
Abstract
BACKGROUND:
The prevention of rheologic alterations in erythrocytes may be important for reducing sepsis-associated morbidity and mortality. Remote ischemic preconditioning (RIPC) has been shown to prevent tissue damage caused by severe ischemia and mortality resulting from sepsis. However, the effect of RIPC on erythrocytes in sepsis is yet to be determined.
OBJECTIVE:
To investigate the effect of RIPC on rheologic alterations in erythrocytes in sepsis.
METHODS:
Thirty male Sprague-Dawley rats were used in this study. An endotoxin-induced sepsis model was established by intraperitoneally injecting 20 mg/kg LPS (LPS group). RIPC was induced in the right hind limb using a tourniquet, with three 10-minute of ischemia and 10 min of reperfusion cycles immediately before the injection of LPS (RIPC/LPS group) or phosphate-buffered saline (RIPC group). The aggregation index (AI), time to half-maximal aggregation (T1/2), and maximal elongation index (EImax) of the erythrocytes were measured 8 h after injection.
RESULTS:
The AI, T1/2, and EImax values in the LPS and RIPC/LPS groups differed significantly from those in the RIPC group, but there were no differences between the values in the LPS and RIPC/LPS groups.
CONCLUSIONS:
RIPC did not prevent rheologic alterations in erythrocytes in the rat model of LPS-induced endotoxemia.
Introduction
Sepsis is a clinical syndrome characterized by physiological, biological, and biochemical abnormalities induced by a dysregulated host response to infection [1]. Sepsis exhibits a continuum of severity, ranging from infection and bacteremia to sepsis and septic shock, which can lead to multiple organ dysfunction syndrome and death [2].
Increased red blood cell (RBC) aggregation, along with other clinical variables, has been shown to be a clinically significant factor for identifying sepsis in animal models of lipopolysaccharide (LPS)-induced endotoxemia, and it may be an early indicator of sepsis [3]. In addition, RBC deformability has been suggested to be a useful monitoring parameter for predicting the prognosis in patients with sepsis [4]. RBCs transport oxygen to tissues and remove carbon dioxide from them via capillaries. The deformability of RBCs is essential for their successful passage through capillaries and splenic sinuses. Pathological conditions affecting RBCs, such as sepsis, can lead to significant alterations in tissue perfusion [5]. The mortality rate in sepsis with cryptic shock, which manifests as global tissue hypoperfusion, was reported to be similar to that in overt septic shock; hence, microcirculation should be closely monitored in patients with sepsis [6, 7].
These concepts provide the basis for therapeutic strategies for improving tissue perfusion. The prevention of rheologic alterations in RBCs can help reduce the morbidity and mortality associated with sepsis [8].
Reportedly, remote ischemic preconditioning (RIPC) exhibits a protective effect against ischemic reperfusion injury caused by brief episodes of ischemia in distant tissues or organs [9, 10]. Recent studies have shown that RIPC suppresses inflammatory mediators and improves survival in an animal model of LPS-induced sepsis [11, 12]; however, its effect on RBC rheology in sepsis is yet to be confirmed.
In this study, we investigated the effects of RIPC on RBC aggregation and deformability in an LPS-induced sepsis model by measuring the aggregation index (AI), time to half-maximal aggregation (T1/2), and maximal elongation index (EImax).
Materials and methods
Animals and experimental protocols
The experimental protocol adopted in this study was approved and registered by the Korea University Medical College Institutional Animal Care and Use Committee KUMC-IUAC (KOREA-2018-0163). Thirty male Sprague-Dawley rats (mean age, 6 weeks; weight, 300 g each) were used in this study. Before the experiment, the rats were stabilized for 1 week in a controlled environment.
An endotoxin-induced sepsis model was established by the intraperitoneal (IP) injection of 20 mg/kg LPS. A commercial preparation of LPS from Escherichia coli O127:B8 (Sigma-Aldrich, St. Louis, MO, USA) was dissolved in 0.4 mL of phosphate-buffered saline (PBS). RIPC was induced in the right hind limbs of the rats using a tourniquet with three 10-minute of ischemia and 10 min of reperfusion cycles.
The rats were randomly allocated to three groups (n = 10 per group): (1) RIPC group: after RIPC, the mice received PBS via IP injection; (2) RIPC/LPS group: after RIPC, the mice received LPS via IP injection; and (3) LPS group: the mice received LPS via IP injection.
Anesthetization and blood sampling
Cardiac blood collection was performed under sevoflurane anesthetization 8 h after LPS or PBS injection. A 5 mL aliquot of whole blood was drawn using a heparin-coated syringe and collected into BD Microtainer® blood collection K2EDTA tubes (0.5 mL, BD, Franklin Lakes, NJ, USA) to determine the platelet count or into BD Microtainer® blood collection BD SST™ tubes (0.5 mL, BD, Franklin Lakes, NJ, USA) to measure the bilirubin and creatinine levels.
Analytical procedures
A microfluidic ektacytometer and aggregometer (RheoScan-AnD300; Rheo Meditech, Korea) was used to evaluate RBC aggregation and deformability [13]. To assess RBC deformability, 5μL of blood was mixed with 500μL of 0.14 mM polyvinylpyrrolidone (PVP; molecular weight, 360,000) buffer solution. Following this, RBC deformability was assessed in 500μL of the mixture using RheoScan-AnD300. EImax was analyzed under maximal shear stress, as described in a previous study [3].
To assess RBC aggregation, 500μL of whole blood was centrifuged at 1500×g for 5 min at room temperature and washed twice with PBS under the same gravitational force [9]. The washed blood sample was suspended in 0.14 mM PVP at 0.4 % hematocrit. Following this, 8μL of the processed blood was pipetted into an RSD-C01 kit, a microchip-based cell aggregometer, and aggregability was analyzed based on a syllectogram. The AI and T1/2 values were determined.
The i-STAT handheld analyzer (Abbott Point of Care Inc., USA) was used to measure the lactate levels.
Statistical analysis
Data are presented as mean±standard error of mean. The values were compared using the Kruskal–Wallis test and median test, followed by post-hoc Wilcoxon rank-sum test, using SAS version 9.4 (SAS Institute, Cary, NC, USA). Statistical significance was set at p < 0.05.
Results
RBC aggregability and deformability
The AI values in the LPS and RIPC/LPS groups were significantly higher than those in the RIPC group (p = 0.008 and 0.014, respectively) (Fig. 1A). The T1/2 values in the LPS and RIPC/LPS groups were significantly lower than that in the RIPC group (p < 0.0001 and = 0.011, respectively). However, there were no differences in the AI and T1/2 values between the LPS and RIPC/LPS groups (Fig. 1B).

Red blood cell (A) aggregation index (AI, in %) and (B) time to half-maximal aggregation (T1/2, in seconds). Data are expressed as mean±standard error of mean. *p < 0.05 vs. LPS group; †p < 0.05, RIPC group. Mice in the RIPC group underwent remote ischemic preconditioning (RIPC) and received an intraperitoneal (IP) injection of 0.4 mL of phosphate-buffered saline; mice in the RIPC/LPS group underwent RIPC and received an IP injection of 20 mg/kg lipopolysaccharide (LPS); mice in the LPS group received an IP injection of LPS.
The EImax value decreased significantly in the LPS and RIPC/LPS groups compared to that in the RIPC group (p = 0.002 and 0.001, respectively), whereas no difference was observed between the values in the LPS and RIPC/LPS groups (Fig. 2).
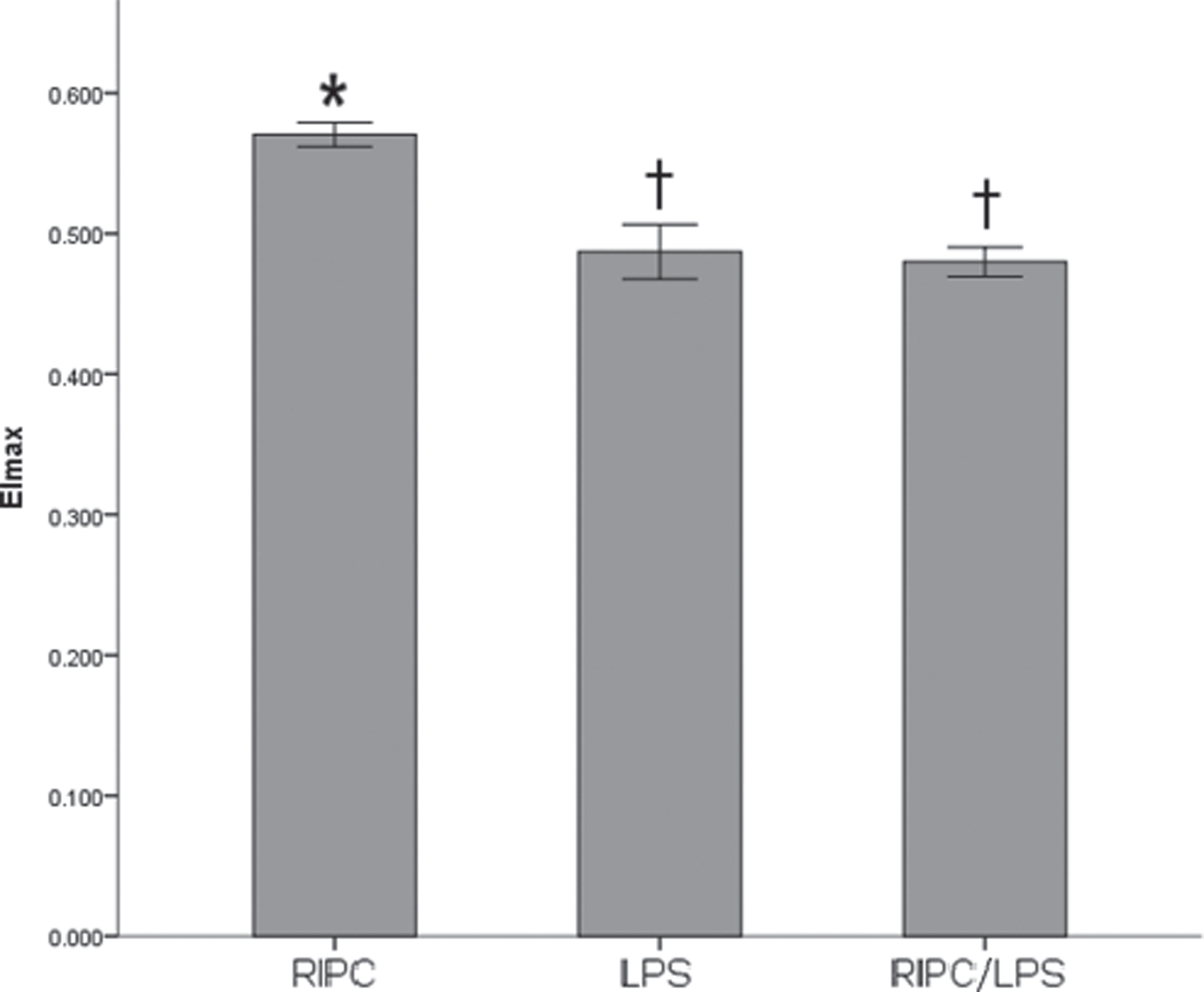
Red blood cell deformability (maximal elongation index, EImax) at maximal shear stress. Data are expressed as mean±standard error of mean. *p < 0.05 vs. LPS group; †p < 0.05, RIPC group. Mice in the RIPC group underwent remote ischemic preconditioning (RIPC) and received an intraperitoneal (IP) injection of 0.4 mL of phosphate-buffered saline; mice in the RIPC/LPS group underwent RIPC and received an IP injection of 20 mg/kg lipopolysaccharide (LPS); mice in the LPS group received an IP injection of LPS.
The platelet counts in the LPS and RIPC/LPS groups decreased compared to those in the RIPC group (both p < 0.001) (Fig. 3), but there was no significant difference between the values obtained for the LPS and RIPC/LPS groups.
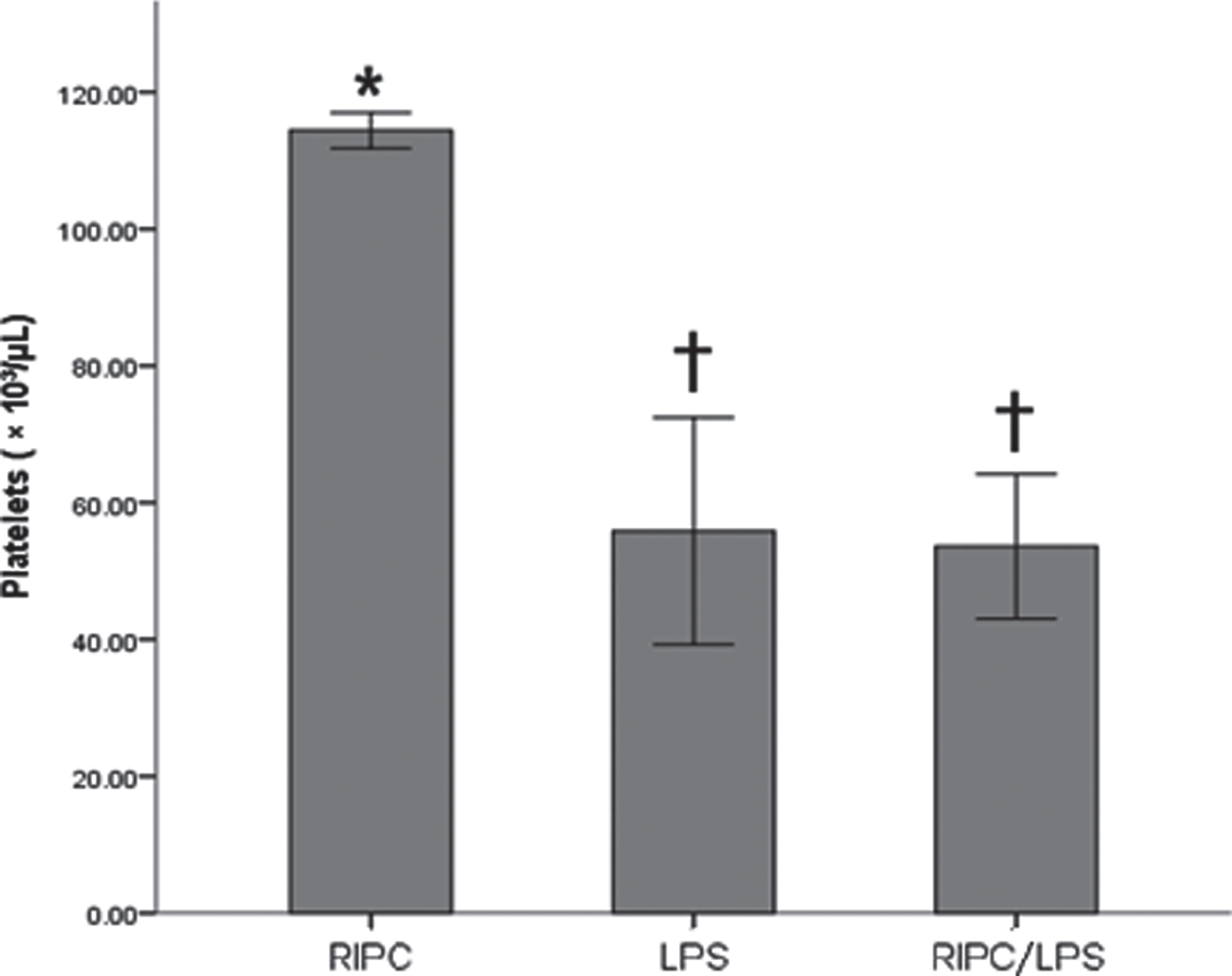
Platelet counts. Data are expressed as mean±standard error of mean. *p < 0.05 vs. LPS group; †p < 0.05, RIPC group. Mice in the RIPC group underwent remote ischemic preconditioning (RIPC) and received an intraperitoneal (IP) injection of 0.4 mL of phosphate-buffered saline; mice in the RIPC/LPS group underwent RIPC and received an IP injection of 20 mg/kg lipopolysaccharide (LPS); mice in the LPS group received an IP injection of LPS.
The bilirubin levels appeared to increase in the LPS and RIPC/LPS groups compared to that in the RIPC group (p < 0.05); however, no difference was observed between the values obtained in the LPS and RIPC/LPS groups. No significant differences were observed among the lactate and creatinine levels of the LPS, RIPC/LPS, and RIPC groups (Table 1).
Data are expressed as mean±standard error of mean. *p < 0.05 vs. LPS group; †p < 0.05, RIPC group. The mice in the RIPC group underwent remote ischemic preconditioning (RIPC) and received an intraperitoneal (IP) injection of 0.4 mL of phosphate-buffered saline; mice in the RIPC/LPS group underwent RIPC and received an IP injection of lipopolysaccharide (LPS); mice in the LPS group received an IP injection of LPS.
Increased RBC aggregation and decreased deformability occurred early on with the reduction in platelet count; however, RIPC did not prevent RBC alterations in the LPS-induced endotoxemia model.
Although the age-standardized incidence and mortality of sepsis are declining, these remain a leading cause of ill health and are critical health problems worldwide [14]. Efforts for preventing infection, early identification of patients with sepsis, and timely implementation of targeted interventions can help improve clinical outcomes [15, 16].
Clinical and experimental studies have shown the co-occurrence of RBC abnormalities with clinical manifestations in the early stages of sepsis [3, 18]. Reportedly, peroxidation of RBC membrane lipids, increase in cytosolic calcium concentrations, impairment of oxygen-dependent adenosine triphosphate efflux from RBCs, and overproduction of nitric oxide induce mechanical abnormalities and physiological changes in RBCs in sepsis [19–22]. Persistent abnormalities in RBCs are associated with mortality in critically ill patients [23], and early interventions to prevent RBC alterations are important for prognosis [24].
RIPC was reported to attenuate the systemic inflammatory response, prevent organ damage, and improve survival in an LPS-induced mouse model [11, 25]. Therefore, it was hypothesized that RIPC would attenuate RBC alterations that occur during sepsis. However, the results of our study did not provide sufficient evidence to support the protective effect of RIPC against LPS-induced RBC alterations.
A possible explanation for this finding is that RIPC was not implemented appropriately. In RIPC, acute hind limb ischemia can be induced using open artery ligation and non-invasive methods with tourniquets such as McGivney hemorrhoidal ligator band, orthodontic rubber bands, and controlled tension tourniquet [26]. We used orthodontic rubber bands, which have been reported to produce tension at levels similar to that observed during ischemia [26]. In this study, RIPC was performed by the same individual who performed it in our previous studies, and the technical errors in RIPC could be ruled out by visually reproducible confirmation of limb ischemia and reperfusion (I/R). In terms of the effectiveness of IPC, as shown in our experimental method, three 10-minute cycles of IPC each have been reported to exhibit superior efficacy than one or two 5-minute cycles in experimental and clinical studies [27, 28].
A second explanation is that unlike mice, rats may not show the beneficial effects of RIPC on the attenuation of the inflammatory response and reduction of mortality in LPS-induced endotoxemia. Previous studies have shown that the immune-related changes in response to systemic toxicity and stress differed between rats and mice [29]. Moreover, there are hemorheological differences between species [30–32]. Therefore, the findings of experimental studies involving laboratory rodents must be interpreted carefully. Further research is needed to determine whether the effects of RIPC are species-dependent.
Another potential explanation is that the effect of RIPC on RBC rheology may not be apparent at 8 h after LPS administration, and the beneficial effect could be delayed. RIPC is known to induce a two-phase phenotype in I/R models [33, 34]. The first window of organ protection was initiated within 5–30 min of the final RIPC cycle and ended completely within 3 h. Conversely, the protective effect reappeared 24 h after the initial stimulation and lasted for 3 to 4 days. In other words, when fatal ischemia occurs at a time point beyond the protection period, a preconditioning effect that reduces the infarct size is not observed. While fatal organ ischemia, such as that induced by coronary vessel ligation, is an intended event, persistent systemic inflammatory responses occur inherently in endotoxemia and sepsis models. RIPC performed immediately before LPS injection attenuated systemic inflammatory responses, as measured at 1 and 4 h after LPS injection, and significantly improved survival [11]. The beneficial effects of RIPC in sepsis models have been reported in multiple studies [35–38]. Therefore, the beneficial effects of RIPC performed immediately before LPS injection can be predicted by observing the RBCs, and the protective effects should be measured serially in RBCs.
In addition, it must be considered whether the AI, T1/2, and EImax values can indicate the variability in the changes in erythrocytes. Reportedly, metabolic alterations and reduction in the levels of 2,3-bisphosphoglycerate (2,3-BPG) can be prevented with appropriate treatment, whereas reduction in deformability and alterations in the redistribution of membrane phospholipids seem to be permanent changes [24]. However, unlike that in patients with sepsis, the decreased RBC deformability index can be recovered in patients with trauma [17]. Therefore, the reversibility of changes in RBCs cannot be evaluated solely based on the value of the deformability index.
Sepsis-induced oxidative stress from activated neutrophils, plasma, endothelial cells, and RBCs can impair the functions of RBCs by inducing harmful changes that affect their structure, intracellular calcium homeostasis, and the concentrations of various intracellular enzymes [20, 39–42]. RBC morphology (shape and distribution width), cytoskeletal protein content, and 2,3-BPG concentration were evaluated to evaluate the effects of RIPC.
RBCs play an important role in tissue perfusion by oxygenating tissues and removing carbon dioxide [43]. Lactic acid levels, which are an indicator of tissue perfusion, can be easily checked clinically at the point of care to indirectly assess RBC function. Lactate levels are recommended as an indicator for resuscitation in patients with septic shock, and increased lactate levels suggest tissue hypoperfusion [44, 45].
In this study, there were no differences in the lactate levels between the groups, even when LPS induced alterations in the RBCs. In a previous study, when LPS-induced RBC alterations appeared, the ratio of the arterial-venous oxygen content difference and the veno-arterial carbon dioxide difference [P(v-a)CO2/C(a-v)O2], which is another indicator of tissue perfusion, did not change; however, the value increased at 12 h after LPS injection. This indicates that it takes time for the rheological changes in RBCs to affect tissue perfusion.
As mentioned above, this study had the following limitations. First, the effect of RIPC was measured only 8 h after LPS administration and was not observed in a time series. Second, the beneficial effects of RIPC were not confirmed in terms of survival rate, systemic inflammation, and organ dysfunction in the rat model of LPS-induced endotoxemia. Third, AI, T1/2, and EImax were used to evaluate RBC rheology in this study; however, the reversibility of RBC alterations could not be confirmed. Therefore, it is necessary to confirm the reversibility of RBC alterations with respect to functional, mechanical, and rheological properties.
Conclusions
RIPC did not prevent alterations in the RBCs in the rat model of LPS-induced endotoxemia. However, only hemorheological parameters, including AI, T1/2, and EImax, may not be useful for determining the reversibility of rheological alterations in RBCs at any given point of time; hence, the effect of RIPC on RBCs should be measured over different time periods using multiple clinical variables.
Conflicts of interest
The authors declare no conflict of interest.