
Abstract
OBJECTIVE:
To investigate the clinical value of dynamic contrast enhanced ultrasound (D-CEUS) in predicting the microvascular invasion (MVI) of hepatocellular carcinoma (HCC).
PATIENTS AND METHODS:
In this retrospective study, 16 patients with surgery and histopathologically proved HCC lesions were included. Patients were classified according to the presence of MVI: MVI positive group (n = 6) and MVI negative group (n = 10). Contrast enhanced ultrasound (CEUS) examinations were performed within a week before surgery. Dynamic analysis was performed by VueBox® software (Bracco, Italy). Three regions of interests (ROIs) were set in the center of HCC lesions, at the margin of HCC lesions and in the surrounding liver parenchyma accordingly. Time intensity curves (TICs) were generated and quantitative perfusion parameters including WiR (wash-in rate), WoR (wash-out rate), WiAUC (wash-in area under the curve), WoAUC (wash-out area under the curve) and WiPi (wash-in perfusion index) were obtained and analyzed.
RESULTS:
All of HCC lesions showed arterial hyperenhancement (100 %) and at the late phase as hypoenhancement (75%) in CEUS. Among all CEUS quantitative parameters, the WiAUC and WoAUC were higher in MVI positive group than in MVI negative group in the center HCC lesions (P < 0.05), WiAUC, WoAUC and WiPI were higher in MVI positive group than in MVI negative group at the margin of HCC lesions. WiR and WoR were significant higher in MVI positive group.
CONCLUSIONS:
D-CEUS with quantitative perfusion analysis has potential clinical value in predicting the existence of MVI in HCC lesions.
Keywords
Introduction
Hepatocellular carcinoma (HCC) is the most common primary malignant liver tumor [1]. Liver resection is one of the possibly curative treatments for HCC [2]. However, the recurrence rate after liver resection is reported as high as 70% which leads to poor prognosis and poor quality of life. Microvascular invasion (MVI) is an aggressive behavior of HCC and is proved to be an independent risk factor for recurrence of HCC [3]. MVI is defined microscopically as liver tumor cells invaded mainly small blood vessels lined by endothelium, such as portal vein branches [4]. A systematic review revealed the incidence of MVI was between 15.0% and 57.1% in surgical specimen [5]. Early and accurate prediction of MVI before surgery is of great significance for assessing the prognosis of HCC patients, selecting optimal clinical treatments, and formulating precise treatment plans.
The DEGUM multicenter study and the EFSUMB liver guidelines recommended contrast harmonic imaging using second generation contrast agents like Sulphur hexafluoride microbubbles has a high diagnostic accuracy for characterization and detection malignant liver lesions [6–8]. Depending on its unique advantages such as real time scan, non-radiation, repeatable and convenient, contrast enhanced ultrasound (CEUS) has been widely used in evaluating microcirculation blood perfusion of the HCCs [7, 8]. According to the most updated prospective multicenter DEGUM IV study, for HCC characterization, it is very important to evaluate the early irregular atrial hyper-enhancement and the wash out, often in the late phase [9].
Furthermore, dynamic contrast enhanced ultrasound (DCE-US) is a quantitative imaging technique bases on conventional CEUS [10]. By quantitative analysis of tissue perfusion and the pathophysiology of angiogenesis of benign and malignant focal liver lesions, DCE-US has been proved to have the potential for a better understanding of dynamic wash-in and wash-out process of CEUS. It could be helpful for the differentiation of cholangiocarcinoma and HCC [11]. As a cost effective, mobile, safe and repeatable imaging method, DCE-US analysis has also been used to make accurate quantification of tissue perfusion and to monitor changes induced by anti-angiogenic [12, 13] and anti-inflammatory [14–17] therapies, both as a potential marker of response and as a tool to enable dose optimization of therapy in individual patients [13, 18]. However, little has been published on the possibility of DCE-US in predicting MVI before surgical operations.
The purpose of our study is to investigate the potential clinical value of DCE-US in evaluating the MVI of HCC.
Patients and materials
Patients
From January 2020 to October 2020, 16 patients with histopathologically confirmed HCC lesions were retrospectively included from 2 university hospitals. The inclusion criteria were: 1) Patients with surgery and histopathologically confirmation HCC lesions; 2) patients who received CEUS examinations one week before surgery; 3) DICOM format of clips was available; and 4) the presence of MVI was confirmed by postoperative histopathologic results. The exclusion criteria were as following: 1) The HCC lesion was invisible during conventional B mode ultrasound scan; 2) patients lack of CEUS DICOM images; and 3) patients with contraindications to ultrasound contrast agent.
According to the final histopathological results, patients were separated into 2 groups, MVI positive group and MVI negative group.
This retrospective study was approved by was approved by the Ethics Committee of Zhongshan Hospital, Fudan University. And the informed consent was waived.
Ultrasound examinations procedure
Two experienced radiologists with more than 15 years’ experience of liver CEUS performed CEUS examinations with the awareness of the patients’ clinical histories. All ultrasound examinations were performed by experienced examiners using 3 high resolution ultrasound machines, two with a C1-6 convex array transducer (Acuson Oxana Siemens, LOGIQ E9 GE), one equipped C1-5 convex array transducer (Siemens Acuson Sequoia).
All patients enrolled in this study fasted for at least 8 hours before CEUS examinations. During the B-mode ultrasound (BMUS) scanning of the whole liver, the location, size and margin of HCC lesions were observed. After the bolus injection of 1.5–2.4 ml Sulphur hexafluoride microbubbles (SonoVue/Lumason, Bracco) via the cubital vein and followed by a 5–10 ml saline flush. According to current liver CEUS guidelines, the enhancements feature of HCC lesions during arterial phase, portal venous phase and late phases were recorded and observed [7, 8]. A clip at least 2 minutes which displaying the enhancement process of suspected HCC lesions was recorded continually without the movement of the transducer. CEUS data were recorded and exported in DICOM format as Cine loops for independent reading by one experienced examiner.
Dynamic contrast enhanced ultrasound (DCE-US) quantitative analysis
The contrast clips were analyzed using the perfusion CEUS software (VueBox®/Bracco, Geneva) by an independent operator who was not informed of the patients’ clinical histories or the results of other imaging modalities. CEUS clips were observed dynamically. Three individually for the tumor size adapted regions of interests (ROIs) were placed in the center of HCC lesions; at the margin of HCC lesions and in the surrounding liver parenchyma accordingly [Fig. 1]. In order to reduce the breath motion artifact, the motion compensation function was used. A time-intensity curve (TICs) was then generated, which displayed the average intensity in a ROI as a function of time, reflecting the transit of the ultrasound contrast agents. The TIC describes the dynamic process of wash-in and wash-out of the contrast microbubbles in the ROI.
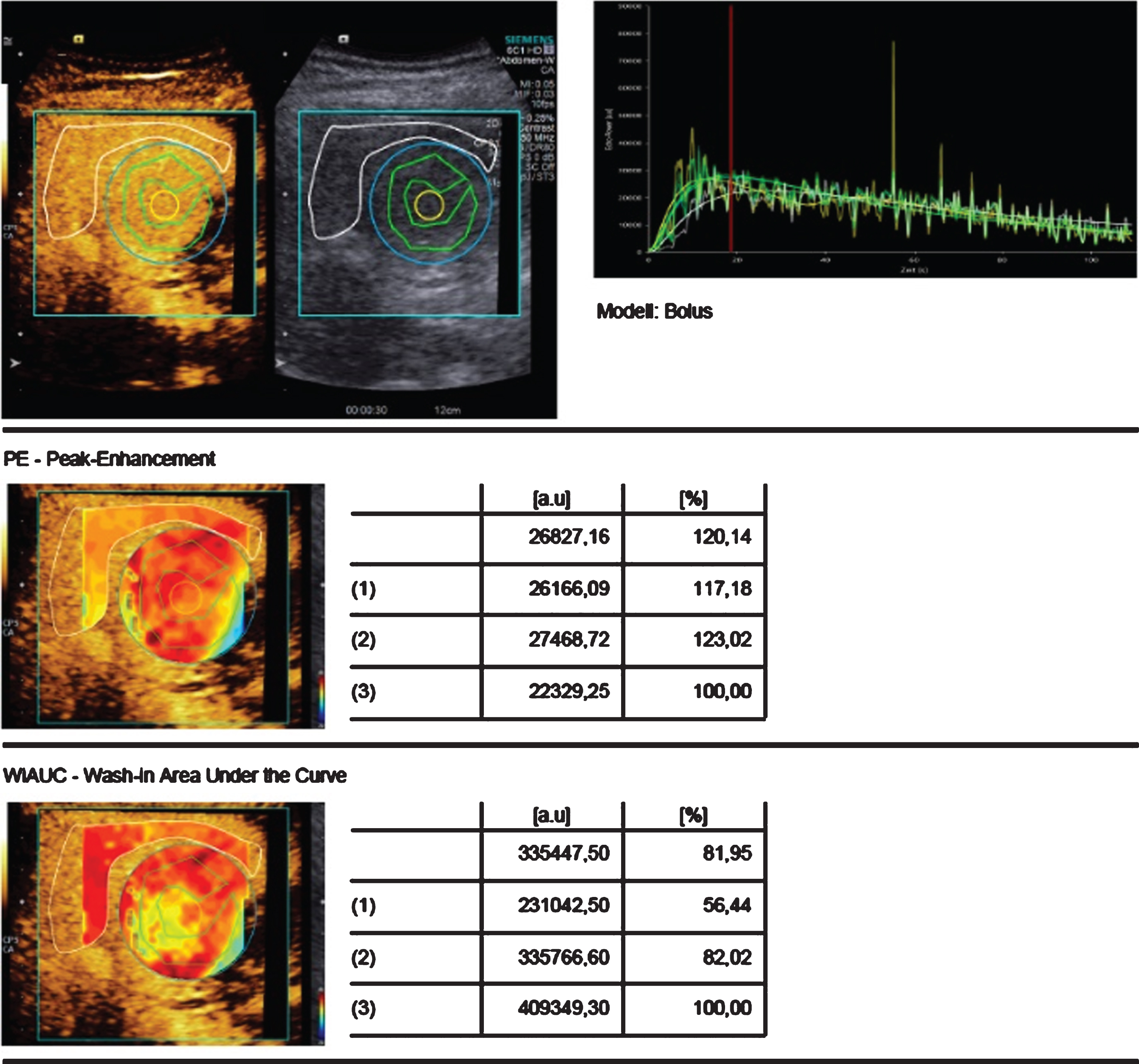
DCE perfusion analysis using the VueBox® of histopathological proven HCC. Regions of interest (ROIs) were set in the center, at the margin in comparison to the surrounding liver tissue. In false color coded in red and yellow irregular hyper-enhancement. Curve analysis with early wash in (peak) and wash out, as criteria for malignancy.
The fitting results were considered credible when the quality of fit > 75%. CEUS quantitative parameters were extracted as follows: WiR (wash-in rate, the maximum slope of the TIC represented as a tangent at the ascending part of the curve), WoR (wash-out rate, the minimum slope of the curve, represented as a tangent at the descending part of the curve), WiAUC (wash-in area under the curve, area under the TIC from time of arrival to the peak enhancement), WoAUC (wash-out area under the curve, the area under the TIC from the peak enhancement to the end of the curve) and WiPI (wash-in perfusion index, WiPI = WiAUC/rise time) [19].
Continuous variables used Student t-test or Mann-Whitney U-test when it’s appropriate. All data were calculated using the software program SPSS Statistics 22.0 (IBM, Armonk, USA) and GraphPad Prism 7 (GraphPad Software, Inc.). P value < 0.05 was considered statistically.
Results
Patients characteristics
The enrolled patients were 12 males and 4 females, with a mean age of 57.9 years (standard deviation, 11.3). Among the enrolled patients, there were six HCC lesions with MVI positive and 10 HCC lesions with MVI negative. Most of the HCC lesions were located in the right lobe of liver (81.2%) with single HCC lesions [Table 1].
Baseline characteristics of patients
Baseline characteristics of patients
On CEUS, all HCC lesions were characterized as an obviously hyperenhanced lesion in arterial phase, and 12/16 (75%) of HCC were characterized as hypoenhanced lesions in the portal venous and late phases. During the arterial phase of CEUS, 93.7% (15/16) of HCC lesions displayed homogeneous hyperenhancement.
Dynamic contrast enhanced ultrasound (DCE-US) quantitative analysis
Further DCE-US and quantitative analysis demonstrated reliable results using VueBox of all HCC lesions with quality of fit exceeding 75%. While comparing between MVI positive and MVI negative group, the WiAUC and WoAUC in HCC lesions were significantly different (P < 0.05) [Fig. 2].
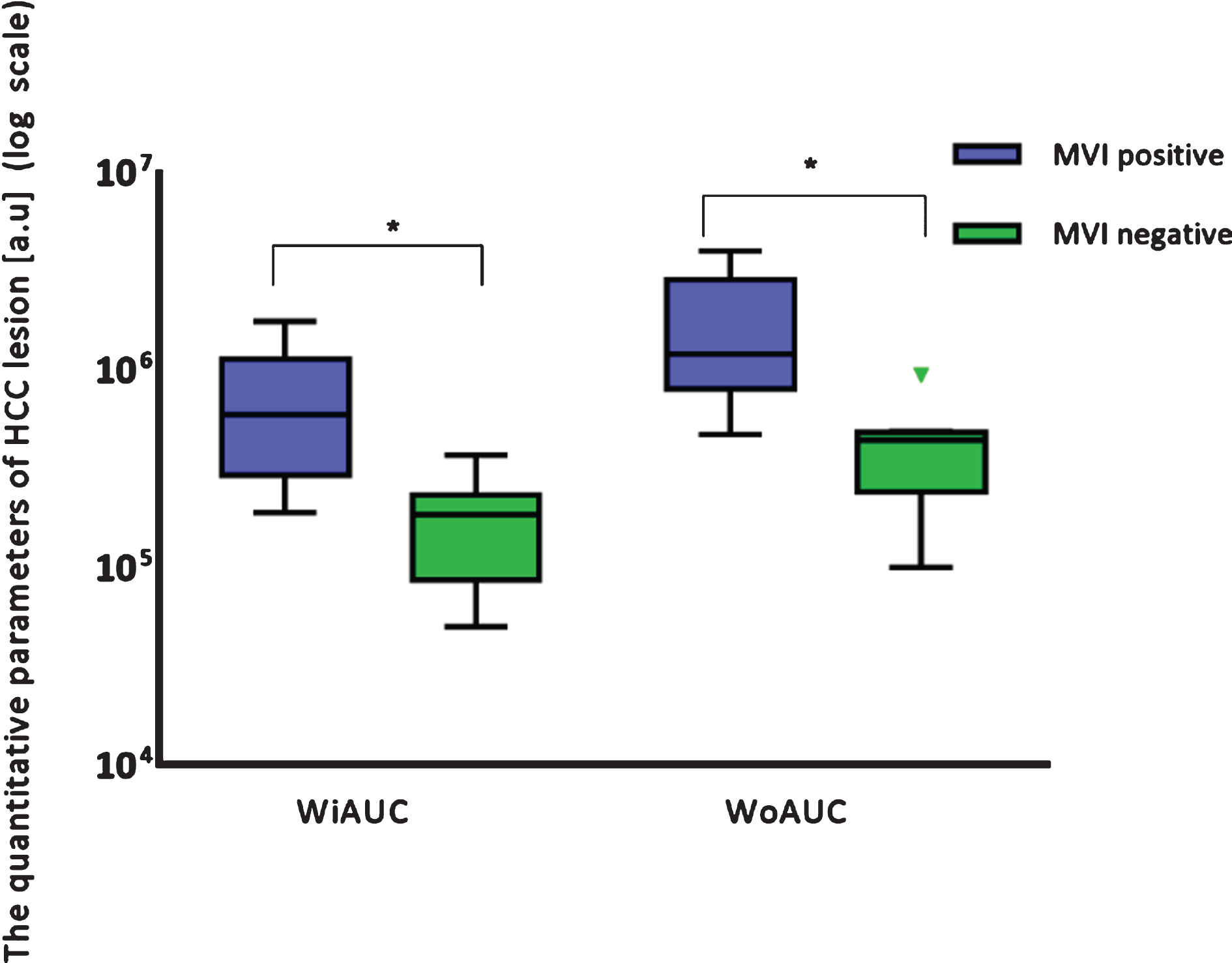
Dynamic contrast enhanced ultrasound (DCE-US) and quantitative parameters of hepatocellular carcinoma (HCC) lesions. Among all DCE-US quantitative parameters, the wash-in area under the curve (WiAUC) and wash-out area under the curve (WoAUC) were higher in microvascular invasion (MVI) positive group than in MVI negative group (P < 0.05).
Also, while set ROIs in the margin area of HCCs, significant difference could be found between MVI positive and MVI negative group in several DCE-US parameters. WiAUC, WoAUC and WiPI were higher in microvascular invasion (MVI) positive group than MVI negative group (Fig. 3).
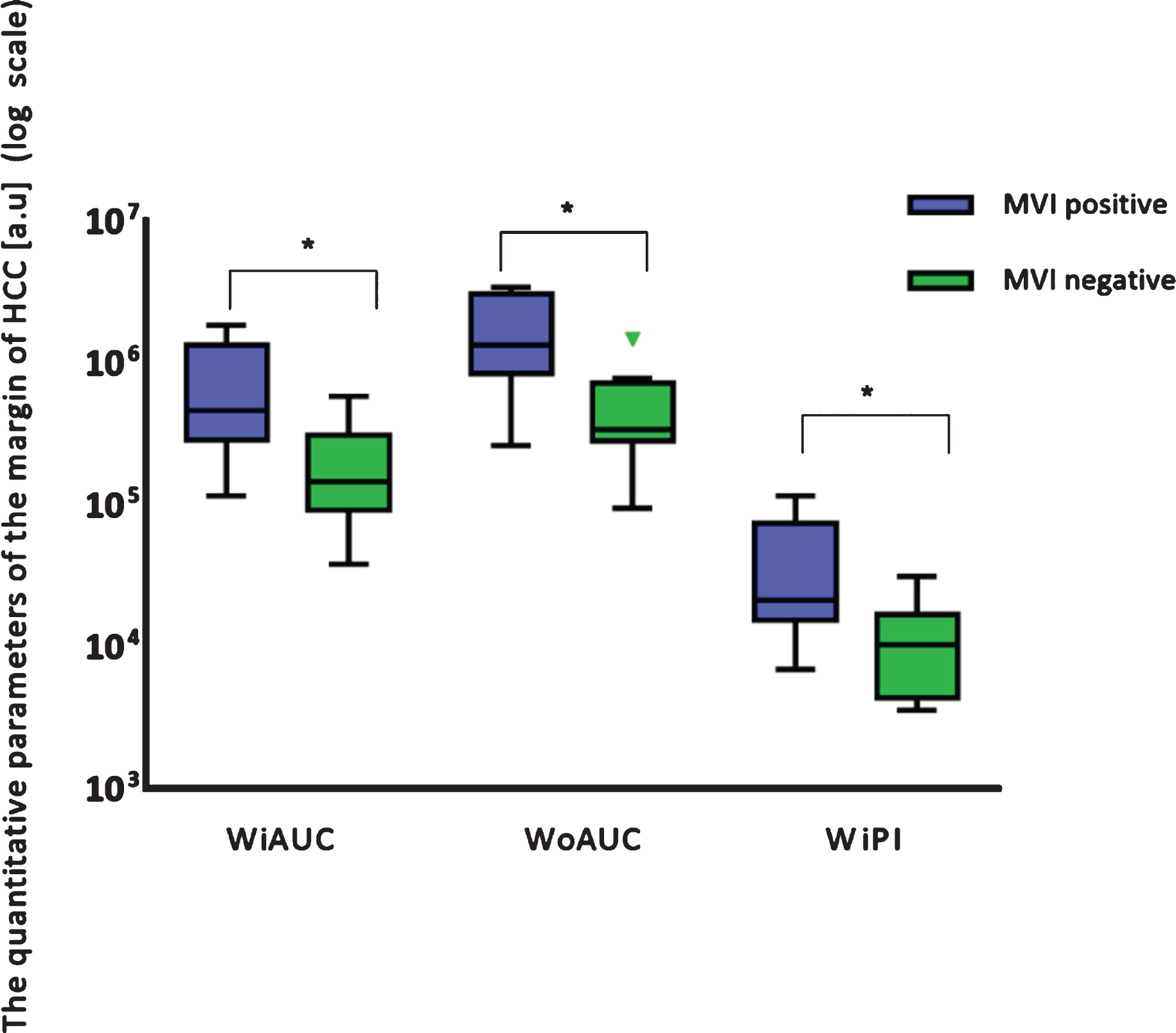
Comparison between the dynamic contrast enhanced ultrasound (DCE-US) quantitative parameters in the margin area of hepatocellular carcinoma (HCC) lesions. The wash-in area under the curve (WiAUC), wash-out area under the curve (WoAUC) and wash-in perfusion index (WiPI) were higher in microvascular invasion (MVI) positive group than MVI negative group (P < 0.05).
In MVI positive group, DCE-US quantitative parameters including WiR and WoR were significantly difference between the ROIs set in the margin area of HCC lesions and in the surrounding liver parenchyma [Fig. 4]. However, no significant difference could be found between the margin area of HCC lesions and its surrounding liver parenchyma in MVI negative group.
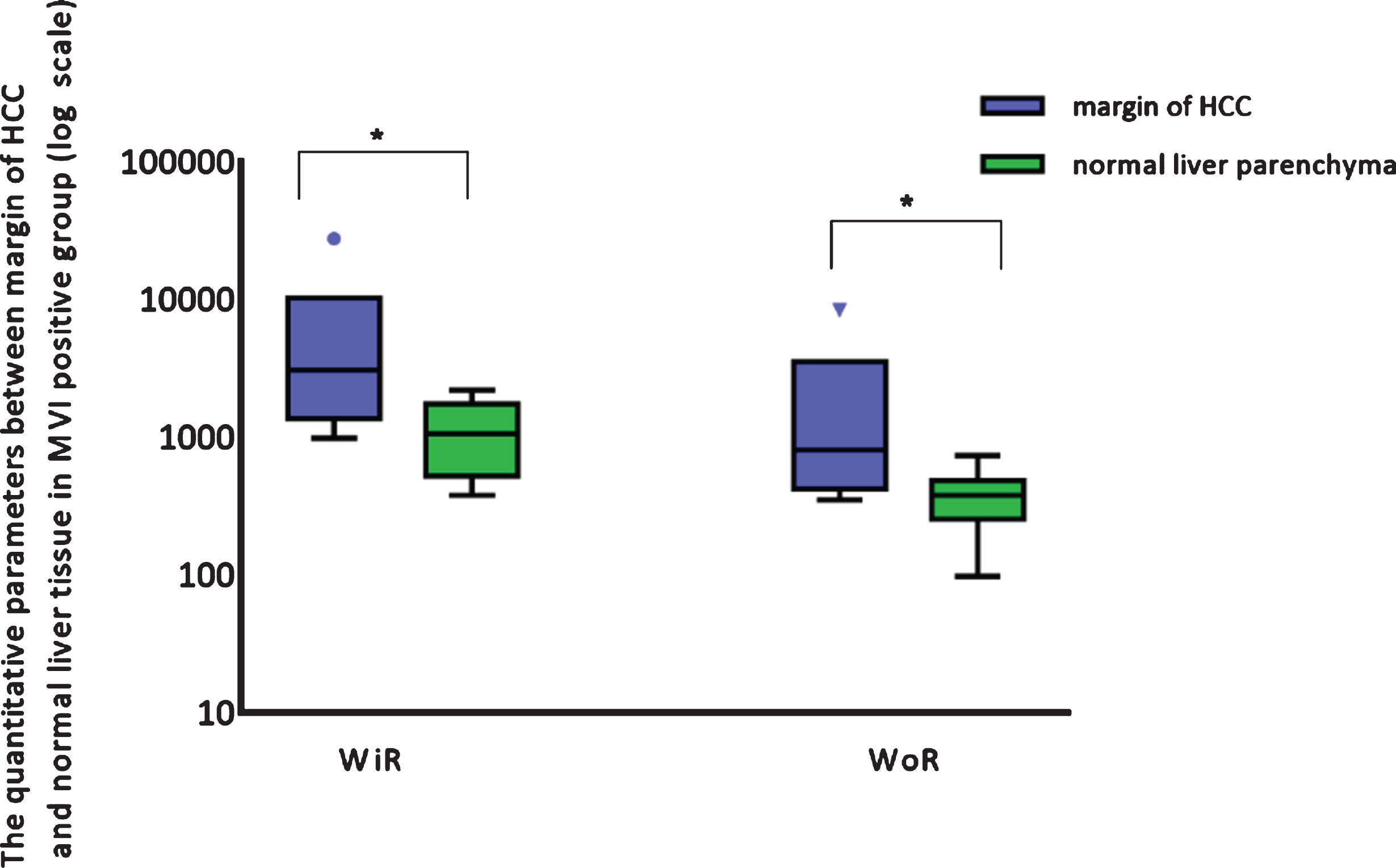
Comparison between the dynamic contrast enhanced ultrasound (DCE-US) quantitative parameters between the margin area of hepatocellular carcinoma (HCC) lesions and its surrounding liver parenchyma in MVI positive group. In MVI positive group, the wash-in rate (WiR) and wash-out rate (WoR) was significantly higher in the margin of HCC lesions than in the surrounding liver parenchyma.
Indicator dilution techniques may be used for the quantification of macro- and microvascular blood flow in HCC lesions [20, 21]. CEUS perfusion imaging was evaluated before for differentiation CCC and HCC lesions. Typical for HCC lesions with more than 15 mm in size is an irregular arterial hyper enhancement and prolonged wash out in the late phase, CCC showed earlier wash out [11, 22]. Previously reported studies suggested the preoperative imaging modalities such as computed tomography (CT) [23] and magnetic resonance imaging (MRI) [24] in predicting MVI. The use of these techniques allows for the estimation of blood flow parameters of tumors and organs. However, in contrast to SonoVue®, which is a strictly intravascular agent, CT and MRI contrast agents show extravascular distribution, limiting such methods in measuring blood flow using multi-compartmental models.
In early experience, DCE-US is very helpful for post intervention treatments control after transarterial chemoembolization (TACE) and ablation therapies of HCC lesions, such as radiofrequency ablation (RFA), microwave ablation (MWA) and irreversible electroporation (IRE) [25–27]. In comparison to contrast enhanced MRI, DCE-CEUS has a very high diagnostic accuracy HCC lesions also if liver specific contras agent for MRI was used [28, 29]. Currently, DCE-US is considered to be reliable to identify relative dynamic changes of these quantitative parameters. It was reported that some DCE-US perfusion parameters representative for perfusion during arterial phase, including the PE, WiAUC and WiR. Those parameters could be used to evaluate the therapeutic efficacy of HCC by the hemodynamical change [30]. DCE-US perfusion parameters such as WoAUC and WoR were also reported to be useful in distinguishing fibrotic and inflammatory lesions of Crohn’s Disease [19].
Pathologically, MVI first invades the capsule of HCC and then to the surrounding blood vessels of HCC lesions. The margin area of HCC lesions is considered to be the most prone place for MVI [3, 31]. In our study, while comparing the difference in blood perfusion between areas in the margin of HCC and the surrounding liver parenchyma, significant difference was reached in several DCE-US quantitative parameters, such as WiR and WoR among MVI positive group and MVI negative group. Based on the hemodynamic evaluations of areas between the margin of HCC lesion and the surrounding liver parenchyma, it might have the potential in prediction of MVI before surgery [31].
During the pathological process of MVI, the HCC tumor cells progressively increase and gradually destroy the surrounding parenchyma structure of HCC lesions [3]. HCC invasion of blood vessel leads to the formation of arteriovenous fistulas, resulting in increased and faster blood flow perfusion. In our result, while comparing between MVI positive group and MVI negative group, DCE-US quantitative parameters, such as WiAUC and WoAUC in the margin area of HCC lesion were significantly higher in the MVI positive group. This could be explained by the invasion effect in the MVI positive group. Moreover, inner HCC lesions, the WiAUC and WoAUC had significant difference between MVI positive and MVI negative group. These hemodynamic changes also could be results of HCC invasion process into the surrounding parenchyma.
In recent years, researches also focused on using radiomics approaches in predicting of MVI [32–35]. In one of our previous study, we reported that radiomic based on grayscale ultrasound images could provide additional information for the preoperative prediction of the presence of MVI [36]. Moreover, radiomics analysis based on multi-parametric ultrasound images including B-mode, shear wave elastography, and shear wave viscosity imaging may have a potential method to predict the MVI of the HCC patients [34]. However, since radiomics approaches depend on artificial intelligence and deep learning methods, it is still limited in daily clinical use.
There have several limitations of this study. Small sample size and retrospective study are the main limitations. Prospective large scale multicenter study in evaluating the presence of MVI of HCC should be performed in the future.
Conclusion
The DCE-US with quantitative analysis has the potential to predicting MVI in HCC lesions in future diagnosis. WiAUC and WoAUC might be valuable quantitative parameters.