
Abstract
BACKGROUND:
Sepsis is a medical emergency during which early detection is closely associated with mortality. In sepsis, red blood cell (RBC) abnormalities have been reported. However, it is not known how early RBC abnormalities are expressed compared with various clinical manifestations used in sepsis-related organ failure assessment (SOFA).
OBJECTIVE:
Therefore, using a lipopolysaccharide (LPS)-induced sepsis model we investigated the clinical significance of RBC abnormalities as an early indicator in the detection of septic injury compared with clinical variables.
METHODS:
Sprague-Dawley rats received LPS (20 mg/kg) intraperitoneally. Aggregation indices (AIs) and aggregation half-time (T1/2), and elongation indices (EI max) were measured. Clinical data-related SOFA and lactate were measured at 2 h, 4 h, 8 h and 12 h after LPS injection.
RESULTS:
AIs increased at 4 h, and T1/2 decreased at 2 h after LPS injection. Platelet counts decreased at 4 h, and lactate increased at 2 h after LPS injection. AIs showed strong correlations with T1/2 and platelets, EI max increased at 2 h after LPS injection, while EI max had a positive correlation with lactate.
CONCLUSIONS:
RBC aggregation appears to be an early indicator of clinical deterioration in sepsis and may represent a diagnostic indicator in sepsis.
Keywords
Introduction
Sepsis and septic shock are medical emergencies with a high mortality rate in ICUs. Early detection, infection source control, antibiotic administration, and hemodynamic management with fluids and vasopressors are critical steps to patient recovery [25]. During the first 6 h after septic shock, mortality increased by 5.3% for every hour of delay in norepinephrine infusion, and the absolute mortality rate increased by 0.3% due to hourly delay in antibiotic administration [2, 20]. International guidelines for the management of sepsis and septic shock were last revised in 2016 and the definition of sepsis was updated as a life-threatening organ dysfunction caused by a dysregulated host response to infection. Patients suspected of infection require quick sepsis-related organ failure assessment (qSOFA). In patients with a qSOFA score of 2 or more, organ dysfunction is assessed by SOFA and a SOFA score of 2 or more suggests sepsis [29].
In clinical and experimental sepsis, reduced RBC deformability and increased RBC aggregation has been reported [3, 24]. RBCs appear to be highly susceptible to septic injury and RBC abnormalities are an early warning signal of sepsis and a factor associated with microvascular dysfunction [7]. However, it is unknown how early RBC abnormalities are expressed compared with the various clinical manifestations used for SOFA. They may be attributed to heterogeneous intensive care population.
Endotoxin toxicity in rats observed in the sepsis model may facilitate comparison of the early phase of clinical disorder [8]. Therefore, we investigated whether RBC abnormalities show any clinical significance as an early indicator of septic injury compared with various clinical variables for SOFA in endotoxin induced sepsis model.
Materials and methods
Ethical approval
Before conducting the experiment, all our staff received user education from the Korea University Medical College-Institutional Animal Care and Use Committee (KUMC-IUAC) and followed the Guide for the Care and Use of Laboratory Animals. The animal experiment was approved and registered by KUMC-IUAC (KOREA-2018-0009).
Experimental animals and protocol
We used 80 male Sprague-Dawley rats (mean age, 6 weeks; weight, 300 g each). All the rats went through stabilization period for 2 weeks under controlled environment before use in the experiment. Endotoxin-induced sepsis model was established by injecting 20 mg/kg LPS (E. coli O127: B8; Sigma, St. Louis, MO, USA) in 0.4 mL PBS solution, intraperitoneally.
Rats were randomly divided into 5 groups (n = 8, each): (1) Control group, blood was collected 12 h after intraperitoneal injection of PBS solution; (2) LPS 2H group, (3) LPS 4H, (4) LPS 8H, and (5) LPS 12H groups, based on blood collection at 2 h, 4 h, 8 h, and 12 h, respectively, after injection of LPS.
Anesthesia and blood sampling
Animals were anesthetized with intraperitoneal injection of Zoletyl (tiletamine and zolazepam, VirbacKorea, Korea) and Rompun (xylazine, Bayer, Germany), and intubated with 16G Jelco (IV catheter radiopaque, Smiths Medical, Italy), and ventilated with room air at the rate of 80 cycles/min and a tidal volume of 3 mL. After 10 min of stabilization, an incision was made in the abdominal area and the abdominal aorta and renal vein were exposed for blood sampling. Each 0.5 mL of arterial and venous blood was collected with a heparin-coated syringe for blood gas analysis. An aliquot of 5 mL of venous blood was also withdrawn with a heparin-coated syringe and collected in BD Microtainer® blood collection K2EDTA tubes (0.5 mL, BD, Franklin Lakes, NJ, USA) to measure platelets, and in BD Microtainer® blood collection BD SSTtrademark tubes (0.5 mL, BD, Franklin Lakes, NJ, USA) for the measurement of bilirubin and creatinine.
Analytical procedures
Arterial and venous blood gas analysis was performed using i-STAT handheld analyzer (Abbott Point of Care Inc., USA) [17] to measure pH, PCO2, PO2, SO2, hemoglobin, and lactate.
SOFA score comprises six systemic items, each for the respiratory (the ratio of arterial oxygen partial pressure to fractional inspired oxygen, PaO2/FiO2), cardiovascular (mean blood pressure), hepatic (total bilirubin), coagulation (platelets), renal (creatinine) and neurological (Glasgow coma scales) systems. Platelet count, total bilirubin and creatinine levels were measured. PaO2/FiO2 was calculated with arterial and venous blood gas analysis. Instead of the mean arterial pressure representing organ perfusion, the difference in veno-arterial carbon dioxide tension known as P(v-a)CO2 was measured, since it is proposed as an adjunctive test for the detection of adequate cardiac output with microcirculatory flow and perfusion [13].
Tissue hypoperfusion was also monitored by calculating the ratio of veno-arterial carbon dioxide tension difference to the arteriovenous oxygen content difference, i.e., P(v-a)CO2/C(v-a)O2 based on blood gas analysis [14]. Arterial or venous blood oxygen contents (CaO2 or CvO2) represent the amount of oxygen carried by hemoglobin [1.34×SaO2 (or SvO2)×Hb] and dissolved in plasma [0.003×PaO2 (or PvCO2)].
RBC aggregation and deformability were evaluated using a microfluidic ektacytometer and aggregometer (RheoScan-AnD300: Rheo Meditech, Korea) [27, 28]. Erythrocyte deformability was analyzed by mixing 5 μL of whole blood with 500 μL of 0.14 mM polyvinylpyrrolidone (MW 360,000) buffer solution. The 500 μL of the mixture was pipetted into RSD-K01 kit and analyzed with a RheoScan-AnD300. Maximal elongation indices (EImax) was measured under maximal shear stress based on a previous study [18].
To analyze erythrocyte aggregation, we obtained an aliquot of 500 μL of rat whole blood and centrifuged the blood sample under 1500 g for 5 min at room temperature and washed with PBS twice [9] under the same gravity force. We removed the plasma at every step and suspended washed blood components in 0.14 mM PVP at a hematocrit of 0.4 1/1. We added 8 μL of the processed blood into an RSD-C01 kit, a microchip-based cell aggregometer, and analyzed its aggregability with a syllectogram. Using a curve fitting program, we determined the aggregation indices (AI) and aggregation half-time [T1/2 (sec), time to half-maximal aggregation]. We also repeated the analysis three times for each sample.
Statistical analysis
Data were presented as means±standard error of mean. SAS version 9.4 (SAS Institute, Cary, NC, USA) was used. Kruskal-Wallis test and median test were used to detect significant differences between groups. Wilcoxon rank-sum test was performed for a post-hoc analysis. Pearson’s correlation test was used to analyze the correlation between variables. A p-value less than 0.05 indicated statistical significance.
Results
Red blood cell aggregability and deformability
AIs showed significant difference between the groups (P = 0.007) and increased significantly in LPS 4H, 8H, and 12H groups than in the control group (P = 0.04, P = 0.01, and P = 0.02, respectively) (Fig. 1). T1/2 also showed significant differences between the groups (P = 0.009) and decreased significantly in LPS 2H, 8H and 12H groups than in the control group (P = 0.006, P = 0.009, and P = 0.02, respectively). EI max increased significantly in LPS 2H, 4H, and 12H groups (Fig. 2).
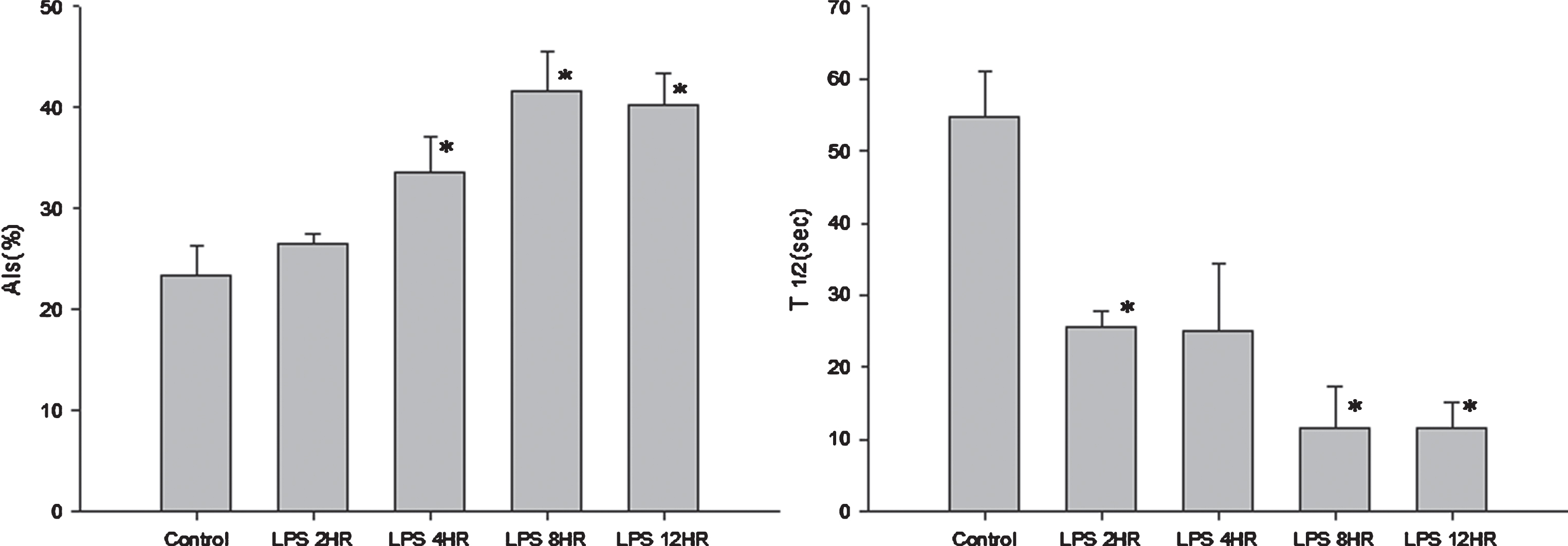
Red blood cell (RBC) aggregability index (AI in %) and aggregation half-time (T 1/2 in sec) means±SEM., *p < 0.05 vs. Control. Control group, blood was collected at 12 h after intraperitoneal injection of PBS solution; LPS 2H, LPS 4H, LPS 8H, LPS 12H groups, blood was collected at 2 h, 4 h, 8 h, and 12 h, respectively, after injection of LPS.
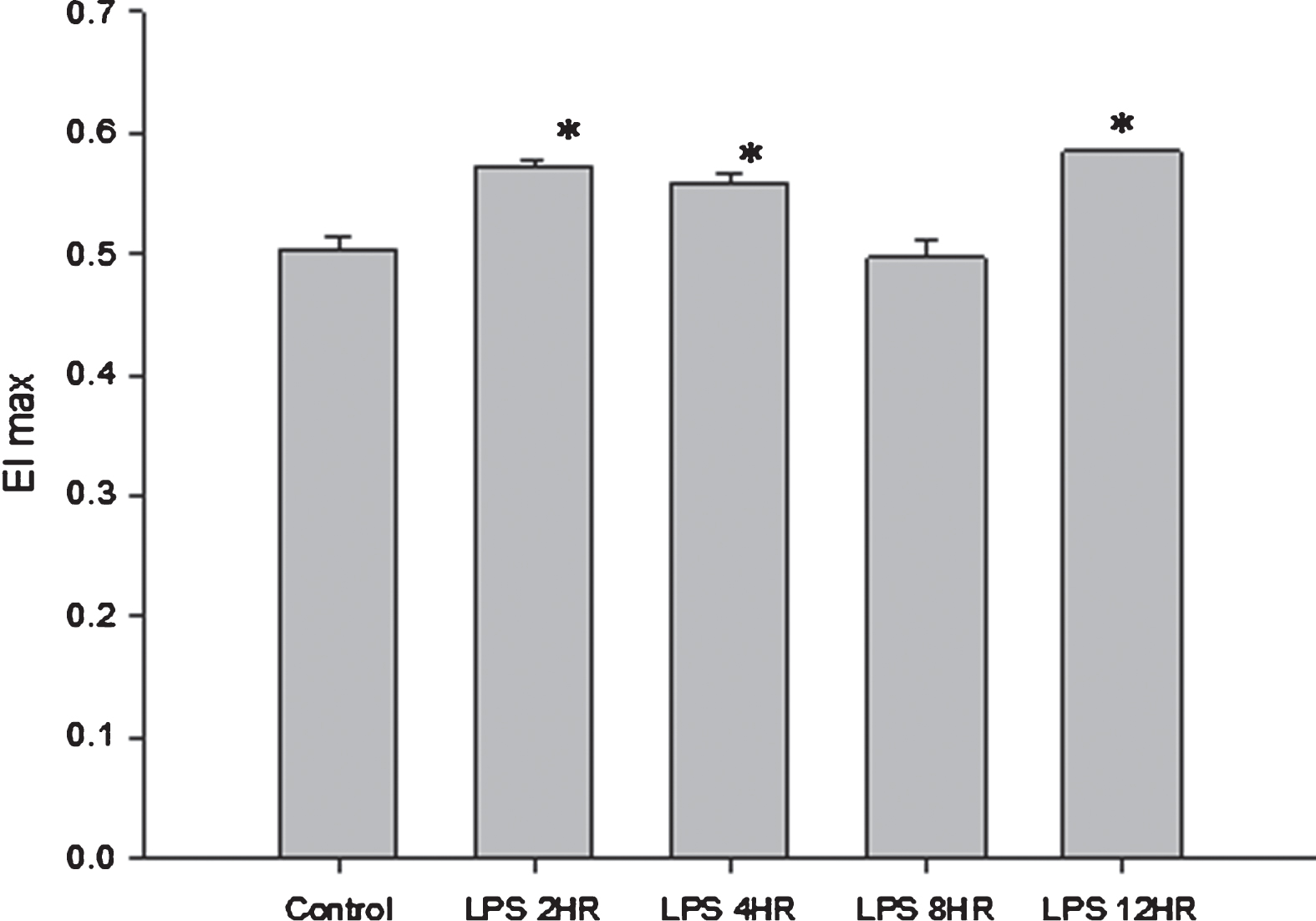
Red blood cell (RBC) deformability (elongation indices, EIs) at maximal shear stress means±SEM., *p < 0.05 vs. Control. Control group, blood was collected at 12 h after intraperitoneal injection of PBS solution; LPS 2H, LPS 4H, LPS 8H, LPS 12H group, blood was collected at 2 h, 4 h, 8 h, and 12 h, respectively, after injection of LPS.
AIs showed significantly negative correlations with T1/2 and platelet count (r = –0.864, P < 0.0001, respectively). T1/2 showed a positive correlation with platelet count and negative correlation with creatinine, while EI max had a positive correlation with lactate (Table 1).
Pearson’s correlation analysis of variables
Correlation coefficient (p-value).
Platelet counts were significantly lower in LPS 4H, 8H and 12H groups compared with the control group (P = 0.005, P = 0.003, and P = 0.03, respectively) (Table 2). Creatinine levels were significantly higher in LPS 2H and 4H groups than in the control group (P = 0.019 and P = 0.027, respectively), bilirubin was significantly higher in LPS 8H group than in the control group (P = 0.007) and lactate was significantly higher in LPS 2H, 4H, and 8H groups and substantially higher in LPS 12H group than in control group (p = 0.009, P = 0.01, and P = 0.006, respectively).
Clinical variables of 5 groups after LPS injection
Clinical variables of 5 groups after LPS injection
means±SEM., *p < 0.05 vs. Control. Control group, blood was collected 12 h after intraperitoneal injection of PBS solution; LPS 2H group, LPS 4H, LPS 8H, LPS 12H group (n = 8, each), blood was collected at 2 h, 4 h, 8 h, and 12 h, respectively, after injection of LPS.
Platelet count showed a statistically significant correlation with AIs, T1/2, bilirubin, creatinine, and P(v-a)CO2/C(a-v)O2 (Table 1).
RBC abnormalities occurred at an early stage involving clinical valuables such as platelet count and lactate. RBC aggregation and T1/2 were closely associated with platelet reduction.
Sepsis is characterized by a profoundly disturbed microcirculation with increased non-perfused capillaries and shunting [12, 31]. Persistent microcirculatory alteration leads to organ failure despite normal global hemodynamic parameters [16, 26]. Cryptic shock is associated with a similar mortality rate as overt shock in sepsis, and microcirculation and tissue perfusion should be closely monitored in septic patients [15, 23].
Hemorheological properties are important factors in microcirculatory dysfunction. In clinical and experimental studies, early alterations of RBC occurred in sepsis and persistent RBC abnormalities were associated with mortality in intensive care unit [11, 24]. However, it is not known how early RBC abnormalities are expressed compared with various clinical manifestations used in sepsis-related organ failure assessment (SOFA) because of heterogeneous patients admitted to intensive care unit. This makes it difficult to be confident that RBC abnormalities is an early clinical indicator of sepsis.
Endotoxin induces septic shock in both mice and humans, and endotoxin-induced toxemia model is appropriate for the comparison of early phase of sepsis. The dose of LPS causing the death of 50% mice is known to be approximately 1–25 mg/kg [8]. Five out of eight rats died at 12 h after intraperitoneal administration of 20 mg/kg LPS and two out of eight rats at 8 h after LPS injection in this study.
Nevertheless, hemorheological differences exist in species and RBC aggregation in rats is almost undetectable unlike in human blood [34]. RBC aggregation is influenced by plasma factors such as concentration of plasma proteins and cellular factors including the affinity of RBC for macromolecules, RBC geometric factors, surface charge, and membrane and cytoskeletal composition. Animals with low erythrocyte aggregation have higher plasma fibrinogen concentrations than animals with high erythrocyte aggregation levels. To exclude the plasma factor, RBC was washed and re-suspended in PVP solution, and RBC aggregability, in other words, aggregation tendency related to RBC intrinsic factors, was measured in this study.
RBC aggregability increased starting from 4 h after LPS administration. T1/2 shortened more rapidly than change in AI values at 2 h after LPS injection. Shortened T1/2 indicates higher potential for aggregability. This finding was comparable to previous studies reporting decreased T1/2 at 2 h after LPS injection [35]. Increased RBC aggregability revealed marked alteration in cellular properties [5]. Activated leukocytes affected RBC biological and mechanical properties via proteolytic enzymes and oxygen-free radicals, and resulted in increased RBC aggregability [6].
However EI was statistically significant but slightly increased unlike most studies. EIs are affected by shear stress and temperature and increased with shear stress and decreased significantly with decrease in temperature [4, 30]. RBC deformability in sepsis patients has been reported to decrease by up to 10% compared to normal individuals on shear stress >10 Pa [11]. In a recent study, the reduction of erythrocyte deformability in patients with sepsis was lower than in patients without sepsis, but the extent was very small and did not correlate with the reduction of erythrocyte deformability and mortality [32]. On the other hand, there was no difference under 3 Pa, which is known as the shear stress value in microcirculation between septic patients and normal volunteers [11]. There is no study of shear stress levels that can best demonstrate the change in erythrocyte deformability in sepsis. Further studies are also needed to determine if changes in erythrocyte deformability affect the microcirculation with low shear stress in sepsis.
RBC abnormalities detected early in sepsis may not be specific findings. Trauma and hemorrhagic shock and non-septic patients resulted in increased RBC aggregation and decreased deformability [21, 32]. Clinical variables related to SOFA such as platelets and lactate, are also not specific to sepsis. However, they are closely associated with early detection of organ failure. SOFA is used for early detection in patients with suspected sepsis.
Platelet counts decreased rapidly after 4 h of LPS administration and appear to show a high degree of correlation with AIs, and T1/2 among other clinical values. Platelet counts were associated with poor clinical outcome, and platelet function was severely altered in septic patients [1]. The reduction of platelet counts was attributed to the adhesion of hypercoagulable platelets to the injured endothelium and platelet segregation in the microcirculation [33, 35]. Endothelial activation and debilitation is another important factor in microcirculatory dysfunction. Platelets are involved in endothelial activation in which platelet-leukocyte interaction and microthrombus formation by activated platelet are regarded as a mechanism in sepsis complications [10]. Platelet adhesion and aggregation were not confirmed in this study. However, platelet function abnormalities appear to be important as an early clinical indicator, such as RBC abnormalities.
In this study, platelet count was negatively correlated with P(v-a)CO2/C(a-v)O2, anaerobic metabolic indicator. Increased platelet aggregation leads to impaired microcirculation and increased P(v-a)CO2/C(a-v)O2 . Recently a new microfluidic system was developed for ex vivo monitoring of hemorheological changes, blood viscosity and platelet adhesion, and further study regarding platelet and RBC aggregation could be performed in this novel system [35].
Lactate increased starting at 2 h after LPS injection. Lactate is used in defining septic shock and increased lactate suggests tissue hypoperfusion [13, 25]. A recent study based on a rat model of sepsis using cecal ligation and puncture suggested lactate as a potential biomarker to identify the onset of sepsis [36].
The limitations of this study are as follows. First, LPS-induced endotoxemia is a specific type of sepsis and a single bolus of LPS in rats caused a transient and rapid systemic inflammatory reaction whereas sepsis in human exhibits a prolonged elevation in systemic inflammatory cytokine production. Second, SOFA was based on Glasgow coma scale to measure brain dysfunction and mean arterial pressure, or vasopressors for cardiac dysfunction. However, these valuables were not measured in this animal study. In a porcine model of fulminant sepsis, the heart rate/mean arterial pressure increased at 4 h after intravenous E.coli injection [22] and it was not assumed that this study missed the clinical end point of declining blood pressure. Third, we did not provide a range of cutoff values that could detect changes in erythrocyte aggregation. More research is needed in clinical practice.
Conclusion
RBC abnormalities based on clinical data obtained via SOFA appeared at an early stage in LPS-induced endotoxemia and represent important indicators of early clinical manifestations in sepsis. Altered RBC may be easily measured clinically as a point-of-care test. In addition, further studies that explore the association between RBCs and platelets or the cut-off value of erythrocytes abnormalities can provide additional insight into the microcirculation and organ failure in sepsis.
Declaration of interests
The authors declare that there is no conflict of interests.
Footnotes
Acknowledgments
This study was supported by Korea University grants and the Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Science, ICT, and Future Planning (No. NRF-2015R1A2A2A01006734).