
Abstract
OBJECTIVE:
To assess iliac blood vessels using conventional ultrasound (US) and contrast-enhanced ultrasonography (CEUS) before kidney transplantation (KT) and determine whether US findings related to post-transplant outcomes.
METHODS:
A total of 119 patients received US and CEUS before KT waiting-list acceptance. The preoperative iliac blood hemodynamics and vascular conditions were evaluated. The operative strategy and follow-up outcomes were recorded. Logistic regression and correlation analysis were used. The accuracy in determining the patency of iliac blood vessels was calculated before and after the injection of contrast materials.
RESULTS:
CEUS can help to significantly improve the visualization of the internal iliac artery, but there was no significant correlation with post-transplant outcomes. In terms of accuracy, there were significant differences in determining the patency of internal iliac arteries between conventional US and CEUS (60.5% and 100%, p < 0.001). The surgical strategy of one patient was regulated and two patients were excluded from KT according to US findings.
CONCLUSIONS:
Compared with conventional US, CEUS helps to improve the visualization of the internal iliac artery. Conventional US and CEUS have the potential to serve as effective methods to evaluate anatomy and hemodynamics of iliac vessels and have a potential value while defining clinical algorithms in surgery decision-making.
Introduction
Kidney transplantation (KT) remains the best available therapeutic option for many end-stage renal diseases (ESRD) [1]. In patients with KT, the diameter, hemodynamic changes, and patency of iliac vessels are important factors affecting the surgical success. Therefore, an assessment of transplant candidates must include an accurate evaluation of vascular anatomy and blood flow status. Imaging techniques can be used to assess changes of arterial and venous vasculature, thus, to determine: if KT is a viable option, if preoperative procedures are essential, and which is the best surgical scheme for each patient on the waiting list.
Different imaging modalities, such as computed tomography angiography (CTA) and magnetic resonance angiography (MRA), are used in the identification of vascular conditions. However, these modalities cannot provide dynamic assessment and measurement of vascular flow. Vascular assessment requires intravenous injection of contrast agents: these materials could generate nephrotoxicity in patients with renal insufficiency [2, 3]. Previous studies have confirmed that the use of gadolinium-based contrast material in MRA can cause nephrogenic systemic fibrosis in patients with severe kidney disease [4–6].
Conventional ultrasound (US), including grey-scale US and Doppler US, remains a cost-effective, readily available imaging modality for preoperative assessment of iliac blood vessels and postoperative follow-up [7–9]. Although Doppler US was used in assessing the vascular status before KT, evidence from a recent study shows that US could not visualize the internal iliac artery in 69% of cases [10].
Contrast-enhanced ultrasonography (CEUS) can improve the visualization of blood vessels. Recent research shows that CEUS has greatly improved the diagnostic performance of US in assessing vascular patency [11, 12]. This can potentially prove to be a relatively safe imaging modality for patients with renal dysfunction. CEUS may have a much higher sensitivity and specificity, which can prove to be more useful in assessing microvascular perfusion of graft kidneys [13, 14]. To our knowledge, no prior studies have examined the hemodynamics of iliac blood vessels using CEUS in patients waiting to be placed on a waiting list for KT. We hypothesized that the use of CEUS can improve the visualization of the internal iliac artery in patients who are ready to receive KT.
In this study, we aim to assess iliac blood vessels before KT, and determine whether US findings are related to post-transplant outcomes.
Materials and methods
Patients’ clinical characteristics
Between March 2018 and March 2019, a total of 441 ESRD patients (>18 y.o.) received US examination before KT waiting-list acceptance. 120 patients out of 441 received KT between March 2018 and May 2019. One patient received secondary KT, and therefore was excluded. Finally, 119 patients (age 43.77±11.23 years; age range 21–67 years; 66 men, 53 women) who received their first KT, and that were not subjected to multi-organ transplant, were included in this study. This study was approved by the review board and ethical committee of our hospital ([2014]005). Written informed consent was obtained from all subjects before examination, in accordance with the Helsinki declaration.
US examination
Patients selected for conventional US underwent for routine gray-scale US, color Doppler US and pulsed Doppler US examination of iliac blood vessels with an EPIQ 5 (Philips Healthcare, Bothell, WA, USA) or iU 22 (Philips Healthcare, Bothell, WA, USA). Exams were performed by one radiologist, with 6 years of experiences in US. To show iliac blood vessels clearly, we used a 1–5 MHz convex transducer, or 3–9 MHz linear probe if necessary. We performed US with the patients in the supine position. The imaging protocol included grey-scale US evaluation of bilateral internal iliac artery, external iliac artery, and external iliac vein. Doppler US was used to assess the patency and to measure the maximum blood velocity (Vmax) of iliac blood vessels. Three measurements were taken, and the mean value was calculated. Next, CEUS was performed after completion of conventional US. The mechanical index was less than 0.06. The contrast agent used in this study was SonoVue ™ (Bracco, Milan, Italy). After identification of the common iliac artery branch, the transducer was kept in a stable position while patients were instructed to take only shallow breathing. Then, the contrast agent was administrated as a 0.5 ml or 0.6 ml bolus and was immediately followed by a flush of 5 ml saline solution via an antecubital vein. Continuous imaging was available to observe iliac blood vessels in real-time. First, CEUS was performed for the right side of iliac blood vessels, and, after a time interval for about 15 minutes, for the left side of iliac blood vessels. All imaging and video clips were stored digitally on the hard disk for subsequent analysis.
Image evaluation
The vasculature was evaluated with respect to the following parameters: blood vessel visible, stenosis, occlusion, plaque, thrombus, and so on. The quality of flow visualization was evaluated by two radiologists (one with 6 years of experience in US, and another with 4 years of kidney US experience). The two radiologists were not blinded to clinical data and other imaging findings. When they disagreed on the results’ evaluation, the image was re-evaluated by another experienced radiologist (with more than 15 years of US experience) until a consensus was reached. Furthermore, the flow visualization quality of the internal iliac artery was subjectively rated by assigning a grade (scale of 0–2), as follows [12]: grade 0, non-visualization of the vessel segment; grade 1, patchy visualization with partial lumen of the vessel and distal lumen not seen; and grade 2, clearly defined visualization of the vessel segment.
Kidney transplant procedure and vessel inspection
KT was performed in our hospital, according to the surgical standards. The kidney transplant was placed in the right or left iliac fossa. Vascular reconstruction was anastomosed to the internal iliac artery placed end-to-end to the donor renal artery. The vein was anastomosed end-to-side to the external iliac vein. The patency of the iliac artery and vein was confirmed by surgery.
Outcomes analysis
The follow-up time lasted from post-transplantation to discharge. The follow-up outcomes included: delayed graft function (DGF), rejection, vascular complication, higher resistive index (RI) and clinically well patient. DGF is defined as dialysis requirement in the first week after KT. According to the results from previous studies [15], we used the 0.80 as an increased RI. Patients were divided into two groups: group 1 with abnormal follow-up results and group 2 with normal follow-up results. The group of abnormal results included: rejection, vascular complications, DGF, and abnormal US findings.
Statistical analysis
Statistical analysis was performed with SPSS software (Version 24.0, IBM, Armonk, NY, USA). Student’s t-test for continuous variables or χ2 test for categorical variables was used to compare the two groups. Binary logistic regression was used to determine risk factors associated with post-transplant outcomes. Correlation analysis was performed with Pearson or Spearman tests. To calculate the accuracy of the iliac vessels’ patency we checked each blood vessel before and after the injection of contrast material. Interobserver agreement was measured by using weighted Kappa statistics (< 0.2: poor agreement; 0.2–0.4: fair agreement; 0.41–0.6: moderate agreement; 0.61–0.8: good agreement; 0.81–1.0: very good agreement). p < 0.05 indicated a statistical significance.
Results
Ranges of vascular diameters and peak velocities
The following conditions of 119 patients were analyzed: bilateral internal iliac arteries, external iliac arteries, and external iliac veins. Table 1 shows the vascular diameter and Vmax.
Preoperative iliac blood vessels hemodynamic parameters in 119 patients
Preoperative iliac blood vessels hemodynamic parameters in 119 patients
Vmax: the maximum blood velocity. SD: standard deviation
Participants’ detailed characteristics, according to the follow-up outcomes, are summarized in Table 2. Group 1 included 26 patients with abnormal results: 5 out of 26 were experiencing DGF, 3 cases presented rejection, 1 case suffered from transplant renal artery stenosis, 1 case presented transplant renal vein thrombus and 1 case suffered from transplant renal artery rupture. 15 patients out of 26 presented abnormal US examination with a higher RI in the graft renal artery. Group 2 included 93 patients, which presented a good renal function recovery and a normal US examination after surgery.
Characteristics of patients according to the follow-up clinical outcomes
Characteristics of patients according to the follow-up clinical outcomes
SCr: blood serum creatinine; US: ultrasound; Vmax: the maximum blood velocity.
No significant difference between the two groups was found regarding plaques, velocity of the internal iliac artery and velocity of the external iliac vein (p = 0.192, p = 0.187 and p = 0.608). On the contrary, statistically significant differences between the two groups were found in the diameter of internal iliac arteries (p = 0.033). Factors associated with abnormal follow-up outcomes are summarized in Table 3. At univariate analysis level, the diameter of internal iliac artery was associated with abnormal follow-up outcomes (p = 0.036). At multivariate analysis level, the diameter of the internal iliac artery and age were associated independently with abnormal follow-up outcomes (p = 0.011 and p = 0.037).
Risk factors of abnormal follow-up clinicaloutcomes
CI: confidence interval, OR: odds ratio.
Pearson analysis revealed no significant correlation between Vmax of the internal iliac artery and postoperative blood serum creatinine (SCr) (r = 0.120, p = 0.193). No significant relationship was shown between plaques of the internal iliac artery and postoperative SCr (r = 0.064, p = 0.487).
The analysis of the bilateral iliac arteries revealed that 42 patients out of 119 (35.3%) suffered from arterial plaques. The analysis of 238 arterial segments showed that 79 plaques (33.2%) were located as following: 7 (2.9%) right external, 31 (13.9%) right internal, 9 (3.8%) left external, and 32 (13.4%) left internal iliac arterial segments. By using CEUS, the lumen of iliac arteries was clearly visible in these patients.
Flow
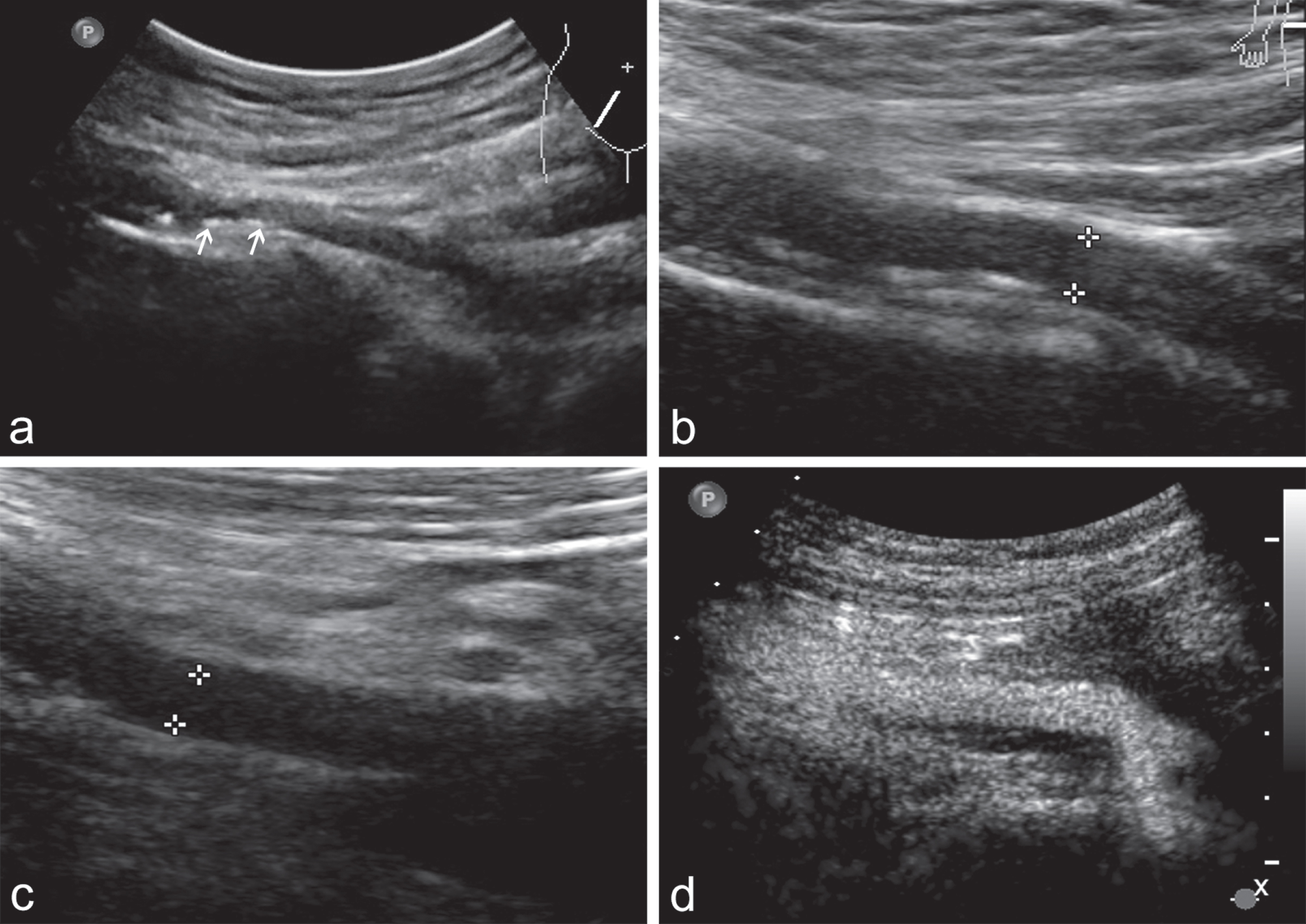
The flow visualization scores of all the internal iliac arteries improved significantly (Table 4) with CEUS (Fig. 1). Patients included in the waiting list for KT, presented: 2 cases of severe arteriosclerosis of the iliac artery and 2 cases of external iliac vein thrombus, detected by conventional US and CEUS. The co-existence of these two aspects was considered significant for the detection of external iliac vein thrombus: intraluminal echoes within the vein on gray-scale images and a lack of flow signal on CEUS images (Fig. 2). Conventional US showed multiple plaques on external or internal iliac arteries in 42 out of 119 patients (35.3%), but these plaques were not seen after contrast material injection.
Summary of internal iliac arteries visualization scores
Summary of internal iliac arteries visualization scores
*Data are number of participants. US: ultrasound; CEUS: contrast-enhanced ultrasonography.

The flow visualization of bilateral internal iliac arteries improved significantly with contrast-enhanced ultrasonography (CEUS). (a) The right iliac artery. (b) The left iliac artery.

Images in a 43-year-old man with indwelling femoral vein catheters before being wait-listed for kidney transplantation. (a) The right external iliac vein was filled with echoes (thin arrow), and (b) does not fill with flow signal in both the longitudinal and (c) transverse planes (thick arrow). This finding is compatible with venous thrombus.
The right internal iliac artery and external iliac vein were surgically confirmed patent in 112 patients; 7 cases out of 119 patients received KT in the left iliac fossa. The left internal iliac artery and external iliac vein were surgically confirmed patent in these patients. Doppler US demonstrated that external iliac arteries and external iliac veins were patent in all these 119 patients, and a clear flow and remote branch were visible in the internal iliac artery of 72 patients out of 119. Flow was clearly visualized in all these internal iliac arteries, external iliac arteries and external iliac veins after the injection of contrast agents.
It was not possible to obtain a clear vision of the internal iliac artery of 47 patients out of 119 (39.5%). 46 patients were visible in their partial lumen of the blood vessel, but the distal lumen was not detected within the internal iliac artery in Doppler US. 47 patients had no clear flow in the internal iliac artery in Doppler US. Flow was clearly visualized in all these internal iliac arteries after contrast material injection, and patency was confirmed by surgical results.
Diagnostic accuracy and agreement for assessment of internal iliac arteries
The accuracy of conventional US in determining the patency of internal iliac arteries was 60.5% (95% CI: 51.1%, 69.2%). The accuracy of CEUS in determining the patency of internal iliac arteries was 100% (95% CI: 93.7%, 100%). The difference between the accuracy of both conventional US and CEUS was significant (p < 0.001). A high level of agreement on flow visualization was reached among all individual assessments (Kappa = 0.857 on assessment of the internal iliac artery).
Impact on the surgical strategy after US
In the first patient, the surgical strategy was modified according to US findings. The patient was diagnosed with plaque formation on the right internal iliac artery. However, there was no plaque on the left internal iliac artery. The lumen of bilateral external iliac artery was thin. In addition, the lumen diameter of bilateral internal iliac artery differed by only one millimeter. As a result, this patient was received KT in the left iliac fossa with an end-to-end anastomosis on the left internal iliac artery. Vascular matching during surgery was satisfactory, and the perfusion of graft kidney after KT was excellent (Fig. 3).
Images in a 39-year-old woman who ready to receive transplantation. Conventional ultrasound (US) and contrast-enhanced ultrasonography (CEUS) in one patient with the modified surgical strategy. The patient was received kidney transplantation at the left iliac fossa with an end-to-end anastomosis to the left internal iliac artery. (a) The plaque of a right internal iliac artery (thin arrow). (b) The lumen diameter of the right internal iliac artery. (c) The lumen diameter of the left internal iliac artery. (d) The contrast-enhanced US imaging of the left internal iliac artery.
In the second patient, there were scattered multiple plaques and atherosclerosis on the bilateral iliac artery. As a result, this patient was excluded from KT (Fig. 4).
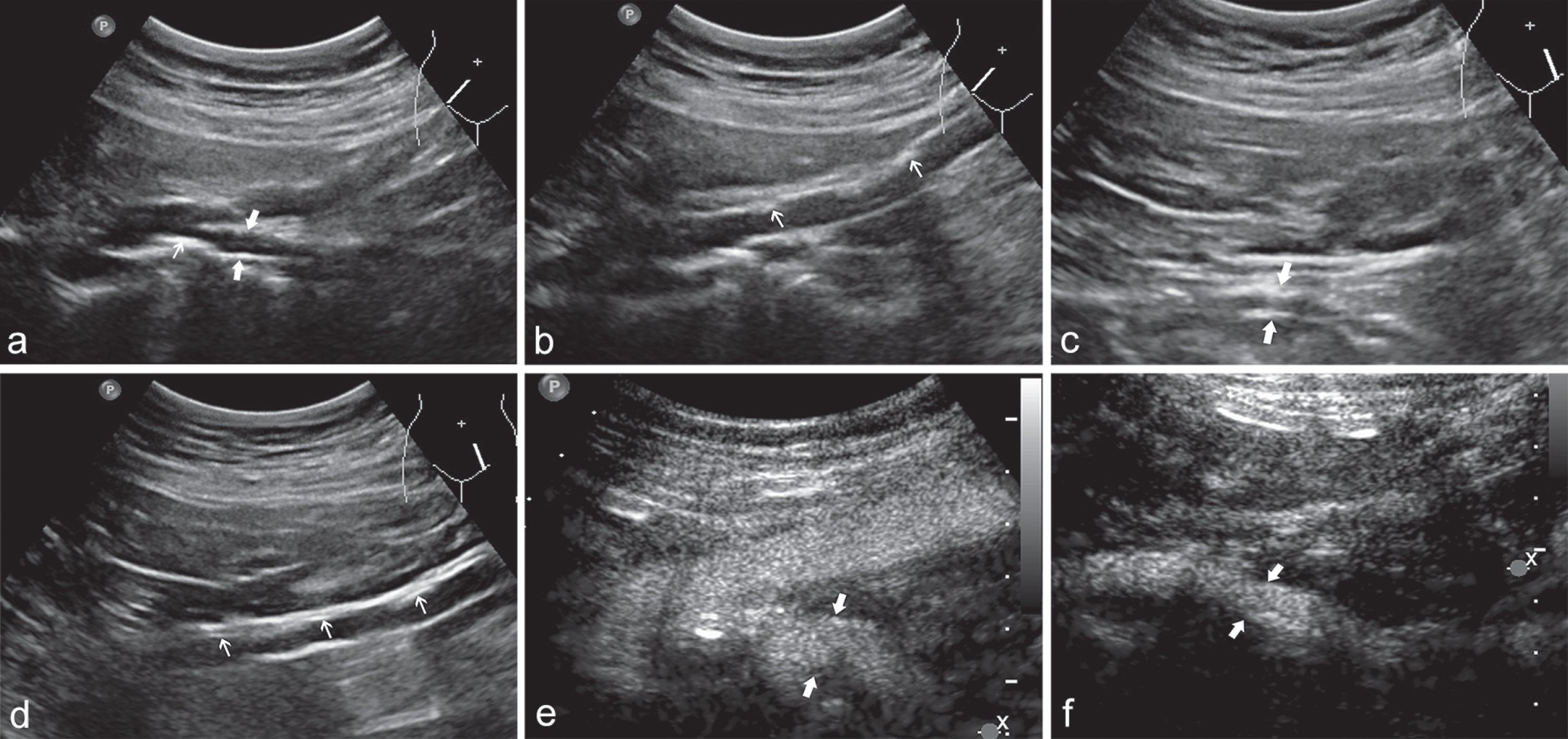
Images in a 71-year-old man who ready to receive transplantation. Conventional ultrasound (US) and contrast-enhanced ultrasonography (CEUS) showed there were scattered multiple plaques and atherosclerosis on the bilateral internal iliac artery and the left external iliac artery. This patient was excluded from kidney transplantation. The right external and internal iliac artery. (a) The plaque of the right internal iliac artery (thin arrow). (b) The plaque of the right external iliac artery (thin arrow). (c) The left internal iliac artery. (d) The plaque of the left external iliac artery (thin arrow). (e) The CEUS imaging of the right internal iliac artery (thick arrow). (f) The CEUS imaging of the left internal iliac artery (thick arrow).
In the third patient, a wall thrombus of the bilateral external iliac vein and femoral vein was detected by conventional US and CEUS. Furthermore, there were scattered multiple plaques on the distal end of the bilateral external iliac artery. The proximal lumen was not visible in the bilateral external and internal iliac arteries. Consequently, this patient was excluded from KT.
CEUS plays a role in the early detection of rejection and the follow-up examination after kidney transplantation [16]. Moreover, the contrast medium (SonoVue™) does not influence the renal microcirculation [17]. CEUS has the advantage of contrast agents without nephrotoxicity, thus it is safe to apply for patients with renal allograft dysfunction [18]. In our study, we applied a CEUS technique to evaluate iliac blood vessels’ characteristics, patency and course in patients with severely impaired kidney function or on dialysis whilst planning KT for the first time. The aim of our study was to improve the visualization of the internal iliac artery. We have been adding CEUS to conventional US and determining that whether US findings are related to transplant outcomes.
Doppler US can evaluate iliac blood vessels and detect the occurrence of atherosclerosis or vein thrombus. However, it is often inaccurate in evaluating deep blood vessels, especially in patients with thick abdominal wall and polycystic kidney disease. CTA and MRA can assess aorto-iliac vasculature, allowing a better choice of recipient selection and a more accurate planning for vascular anastomosis [19]. But they are limited in evaluating venous anatomy and calcification. The former limitation is of crucial importance, as dwelling femoral vein catheters has been often employed in some patients with dialysis, contributing to venous thrombus or occlusion.
Internal iliac artery should be selected as a first choice in transplant renal artery anastomosis. First, an end-to-end anastomosis to the internal iliac artery has the obvious advantage of hemodynamics, and this surgical option can provide adequate blood perfusion for graft kidneys. In addition, it does not affect blood supply of the lower extremity artery in patients with peripheral arterial disease, advanced age or diabetes. However, previous studies including small samples have compared end-to-end anastomosis to the internal iliac artery versus end-to-side anastomosis to the external iliac artery, showing that both methods are providing similar results both in the early postoperative period and 3 years follow-up [20, 21].
The diameter of the internal iliac artery and age were associated with abnormal follow-up outcomes. Furthermore, post-transplant outcomes are associated with various factors, not only with iliac blood vessel factors but also with other factors such as surgeon’s experience, infection, urinary obstruction, rejection and so on. Preoperative US findings, which included the internal iliac artery velocity and plaques, might not determine post-operative renal function, so multiple factors should be considered together in the future study. CEUS can help to improve the visualization of the internal iliac artery, but there was no significant correlation with complications after surgery.
Indeed, vascular plaques of the iliac area are frequent in the elderly diabetic population [22]. The location or extent of plaques can compromise vascular anastomosis. And the anastomosis time might be prolonged, which represents a major risk factor for poor survival [23]. The advantage of a complete preoperative vascular assessment is that the surgical vascular procedure can be planned before KT.
Andres et al. [19] reported that 29% of candidates were excluded from the waiting list because of atherosclerosis. A research reported 3% of candidates excluded from KT because of severe vascular disease diagnosed with Doppler US [7].
In a study, the internal iliac artery was not demonstrated with conventional US in 69% of 106 vessels [10]. In our study, the internal iliac artery was unclearly visualized in 47 out of 119 patients (39.5%). The difficulty in identifying the flow in 46 patients was attributed to the deep location of blood vessels. One patient had polycystic kidney disease and the kidneys increased up to the pelvic cavity. However, the injection of contrast agents can clearly solve this problem and improve the accuracy in displaying the flow up to 100%. Hom et al. [12] have reported that CEUS could help to improve the hepatic artery and portal vein visualization in liver transplant patients. A research about liver carcinoma reported that flow was not observed at depths greater than 7 cm by US, but CEUS helped to monitor flow in the deep location [24].
Compared with color Doppler, gray-scale US can display the vascular outline and wall more intuitively and accurately. Pulse Doppler can measure hemodynamic parameters and provide functional information, which is one of the advantages of US compared with other imaging methods. CEUS can improve the quality of vascular imaging, which is similar to angiography, but does not provide hemodynamic parameters. CEUS is useful for vascular imaging in cases of challenging conditions for color Doppler US. However, CEUS is limited by severe calcifications. Therefore, the combination of conventional US and CEUS can improve the diagnostic value of vascular disease.
However, there are several limitations in the present study. First, this study is a single-center design with a relatively small number of patients who underwent KT. Second, the follow-up time was short, so a long-term follow-up study is foreseen. In addition, this study was designed to estimate diagnostic accuracy of conventional US and CEUS. Different imaging techniques were neither compared, nor evaluated. Further studies will be required to have more evidence available. In conclusion, compared with conventional US, CEUS helps to improve the visualization of the internal iliac artery, especially for iliac arteries in the deep location, but no significant correlation was found with post-transplant outcomes. Conventional US and CEUS have the potential to serve as effective methods to evaluate anatomy and hemodynamics of iliac blood vessels and have a potential value while defining clinical algorithms in surgery decision-making.
Footnotes
Acknowledgments
This study was supported by the Clinical Research Innovation and Cultivation Fund Project of Renji Hospital, School of Medicine, Shanghai Jiaotong University (grant number PYI-17-008).