
Abstract
OBJECTIVE:
To explore the correlation between two-dimensional ultrasound (2D-US), contrast-enhanced ultrasound (CEUS) and microvascular invasion (MVI) in hepatocellular carcinoma (HCC).
METHODS:
In this retrospective study, 56 patients with surgically pathologically confirmed HCC lesions were included. Patients were classified according to the presence of MVI: MVI positive group (n = 17) and MVI negative group (n = 39). 2D-US and CEUS examinations were performed within two weeks before surgery. The 2D-US and CEUS features were analyzed for correlation with MVI. Statistically significant parameters of ultrasound characteristic were scored, and the results of the scores were analyzed by ROC curve.
RESULTS:
There were statistically significant differences in tumor shape, boundary, capsule, CEUS portal phase and delayed phase enhancement pattern, time to wash out, and tumor margin after enhancement (P < 0.05), while there were no statistically significant differences in tumor location and size, CEUS arterial phase enhancement pattern, initial time, time to peak, and peritumor enhancement (P > 0.05). When diagnosing the presence of MVI in HCC patients with cut-off value of the score combined 2D-US and CEUS features≥3, the maximum Jorden index was 0.58, and its diagnostic sensitivity and specificity were 94.10% and 64.1%, respectively, meaning that the total score≥3 was highly suspicious of the presence of MVI.
CONCLUSIONS:
2D-US and CEUS are feasible methods for preoperative prediction of MVI in HCC, and can provide some theoretical basis for individualized clinical treatment.
Keywords
Introduction
Hepatocellular carcinoma (HCC) has a high morbidity and mortality rate [1, 2] and a poor prognosis [3, 4] around the world. Radical surgical resection is one of the main treatment methods, and the way of surgical resection is closely related to the prognosis, some studies have shown [5] that the recurrence rate of patients after non-anatomical hepatectomy is significantly higher than that of anatomical hepatectomy. Microvascular invasion (MVI) is an indicator of tumor aggressiveness and has a predictive effect on the prognosis of hepatocellular carcinoma. The risk of postoperative recurrence in patients with MVI positive is 4.4 times higher than that in MVI negative patients [6]. It has been reported in the literature that the presence of MVI in HCC requires intraoperative resection of the tumor with anatomically larger margins or postoperative adjuvant embolization chemotherapy, and patients with narrow margins have a higher recurrence rate and poorer overall survival compared to those with wider margins (> 1 cm) [7]. However, it is difficult to accurately evaluate HCC MVI before operation, and preoperative puncture biopsy can obtain liver tissue for pathological diagnosis, but it is easy to be misdiagnosed and missed, and may cause tumor implantation and intra-abdominal bleeding. Therefore, HCC MVI can generally only be detected by postoperative histopathological examination of tumor specimens [8, 9], but there is a certain diagnostic lag in postoperative pathological results. Contrast-enhanced ultrasound (CEUS) can show the microvascular perfusion of the tumor with a high sensitivity and a strong cross-modality comparability to histopathology [10], showing a high diagnostic accuracy in assessing HCC compared to corresponding results from MRI scans [11]. Some studies [12, 13] have shown that CEUS with quantitative perfusion analysis has potential clinical value in differentiating malignant tumors and predicting the existence of MVI in HCC lesions. The purpose of this study is to explore the correlation between 2D-US, CEUS features and MVI in HCC, in order to help clinicians choose the best treatment through preoperative non-invasive evaluation, so as to improve the prognosis of patients.
Materials and methods
The object of study
The clinical and preoperative 2D-US and CEUS data of patients who underwent hepatectomy and pathologically diagnosed HCC in our hospital from January 2019 to December 2020 were analyzed retrospectively. The inclusion criteria were as follows: (1) postoperative pathological results clearly indicated the existence of MVI; (2) CEUS within 2 weeks before operation; (3) single tumor; (4) no preoperative radiotherapy, chemotherapy, targeted therapy and other treatment. The exclusion criteria were as follows: (1) obvious portal vein tumor thrombus formation in preoperative imaging syndrome; (2) signs of intrahepatic or extrahepatic metastasis; (3) history of other malignant tumors; (4) loss of clinical and contrast-enhanced ultrasound image information; (5) poor image quality. According to the inclusion and exclusion criteria, 56 patients with HCC confirmed by pathology were enrolled in the group. There were 44 males and 12 females, aged 29–68 (52.590±7.903) years. In this study, all the patients signed the informed consent form before receiving CEUS examination.
Instruments and methods
CEUS was performed in low mechanical index mode using Philips IU22/ EPIQ 7 and Siemens ACUSON Sequoia color Doppler ultrasound diagnostic instruments with convex array probes C5-1 and 5C1 (both at 1–5 MHz), respectively, and the contrast agent was Sulphur-hexafluoride microbubbles (SonoVue, Bracco Imaging, Milan, Italy).
The patients took horizontal position or left supine position, scanned the liver routinely and selected the best section of the lesion. Then the contrast agent SonoVue was added to 5.0 ml saline to make microbubble suspension, and the microbubble suspension was mixed repeatedly for 30 seconds. According to the instrument and the body weight of the patients, 1.0–2.0 ml microbubble suspension was withdrawn and injected into the elbow vein followed by tail injection of 5 ml saline. While recording the time, the lesion was dynamically observed in real time for 4–6 min continuously and the images were stored in CEUS mode.
Data analysis
The general clinical information of the patients such as gender, age and serum alpha-fetoprotein values were routinely recorded. The images were analyzed by two doctors with more than 5 years’ experience in abdominal CEUS diagnosis using an independent blind method to record 2D-US and CEUS features of the lesion. The final diagnosis was made by a third physician with more than 10 years of experience in the diagnosis of abdominal CEUS when interobserver diagnostic opinions differed.
The capsule types of tumors can be divided into three type [14] (Fig. 1): (A) complete capsule: the tumor capsule is well continuous without obvious interruption; (B) incomplete capsule: the tumor capsule is defective with poor continuity; and (C) no capsule. The tumor capsule showed as a peritumor hypoechoic halo on 2D-US. Wash out refers to the lesion showing high enhancement in the arterial phase and low enhancement changes in the portal phase as well as the delayed phase. Enhanced tumor margins are classified as smooth or non-smooth. In the contrast state, a smooth margin is defined if the lesion shows a regular round or round-like shape in all views during the scan, while a non-smooth margin is defined if some views show burr-like or crabfoot-like protrusions or poorly demarcated from the surrounding area. Peritumoral enhancement [14] refers to patchy or crescent enhancement around the lesions in the arterial phase and equal enhancement in the portal phase or delayed phase.

Capsule types of tumor. A. The capsule is complete, B. The capsule is incomplete, C. No capsule.
The included subjects were divided into MVI-positive and MVI-negative groups based on the surgical pathological findings.
SPSS Statistics 25.0 was applied for statistical analysis, and P < 0.05 was considered as the difference was statistically significant. The measurement data were expressed as
Results
The general condition of the patients and the characteristics of the lesions
According to the surgical and pathological findings, a total of 56 HCC patients were enrolled in this study, of which 39 cases were positive for MVI and 17 cases were negative for MVI. The general conditions and lesion characteristics of the patients in both groups are shown in Table 1. There were no statistically significant differences in age, gender, lesion location and size, and serum alpha-fetoprotein values (P > 0.05).
General information of patients and characteristics of lesions. (N(%)/
)
General information of patients and characteristics of lesions. (N(%)/
Compared with the MVI-negative HCC, the irregular shape, unclear boundary and incomplete capsule of the tumor in the MVI positive HCC were higher than those in the MVI-negative HCC, with statistically significant differences (P < 0.05), as shown in Table 2.
Comparison of two-dimensional ultrasound features between MVI- positive and MVI -negative HCC (N(%) /
)
Comparison of two-dimensional ultrasound features between MVI- positive and MVI -negative HCC (N(%) /
Compared with MVI-negative HCC, there were statistically significant differences in enhancement levels in the portal and delayed phases of CEUS, time to washout, and enhanced tumor margin in MVI-positive HCC tumors (P < 0.05), while there were no statistically significant differences in enhancement levels in the arterial phase, initial time, time to peak, and peritumor enhancement (P > 0.05). In the final CEUS LI-RADS classification, LR-M was seen more often in MVI-positive patients compared to MVI-negative patients (58.82% vs 25.64%), and the difference was statistically significant (P = 0.017 < 0.05), as shown in Table 3.
Comparison of CEUS features between MVI-positive and MVI-negative HCC.(N(%) /
)
Comparison of CEUS features between MVI-positive and MVI-negative HCC.(N(%) /
Compared with MVI-negative HCC, MVI-positive HCC tumors are more rapidly washed out, and most of the lesions in the portal phase are less intensified and appear significantly hypoenhanced, while the MVI-negative tumors are more slowly washed out, and the reduction in the degree of enhancement is not obvious. In the delayed phase, the enhancement degree of most lesions decreased, as shown in Fig. 2 and Fig. 3.
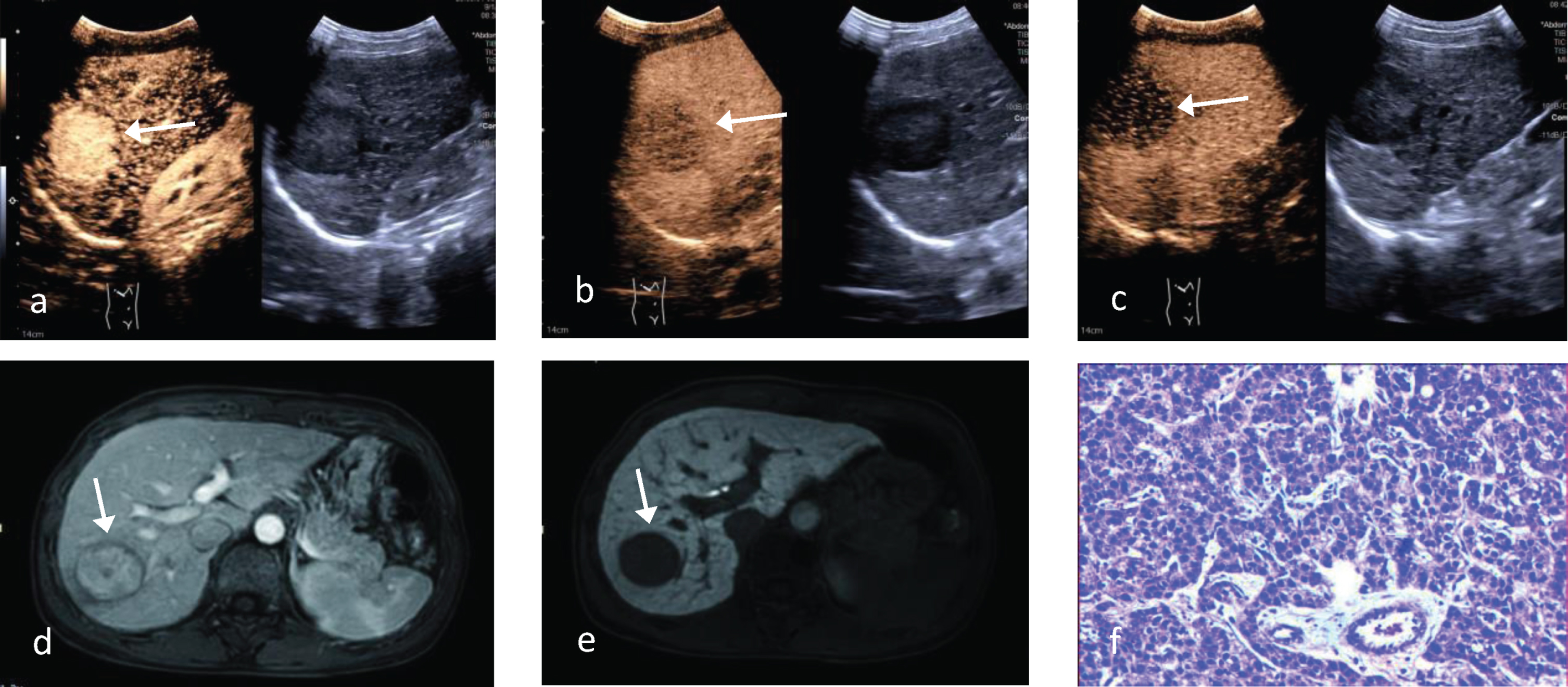
CEUS features of MVI-positive HCC. The patient, a 55-year-old female, had a hypoechoic lesion in the right lobe of the liver that showed inhomogeneous hyperenhancement in the arterial phase (17s) of CEUS and the tumor margin was not smooth (a), in the portal phase (68s) when the contrast began to fade and showed inhomogeneous hypoenhancement (b), in the delayed phase (127s) when the contrast continued to fade and showed inhomogeneous more hypoenhancement (c). d-e) Contrast-enhanced MRI imaging: Nearly complete tumor capsule but unsmooth margin. f) Histopathology imaging (x100).
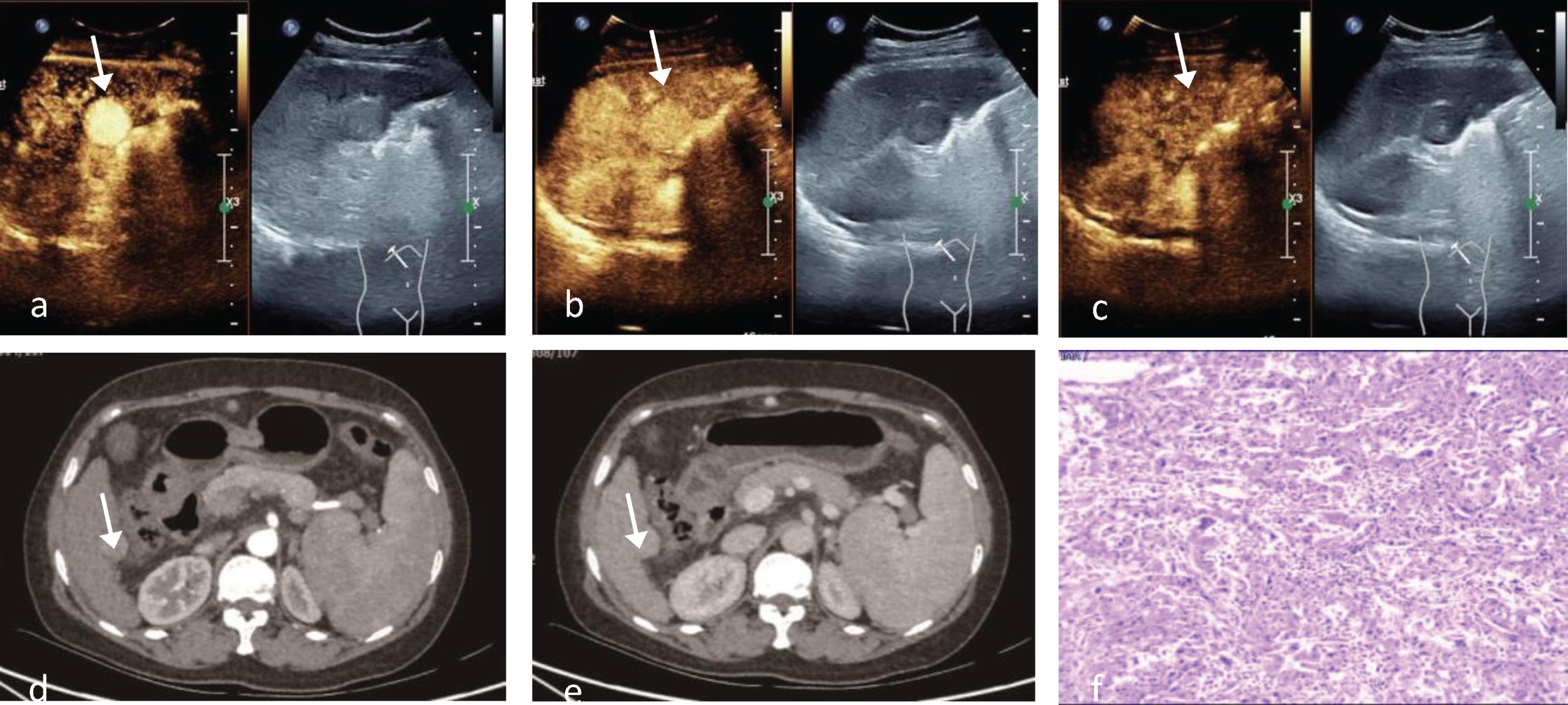
CEUS performance in MVI-negative HCC. The patient, male, 46 years old, showed a homogeneous hyperenhancement of isoechoic lesion in the left lobe of the liver in the arterial phase (25s) with smooth tumor margin(a), slightly hyperenhancement in the portal phase (74s) (b), and isoenhancement in the delayed phase (131s) without significant fading of the contrast (c). d-e) Contrast-enhanced CT imaging: smooth tumor margin; hyperenhancement in the arterial phase (d); isoenhancement in the delayed phase (e). f) Histopathology imaging (x100).
The statistically significant indexes in results 3.2 and 3.3 above were jointly scored: irregular shape, unclear boundary, incomplete capsule, enhancement pattern of “high enhancement in arterial phase - low enhancement in portal phase and delayed phase” and enhanced unsmooth tumor margin were scored as 1 point, totaling 5 points (Table 4), and the ROC curve was plotted for the score (Fig. 4). The results: the maximum Jorden index was 0.582 when the score was more than 3scores, and the sensitivity, specificity and AUC were 94.10%, 64.10% and 0.849 (95% confidence interval: 0.749∼0.949), which means that the presence of MVI in HCC was highly suspected when three or more of the statistically significant indicators were met.
HCC MVI score results of 2D-US combined with CEUS in qualitative diagnosis
HCC MVI score results of 2D-US combined with CEUS in qualitative diagnosis

ROC curve of HCC MVI score in qualitative diagnosis of 2D-US combined with CEUS.
MVI is the most important independent risk factor affecting recurrence and survival of hepatocellular carcinoma patients after radical resection [15]. MVI refers to the nesting masses of cancer cells seen microscopically in the lumen of the endothelium-lined vessels, mostly in the small branches of the portal vein within the paracancerous liver tissue, followed by branches of the hepatic veins, and less frequently in the hepatic arteries, bile ducts, and lymphatic vessels [16]. However, postoperative pathology suggests a degree of lag in MVI. If the MVI of HCC can be predicted before surgery, it can help to plan the surgery and select the best treatment method to improve the prognosis. Several studies around the world have reported [17] the use of CT, MRI, PET and other imaging examinations for MVI prediction, and preoperative imaging to assess the presence of MVI in hepatocellular carcinoma is considered to be a reliable method, but as far as ultrasound is concerned, its correlation with MVI in hepatocellular carcinoma is less studied. CEUS is an emerging imaging technology that can display tumor microblood perfusion, with the advantages of safe and non-radiation, low price, reproducibility, and real-time dynamic observation. This study focuses on the correlation between 2D-US and CEUS features and HCC MVI, with the aim of preoperative prediction of HCC MVI before operation, so as to provide a new and more valuable imaging basis for clinical selection of surgical procedure and optimal treatment.
The results of this study showed that the differences in lesion shape irregularity, unclear boundary, incomplete capsule, and enhanced unsmooth tumor margins were statistically significant in the MVI-positive compared with the MVI-negative HCC (P values were 0.008, 0.001, 0.039, and 0.005, respectively). Kanai et al. [18] divided HCC into single nodular type, single nodular type with peripheral protuberance and multinodular fusion type according to their morphology. many studies found that mononodular type with extranodular growth and multinodular type had an increased risk of MVI and poor prognosis [19–21]. The tumor capsule [22] is pathologically a layer of fibrous capsule formed due to fibrosis caused by tumor swelling growth compressing the surrounding liver tissues, which to some extent limits tumor invasion and spread of metastasis. When the capsule of hepatocellular carcinoma is incomplete, it suggests increased tumor invasiveness and significantly increased risk of MVI. In this study, 64.71% of MVI-positive HCC showed incomplete capsule and 82.35% showed unclear boundary, but some MVI-positive HCC showed complete capsule and clear boundary, which may be related to the degree of tumor differentiation and invasion, when the tumor tissue did not break through the capsule or early infiltration, it could show complete capsule and clear boundary. There was no statistically significant difference between the two groups in terms of tumor location, size, echogenic type and internal necrosis (P > 0.05). Previous studies [23] showed that tumor size was closely correlated with prognosis. In this study, there was no significant correlation between tumor size and MVI. The reason may be that the sample size is small and there is a certain subjective deviation in determining the maximum section by ultrasound, resulting in errors in tumor diameter measurement.
The liver is supplied by both portal vein and hepatic artery. Normal liver parenchyma is predominantly supplied by portal vein (about 75%) while hepatic carcinoma is predominantly supplied by hepatic artery, and CEUS performance can reflect the microvascular perfusion of tumor lesions. A prospective multicenter study [24] showed the excellent diagnostic accuracy of CEUS for the noninvasive diagnosis of HCC in high-risk patients. The results of this study showed that MVI-positive HCC showed low enhancement in the portal and delayed phases of CEUS, and previous studies [25] found that MVI in hepatocellular carcinoma is associated with low tumor differentiation, and the proportion of portal blood supply in hypofractionated hepatocellular carcinoma is lower, so the degree of enhancement in the portal and delayed phases is significantly lower than that in the liver parenchyma. In addition, hypofractionated hepatocellular carcinoma is often associated with arteriovenous fistulae, which makes contrast contouring more rapid [26]. Therefore, compared with MVI-negative HCC, MVI-positive HCC has a faster wash-out, and most of the lesions in the portal phase have a reduced degree of enhancement and appear significantly hypoenhanced, while MVI-negative HCC has a slower wash-out and no obvious decrease in enhancement. In addition, the quantitative analysis of CEUS enhancement phase of HCC showed that there was no significant difference in the time to enhancement and time to peak of quantitative parameters between MVI-positive and negative HCC; while the time to washout of MVI-positive HCC was significantly shorter, which also corroborated the above results. Early washed-out is a specific feature of LR-M class lesions, while MVI-positive HCCs was more rapidly washed-out compared to MVI-negative HCCs, suggesting a correlation between LR-M and the presence of MVI. A study [24] showed that CEUS LI-RADS has high diagnostic efficacy for HCC, but whether it can be used to predict microvascular invasion still needs to be further explored in the future. The non-smooth tumor margin [18] is considered to be the biological tendency of HCC to invade the tumor capsule and protrude to the non-tumor parenchyma, and it is most common in the extranodal extension. CEUS can more clearly show whether the margin of the lesion is smooth after enhancement, which can reflect the presence of MVI to a certain extent. Some studies reported [27] that HCC exhibited peritumoral enhancement on MR images showing an increased risk of microvascular invasion [28] whereas Chou et al. [14] found that CT presentation of peritumoral enhancement was not an important risk factor for MVI in HCC, and there was no significant correlation between CEUS peritumoral enhancement and MVI in this study, considering that it may be due to differences between different imaging modalities, and the relationship between peritumoral enhancement on CEUS images and MVI needs to be further explored.
In this study, 2D-US combined with CEUS was used to predict MVI in HCC, and the above 2D-US and CEUS features associated with MVI were further scored together. 3 score was the best score cutoff value, that is, the presence of MVI was highly suspected when three or more of the five statistically significant indicators were met, with a high diagnostic sensitivity of 94.10% and specificity of 64.10%, respectively. Therefore, it can provide a basis for early diagnosis of MVI in HCC in clinical work.
In summary, there is a certain correlation between HCC MVI and 2D-US and CEUS performance. 2D-US and CEUS can be used to evaluate HCC MVI preoperatively to provide more imaging basis for individualized clinical treatment.
This study has the following limitations: (1) the correlation between the degree of differentiation and microvascular invasion was not analyzed because there were results of “high-medium differentiation” and “medium-low differentiation” in this study; (2) The number of cases enrolled in this study after screening according to the inclusion and exclusion criteria was small and it was a single-center study, which may cause a degree of selective bias.