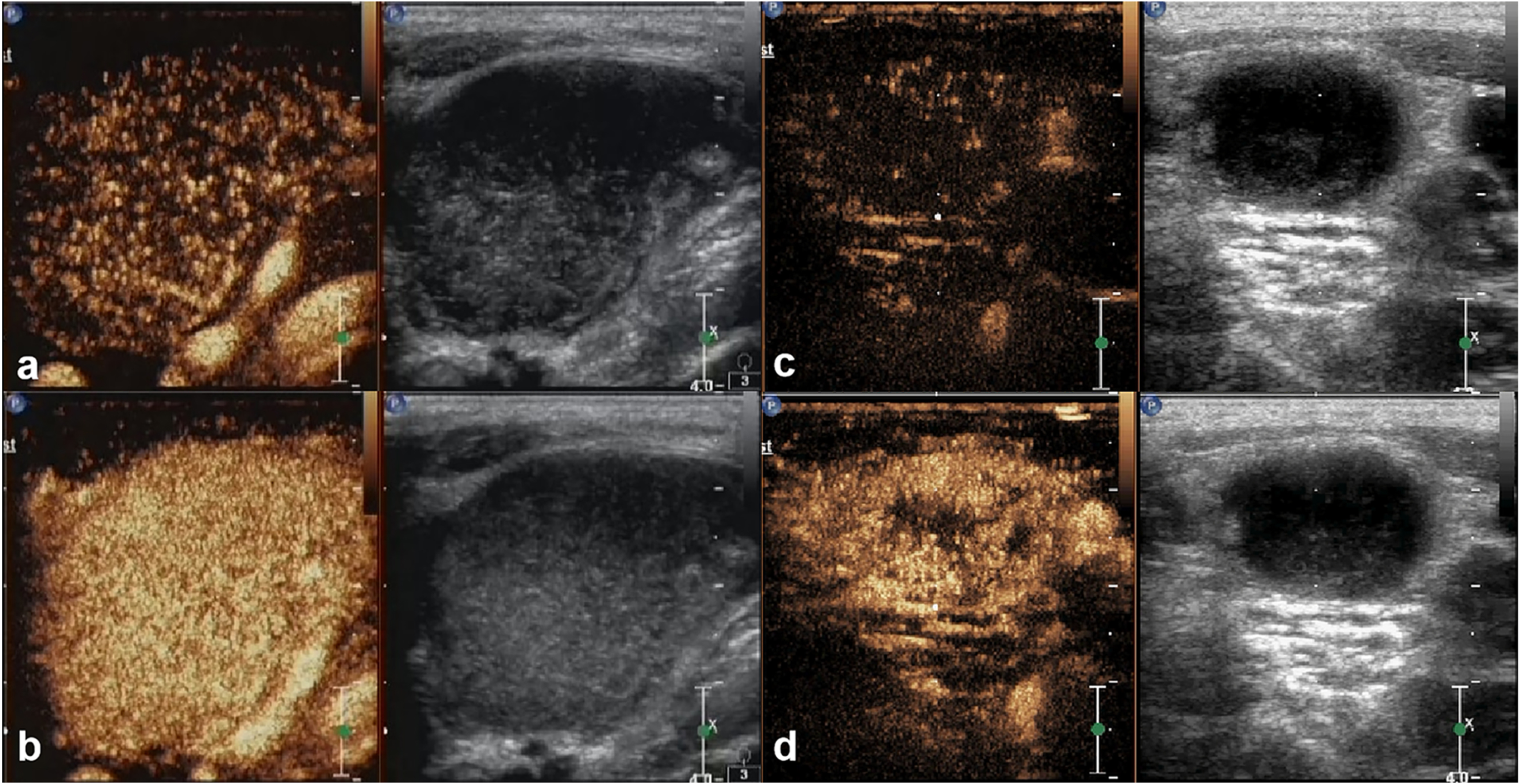
Table 3 shows the selected features and their corresponding coefficients in US and CEUS score by LASSO and logistic regression analyses. Positive values are associated with lymphoma and negative values are associated with CTL. For features of US score, the short diameter (0.123), oval shape (0.305), sharp border (0.707), grid hyperechogenicity (0.846), mixed (1.334) and hilar (0.446) vascularity were associated with lymphoma, while cystic changes (-0.776), calcification (-0.466), peripheral vascularity (-0.836), and peripheral hyperechogenicity (-0.189) were associated with CTL. Regarding features of CEUS score, hyperenhancement (1.091) and an ill-defined border of the nonenhanced area (0.214) were associated with lymphoma, while centripetal enhancement (-1.970) and the degree of the nonenhanced area (-0.628) were associated with CTL. As shown in Table 4 and Fig. 4, the combined model and nomogram including the US score, CEUS score and 3 selected clinical data were developed, and the CEUS score outperformed the US score according to the coefficients and nomogram.
The selected features and their corresponding coefficients in US score and CEUS score
The selected features and their corresponding coefficients in US score and CEUS score
US score: ultrasound score, CEUS score: contrast-enhanced ultrasound score.
The selected features and their corresponding coefficients in combined model
US score: ultrasound score, CEUS score: contrast-enhanced ultrasound score.
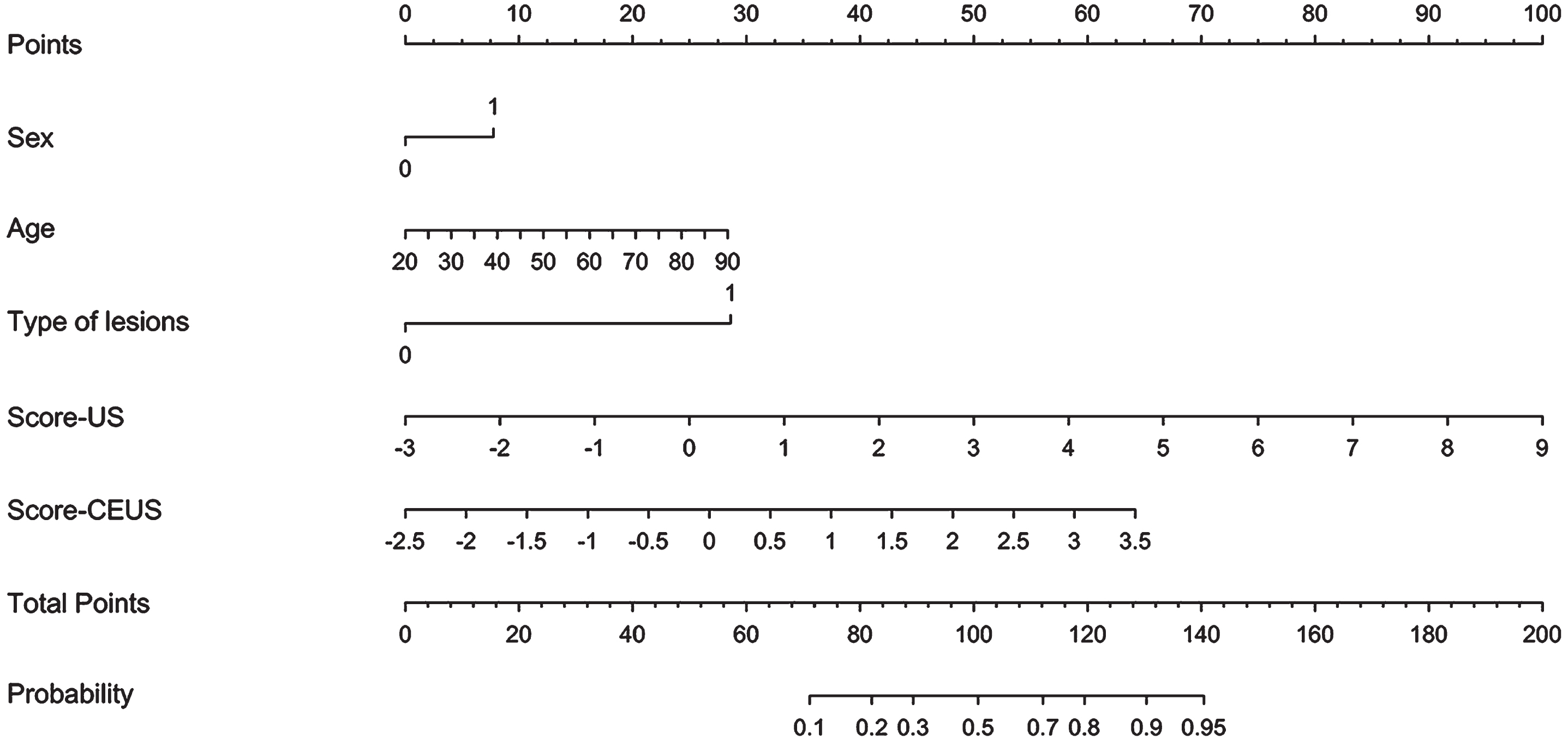
A nomogram based on the US score, CEUS score and clinical data.
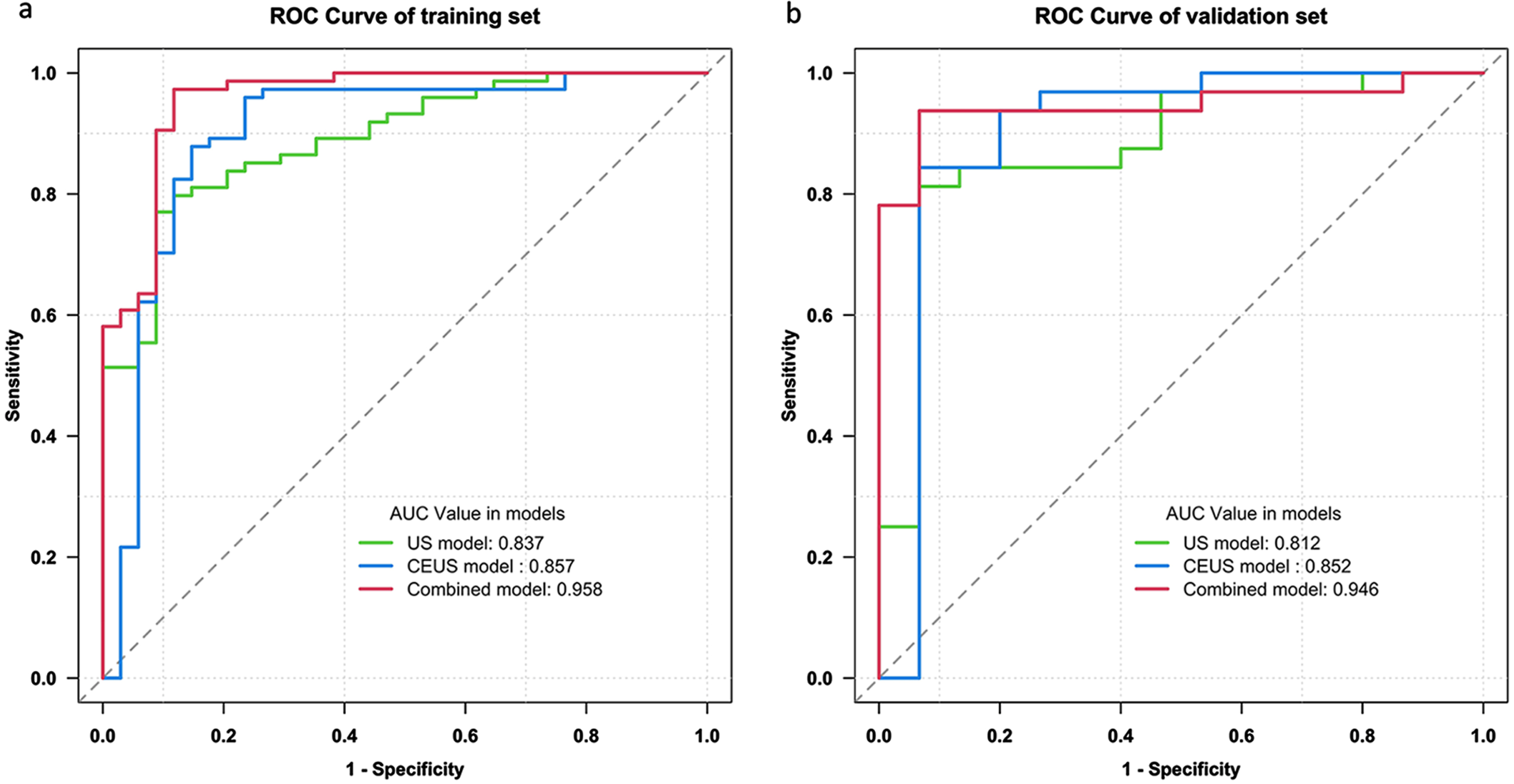
The diagnostic performance of three models in differentiating lymphoma and CTL in the training set and the validation set are shown in Table 5 and Fig. 5. For the US model, the accuracies were 77.8% and 74.5% in the training set and validation set and an AUC of 0.837 was observed for the training set and 0.812 for the validation set. For the CEUS model, the accuracies were 85.2% and 74.5% in the training set and validation set, respectively, and yielded an AUC of 0.857 for the training set and 0.852 in the validation set. The combined model achieved excellent diagnostic efficacy (accuracies, 91.7% and 87.2%; sensitivities, 95.9% and 84.4%; specificities, 82.4% and 93.3%; AUCs, 0.958 and 0.946) in the training set and validation set compared to the US model or the CEUS model.
Models performance for differentiating lymphoma and CTL
① ∼Clinical data, ② US features, ③ CEUS features, US model=① +②, CEUS model=① +③, Combined model=① +② +③. US: ultrasound, CEUS: contrast-enhanced ultrasound, CTL: cervical tuberculous lymphadenitis, AUC, area under the curve.
As shown in Table 6, compared with the US model and the CEUS model, the combined model had better differential diagnostic ability in both the training set (p = 0.011 and 0.029, respectively) and validation set (p = 0.018 and 0.001, respectively), while no difference was observed between the US model and CEUS model in the training set (p = 0.586) and validation set (p = 0.217).
Comparison of the US model, the CEUS model and the combined model
US: ultrasound, CEUS: contrast-enhanced ultrasound.
In this study, we found that grid hyperechogenicity, vascularity, cystic changes, enhancement direction, the degree of enhancement and the degree of non-enhancement areas were significant predictors for the differential diagnosis of CTL and lymphoma. The combined model showed more reliable differential diagnostic ability (accuracy, 91.7% and 87.2%; sensitivity, 95.9% and 84.4%; specificity, 82.4% and 93.3%; AUC, 0.958 and 0.946) than the US model and the CEUS model in the training set and the validation set.
The presence of grid hyperechogenicity on US was an important predictor to differentiate CTL from lymphoma in the present study. The internal echo pattern of lymphoma is characterized by a heterogeneous echo pattern of both the cortex and medulla, resulting in overall grid hyperechogenicity [21]. As this grid hyperechogenicity is not observed in most cases of CTL, it appears to be a useful feature in identifying lymphoma. Vascularity patterns and their changes were useful features for differentiating lymphoma from CTL, lymphoma presented with mixed vascularity (46.2%), while CTL predominantly presented with peripheral vascularity (59.2%). These results for CTL and lymphoma are consistent with previous studies [15, 17]. This was likely due to the destruction of the normal vascular structure when caseous necrosis occurs inside the CTL, thus resulting in insufficient blood supply to the central LN area, but the intact LN margins are rich in new capillaries; however, in most lymphomas, the blood vessels are highly hyperplastic, which makes the distribution of blood flow more abundant. Similarly, a cystic change is a specific feature of CTL, and the general mechanism of cystic changes in CTL is a destruction of the normal vascular structure of the LNs by Mycobacterium tuberculosis, leading to caseous necrosis. In contrast, a cystic change is also rarely observed in lymphoma, a heterogeneous group of neoplastic diseases that arise from a single mutated lymph node cell but most occur after chemotherapy [22].
Recent studies showed that conventional US with the help of CEUS can improve diagnostic accuracy in many areas of otolaryngology [7, 23]. For CEUS features in our study, centripetal enhancement was a key factor in CTL that may help distinguish it from lymphoma. Most CTL lesions had a centripetal enhancement pattern (87.8%), and most lymphomas had a chaotic enhancement pattern (81.1%). Pathologically, as reported in previous studies [8, 13], this phenomenon might be associated with the formation of granulomas in the marginal area of CTL, which can cause telangiectasia and results in the initial formation of a pattern of the contrast agent dominated by centripetal enhancement in the LN border area, whereas in most lymphomas, extensive blood vessels are observed that allow the contrast agent to easily flow, however, the enhancement direction of the entire nodule is not easy to determine, and most show chaotic enhancement. The enhancement degree, which is an important factor in lymphoma, can help distinguish it from CTL. In our study, we documented homogeneous hyperenhancement of most lymphomas (94.3%). The same enhancement pattern was reported by Slaisova et al [12]. This finding may be related to the observation of more abnormal arteries in lymphomas.
We distinguished two diseases by dividing the four enhancement types in this study, which were screened as predictors in the CEUS model. CTL predominantly shows rim-like enhancement (65.3%), and appeared as more perfusion defect areas than lymphoma, 73.5% had a necrosis score of 3 or 4, in contrast, only 5.7% of patients with lymphomas showed the same degree of necrosis. Correspondingly, A potential explanation for this result is that extensive caseous necrosis caused by Mycobacterium-mediated tissue destruction promotes the necrosis of most LNs in patients with CTL. However, 6 patients with CTL still presented with spotty or homogeneous enhancement and 13 patients presented with a degree of necrosis of less than half. This result may be related to the pathological changes in patients with CTL. According to a previous report [24], active CTL pathologically progresses through four stages according to the duration of the disease, and necrosis is detected at the necrotizing stage. Not all LNs are at the same stage, and only a small number of LNs are in the lymphoid hyperplasia stage with no or only a small amount of caseous necrosis. In addition, intranodular necrosis or cysts are only occasionally discovered in untreated lymphomas with a large diameter [25]. Previous studies have suggested that lymphoma showed a speckled enhancement in the early arterial phase, resembling a snow-like appearance with diffuse bright spots [26] and subsequent widespread homogeneous enhancement in the late phase [9, 12]. Slaisova et al [12] considered that 88.3% of lymphomas were the intense homogeneous enhancement type. In this study, homogeneous and spotty enhancement accounted for 29.2% and 55.7% of cases, respectively, which is consistent with previous studies. This result may be related to the presence of many abnormal arterioles within lymphomas, a phenomenon reported only for lymphomas in the literature [27] and suggested to be helpful in distinguishing other lymphadenopathies, which further corroborates the findings in our reports.
In this study, this 5 features, including 3 clinical information, US score and CEUS score, selected to build the combined model performed well not only in training set but also in validation set, with AUCs of 0.958 and 0.946, respectively. The high accuracies, sensitivities and specificities with 91.7%, 95.9% and 82.4% in the training set as well as 87.2%, 84.4% and 93.3% in the validation set were observed. Patients with CTL were younger and predominantly female compared with patients with lymphoma, consistent with a previous report [4]. We identified an additional feature that was helpful to distinguish CTL from lymphoma, namely, the distribution of the nodules. Lymphoma usually presents as multiple nodules, while CTL typically manifests as solitary nodules. Therefore, US and CEUS features combined with clinical data would be useful for the differential diagnosis and may improve the diagnostic accuracy. In addition, we further transformed the combined nomogram into a visual diagnostic tool, which could easily be used for rapid differential diagnosis of CLT and lymphoma. Notably, in the combined model, we obtained the US score and CEUS score to quantitatively evaluate the role of US and CEUS features, in order to find out which feature has higher value for the final diagnosis among clinical features, US features, and CEUS features. It is not difficult to see from the nomogram that the CEUS score outperformed the US score, CEUS features need to be paid more attention to when identifying the two groups of diseases in the clinical auxiliary diagnosis.
Our study had some limitations. First, this retrospective study included a limited study population, and the establishment, training and validation of the diagnostic models for the two diseases were based on only data from a single tertiary hospital. Second, patients did not have available results from serological examinations or other clinical manifestations, such fever and neck pain. Third, we did not use quantitative CEUS parameters for the differential diagnosis of the two diseases. Finally, other causes of cervical lymphadenopathies were not included in the diagnostic models.
In conclusion, the combined model based on US and CEUS features and basic clinical information showed a high accuracy for discriminating CTL and lymphoma. This model may be helpful for clinical decision-making.
Footnotes
Acknowledgment
This work was supported by Fujian provincial health technology project (No. 2021TG017), National Clinical Key Specialty Construction Program of China [No. (2013)544].