
Abstract
BACKGROUND:
In recent years, follow-up after breast reconstruction with silicone implants and the detection of complications have been relieved by the possibility of improved diagnostic methods.
METHODS:
Between January 2015 and December 2019 a total of 40 patients (29–84 years) with silicone implants were included in this retrospective study. The implants were examined clinically and with modern imaging: general ultrasound imaging (US), magnetic resonance imaging (MRI), high resolution computed tomography (CT) and positron emission tomography –computed tomography (PET-CT). If necessary, a histological/cytological sample was taken. The breast implants were assessed by three radiologists specialized in breast imaging. The grade of capsular contracture was classified according to the Baker classification.
RESULTS:
All 40 women obtained a clinical examination and an US diagnostic to identify early and more common complications such as implant folding and capsular fibrosis. Depending on the clinical examination and ultrasound findings additional MRI (n = 10), CT (n = 9) and/or PET-CT (n = 2) were performed. 16 patients had implants folding proven with US (n = 16), MRI (n = 6) and CT (n = 1). The grade of capsular fibrosis was determined according to the Baker classification. The following results were obtained in our study: 25 breast implants with Baker grade I and eleven breast implants with Baker grade II, both proven with US; one breast implants with Baker grade III and one breast implant with Baker grade IV, proven with US (n = 2), MRI (n = 1) and CT (n = 1). One patient had intracapsular rupture and one patient had extracapsular rupture, both detected on CT and surgically proven. No patient had a silicone accumulation in the lymph nodes. One patient had pathologically enlarged axillary lymph nodes, which were evaluated as inflammatory changes in PET-CT. Long-term complications such as the development of malignant breast tumors could not be observed.
CONCLUSION:
To detect early complications after breast implant surgery, a regular clinical examination is indispensable. Imaging methods complement each other and if they are used multimodal, it is easier to identify early complications. Modern diagnostic modalities like ultrasound and magnetic resonance imaging expand the spectrum and improve diagnostic safety.
Introduction
Breast reconstruction is one of the most common operations for many women diagnosed with breast cancer or for aesthetic reason. Over a third of women with breast cancer undergo a total mastectomy and a large number of them receive breast augmentation [1]. For breast reconstruction women usually receive silicone implants. Today implants consist entirely of silicone or they have a double lumen consisting of a saline construct on the inside and a silicone shell on the outside. The median life expectancy of silicone implants is approximately 10–16 years [2].
Capsular fibrosis is a local complication and the most frequent side effect after implant-based breast augmentation. The capsular tissue of this long-term foreign body response may stiffen and extend, becoming extremely painful and unaesthetic [3]. Radiotherapy, as part of adjuvant treatment for breast cancer, can also lead to an increased risk of tissue damage, infection, capsular reaction and poor aesthetic results due to the impairment of the blood supply to the skin [4, 5].
After breast prosthesis augmentation, a clinical and diagnostic follow-up should be performed to detect possible postoperative local complications. Diagnostic imaging after surgery is currently evaluated critically for various reasons and high diagnostic standards are required. Implant complications must be detected early, not only to avoid unnecessary and expensive implant changes, but, above all, to avoid consequential damage. Common complications associated with breast reconstruction can lead to early and late effects. Peri-implant fluid collection or hematoma and infection belong to early changes. Late complications including capsular contraction, foreign body reactions, intracapsular or extracapsular rupture, reactive lymphadenopathy due to leakage of silicone from direct injection or extracapsular rupture, fat necrosis and recently, anaplastic large cell lymphoma (ALCL) and breast fibromatosis [6–8].
Anamnesis and clinical examination with palpation by an experienced examiner are fundamental and indispensable in the assessment of breast implants. In addition an ultrasound examination of the implant should be performed as first imaging modality after clinical examinations. This is the most used imaging method as it is often available and a safe, noninvasive and repeatable technique [9].
Furthermore the results could be supplemented by specifically selected imaging methods such as MRI, CT and PET-CT. If necessary a histological/cytological sample can be taken [9, 10].
Materials and methods
Patients
In a retrospective clinical study between January 2015 and December 2019 40 women (age 29–84, mean age 53.7 years) were included who underwent breast surgery and augmentation with silicone implant due to breast cancer or for cosmetic reconstructive reason. Most patients (n = 27) underwent bilateral breast reconstruction because of breast cancer; two of them had bilateral cancer and 25 of them underwent unilateral mastectomy with immediate prosthetic reconstruction and contralateral breast symmetrization. Six women had gene mutation. Six women underwent unilateral mastectomy for cancer with delayed unilateral breast reconstruction. Two women with BRCA I mutation underwent a bilateral prophylactic mastectomy and prosthetic augmentation. Finally, five women obtained bilateral aesthetic breast reconstruction (Table 1).
Demographic and clinical data
Demographic and clinical data
All 40 women obtained a clinical examination and an ultrasound examination six to twelve months after surgery. An early and frequent change of breast implants are implant folds. This complication can already be palpated in the clinical examination, but even more precisely with ultrasound examination. Depending on the clinical findings, tissue density and suspicious lesions or suspicious for malignancy irregular tumor with micro-calcificaions an additional MRI, CT and/or PET-CT is/are performed.
The local ethics committee approved the retrospective design of this study and written consent form was available for all patients who were enrolled in the study (approval number 20-1755-104).
Fundamental ultrasound
A conventional ultrasound was performed on all patients in a supine position by the same high-resolution ultrasound device (LOGIQ E9, GE Healthcare, Milwaukee, USA). A linear multifrequency transducer (frequency range 6–15 MHz) was used for these examinations. An ultrasound examination of the entire breast on both sides was performed by one of three radiologists with more than two years of experience using ultrasound. B-Mode was optimized by speckle reduction imaging (SRI), tissue harmonic imaging (THI) and cross beam (ultrasound CT modality). For vascularization color coded Doppler ultrasound and Power Doppler was performed by optimized parameters for low flow imaging, with adapted flow parameters (PRF, color gain and wall filter).
After a B-Mode ultrasound examination was completed, the same radiologist performed an ultrasound elastography examination on the same screen. From the best image quality of strain elastography an integrated automatically core coded evaluation was used, with 5 points in green colors for the highest quality, yellow for sufficient quality and red for less quality. Tissue with highest degree of stiffness as homogenous blue was evaluated if possible with 5 green points of quality level. Soft tissue was coded by red or yellow false colors, intermediate tissue by green color.
There are two main elastography methods, i.e. shear wave and strain elastography. A shear wave elastography imaging method includes point shear wave speed measurement to quantify the tissue stiffness, which is a highly operator independent technique [11]. The basis of strain elastography imaging method is the compression of tissue, which causes tissue displacement or tissue strain.
For each equivocal lesion that was detected during ultrasound examination we carried out a supplementary contrast-enhanced ultrasound (CEUS). Hereby an additional vascularization of the breast masses can be assessed. For this purpose microbubbles are administered intravenously. The microbubbles cause a short-term increase of the ultrasonic signal making vessels and blood supply to the tissue visible. The advantage of CEUS is that it is also suitable for patients with contraindications such as renal failure or iodinated contrast allergy, which would make a contrast-enhanced MRI and CT impossible.
Magnetic resonance imaging
Excellent high-resolution and high-contrast images of breast tissue and the implant interface were acquired with a 1.5 Tesla MRI (Symphony Tim, Erlangen, Germany) by using of dedicated breast coils using phase-array technology. Examinations were performed with contrast agent (Dotarem, Guerbet, France). We use a common breast protocol combines axial silicone-selective sequences with axial fast spin-echo (FSE) T2-weighted imaging, enhancing or nonenhancing T1-weighted imaging with subtraction and diffusion weighted imaging.
High resolution computed tomography
During the study period two different multi-detector computed tomography scanners were used at our university hospital (Somatom Sensation 16 and Somatom Flash Dual Source; Siemens, Erlangen, Germany). Scans were performed with normal (120 mAs) or low-dose technique (40 mAs) and with or without the application of 70–120 ml of non-ionic contrast agent (e.g. Accupaque 350, Bayer-Schering AG, Berlin, Germany). For image analysis transverse, sagittal and coronal planes, with a slice thickness of 3.0–5.0 mm were reconstructed (kernel: B60f and B40f).
Positron emission tomography –computed tomography
PET-CT scans were performed unenhanced with low-dose technique (35 mAs, on Somatom Sensation 16; Siemens, Erlangen, Germany). Transverse, sagittal and coronal planes of the images were reconstructed, with a slice thickness of 5.0 mm and B30f or B31f kernel.
All images were achieved in a Picture Archiving and Communication System (PACS) and are available for retrospective analysis.
If necessary a histological/cytological sample was taken proven by an ultrasound-guided core needle biopsy.
The breast implants were assessed by three radiologists, specialized in breast imaging in consensus. The grade of capsular contracture was classified according to the Baker score: Grade I –the breast is soft and appears natural in size and shape; Grad II –the breast is a little firm, but appears normal; Grad III –the breast is firm and appears abnormal; Grad IV –the breast is hard, painful to the touch, and appears abnormal.
Clinical outcome
All patients were obtained after surgery with a follow-up care (for at least 10 years) at a breast care center.
Results
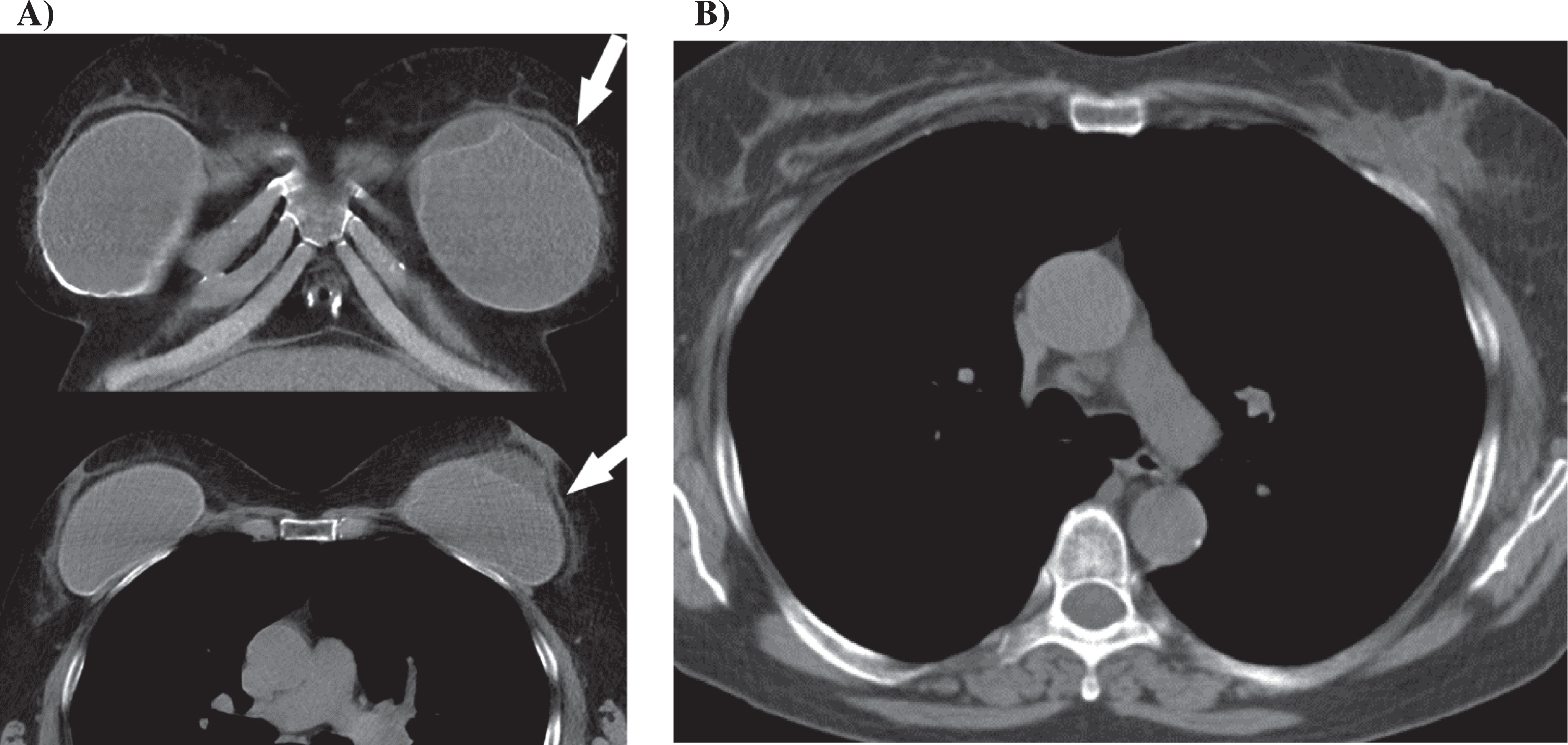
Implant folding’s - proven with US and an additional MRI and CT (Figs. 1 & 2) –developed in 16 out of 40 women.
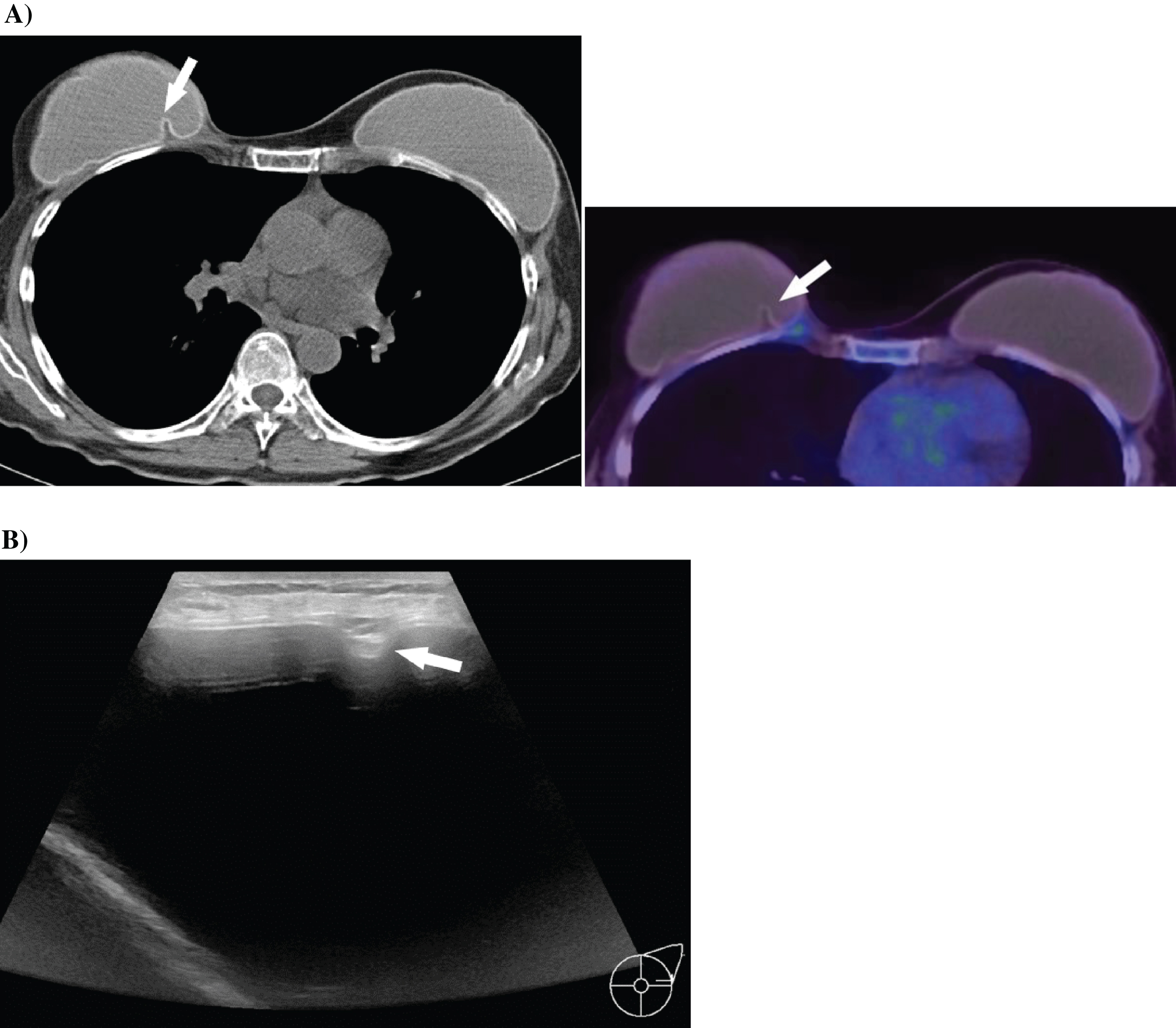
A & B 51-year-old woman with a family predisposition of breast cancer and a history of prophylactic mastectomy on both sides and breast reconstruction with silicone implants. A) CT (right) and PET CT (left) examinations with implant folding on the right side (white arrow) without any sign of rupture. B) Corresponding to the CT examination, the ultrasound examination shows the implant folding (white arrow) without any rupture signs.
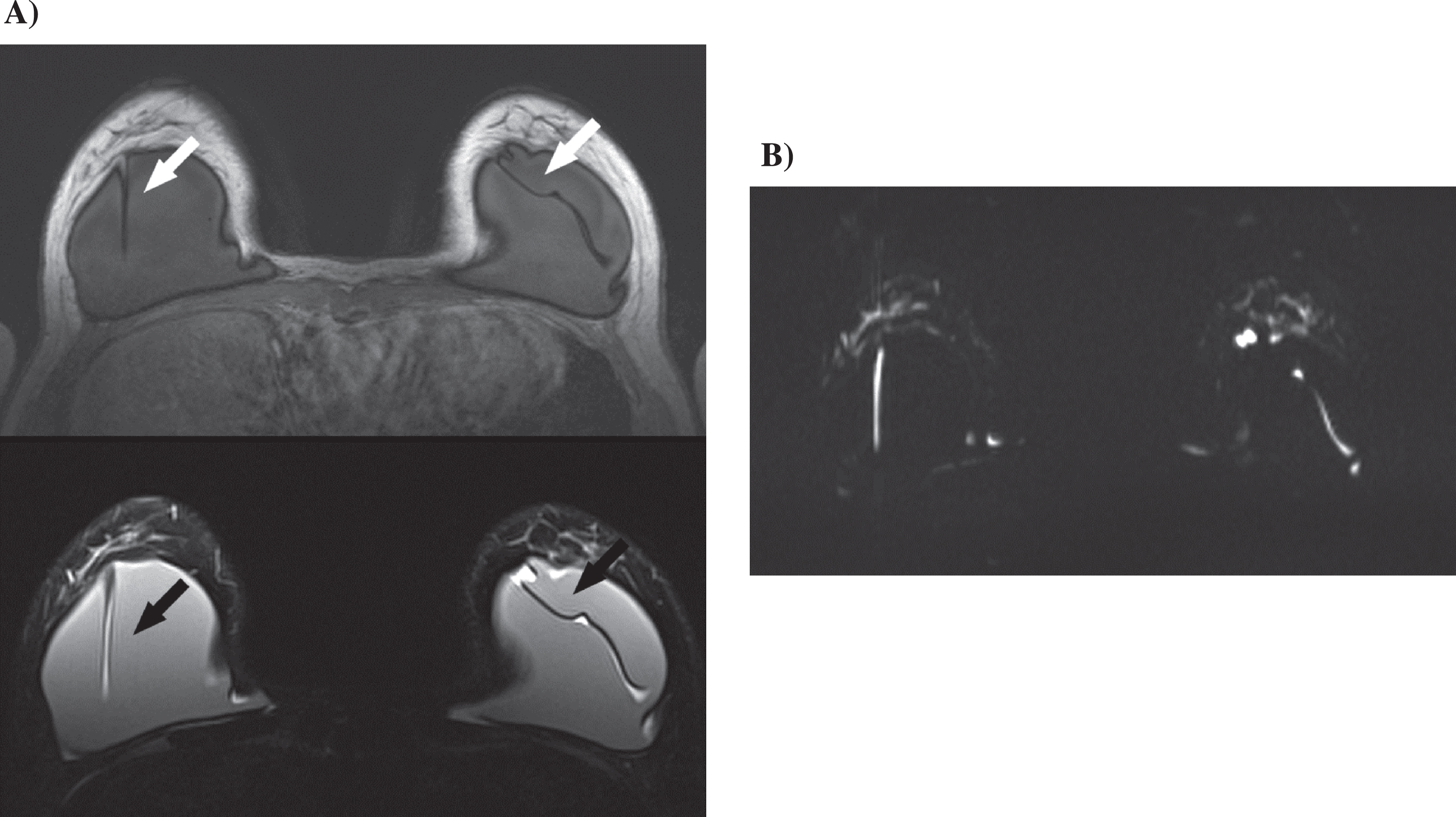
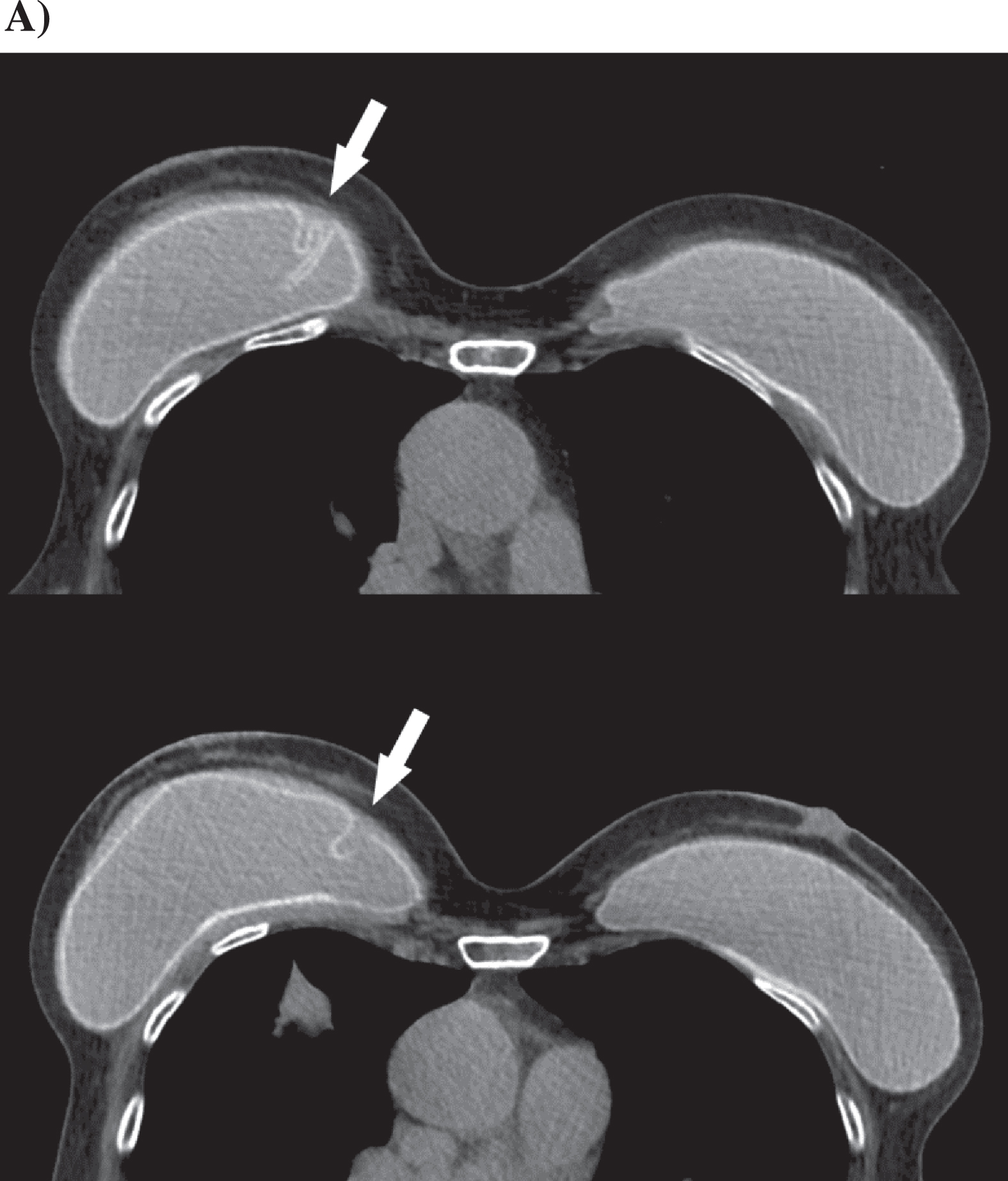
A & B 55-year-old woman with a history of breast cancer, bilateral mastectomy and reconstruction using silicone implants. A) The MRI shows a bilateral implant folding (white arrow) in T1 sequence (upper) and T2 sequence (lower). No signs of rupture. B) Corresponding diffusion-weighted sequence.
25 women had a capsular contracture grade I, eleven women had a capsular contracture grade II (Fig. 3), one woman had capsular contracture grade III and one woman had capsular contracture grade IV (Fig. 4) due to the distribution of the Baker score (Table 2). This findings were verified with MRI (n = 10), CT (n = 9) and PET-CT (n = 1). One woman had intracapsular rupture (Figs. 5 & 6) and one woman had extracapsular rupture. Both ruptures were detected on CT and surgically proven.
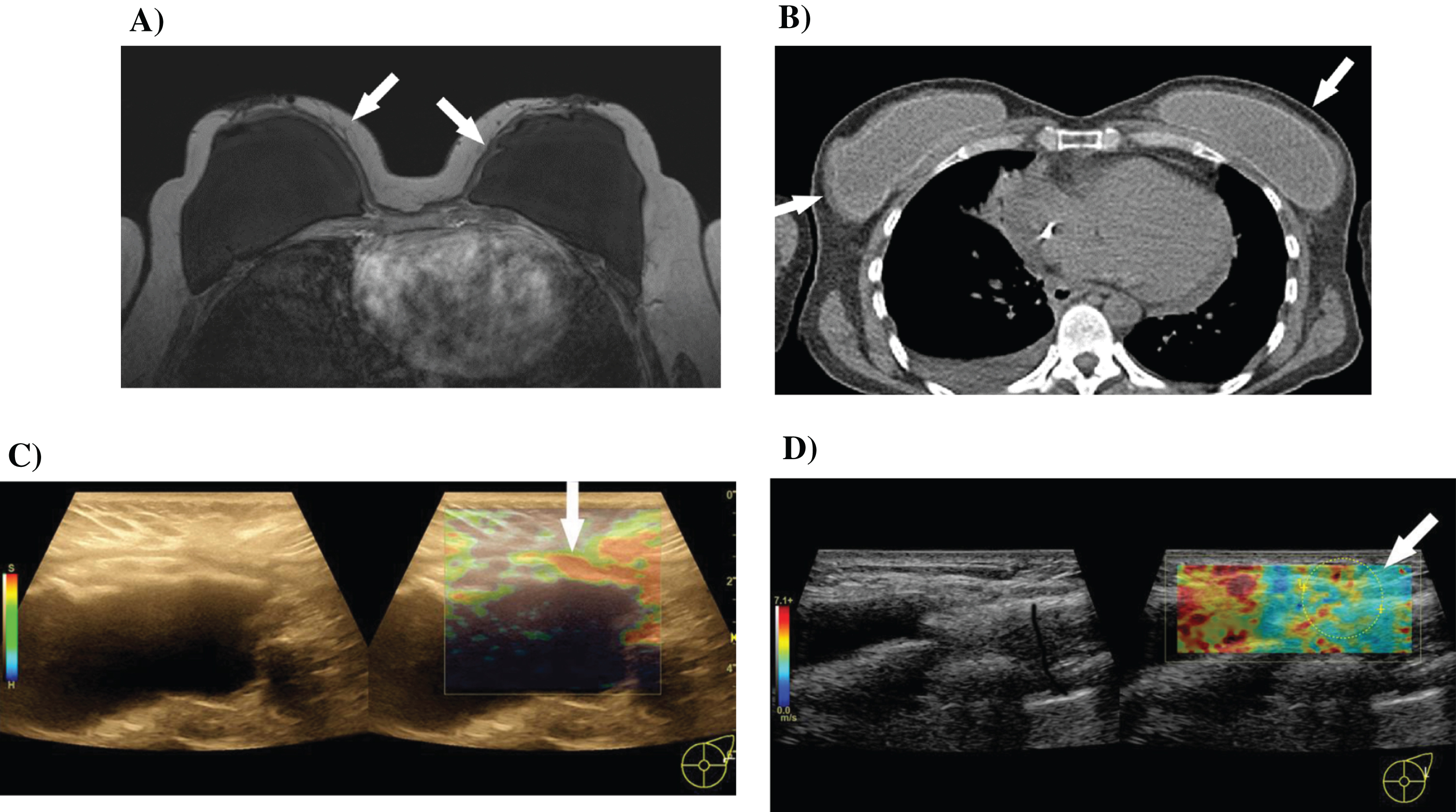
A–D 33-year-old woman with a known gene mutation (BRCA-1) and a history of prophylactic bilateral mastectomy for breast cancer and reconstruction using silicone implants. A) MRIimage (T1 sequence) shows moderate capsular periprosthetic fibrosis on both sides (white arrows). No capsule rupture. B) Corresponding PET-CT. C) Ultrasound examination with B-image on the left side and ultrasound elastography on the right side. In false colors, strain elastography shows different densities of the periprosthetic tissue from blue (hard) to red (soft) (white arrow). D) Using shear wave elastography, assessment of the elasticity of the periprosthetic tissue in false colors, this time red for hard and blue for soft. The white arrow shows the region of measurement of the induration.
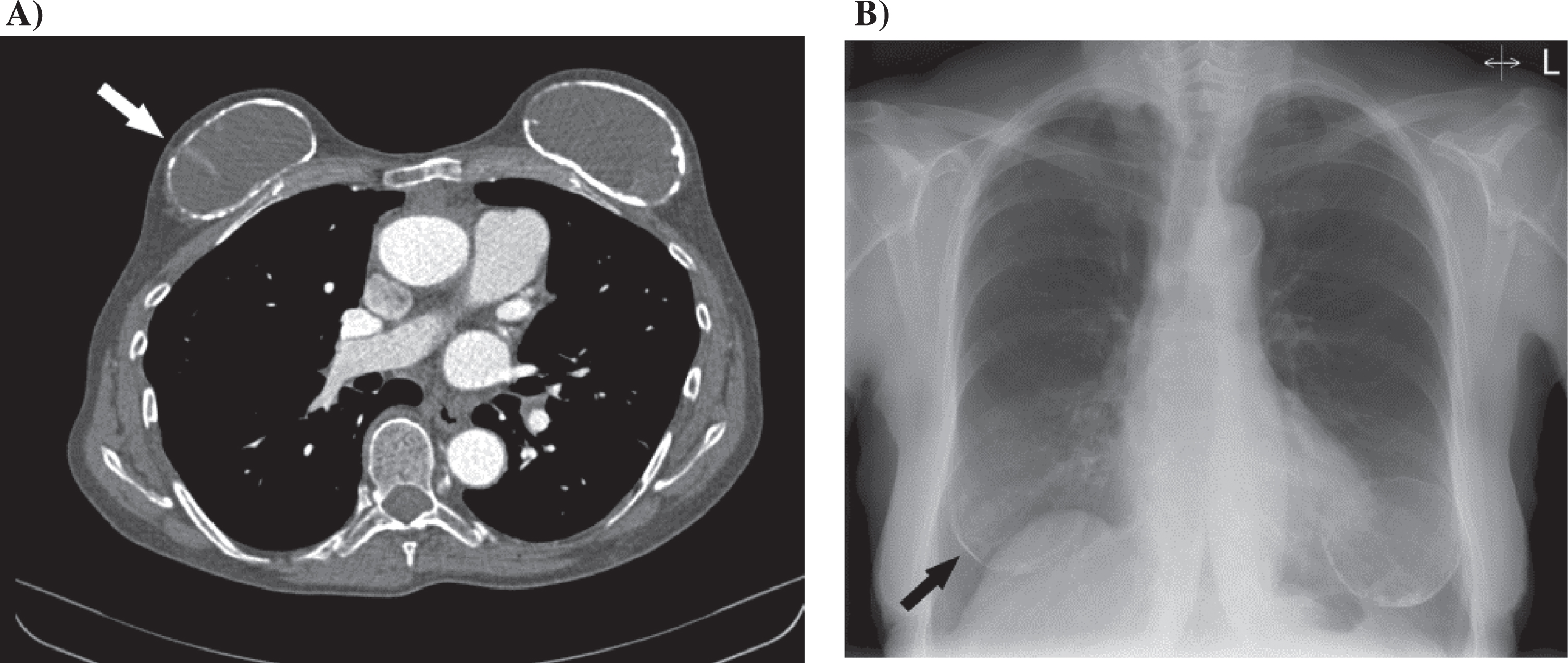
A & B 59-year-old woman with a history of mastectomy for breast cancer on both sides and breast reconstruction with silicone implants. A) CT examination shows capsular contracture Baker grade IV on both sides with calcification and on the right side with folding (white arrow). B) Corresponding X-ray examination with visible capsular calcification (black arrow).
Long-term complications after implantation of breast prostheses
A & B 60-year-old woman with a history of prophylactic mastectomy on both sides due to a known gene mutation and following breast reconstruction with silicone implants. A) CT examination shows a intracapsular rupture of the silicone implant on the left side (white arrow) in coronal (upper) and axial (lower) reconstructions. B) CT examination after implant explantation.
A 69-year-old woman with a history of breast reconstruction using silicone implants on both sides for breast cancer. A) Intracapsular rupture of the silicone implant on the right side (white arrow). Interruption of the inner capsule and irregular wavy structural change of the inner capsule.
No patient had a silicone accumulation in the lymph nodes. One patient had pathologically enlarged axillary lymph nodes, the PET-CT showed inflammatory changes.
Long-term complications such as the development of malignant breast tumors or anaplastic large cell lymphoma (ALCL) could not be observed during our investigation period.
Diagnostic imaging plays an important role in the follow up of breast implants and the detection of possible early or long-time complications [12, 13]. It should be taken into account that a rupture of breast implant can lead to locally reactive changes, which can ultimately lead to a spreading systematic defense reaction. This carries the risk for the development of a secondary tumor. To the important tasks of imaging in regard to implant diagnostics, count: Assessment of implant shape and position, surrounding tissue and axilla; the early detection of capsular fibrosis with assessment of the expression (Graduation); the assessment of silicone leakage (silicone abrasion, silicone bleeding); the characterization of lymph node changes (detection of silicone); the possible detection of malignant tumors; the detection of inflammation and of changes in malignant tumors like lymphoma.
Radiological features of intracapsular rupture are: Inhomogeneous internal structures, circumscribed contour irregularity and small silicone leakage. Diagnostic criteria of extracapsular rupture are: Leakage of a large part of silicone, migration of silicone in lymph nodes, contour interruption and capsular folding until rupture [14].
Early complications such as foldings can be detected with a palpation by an experienced examiner and additionally by high-resolution ultrasound diagnostics [1, 9]. High-resolution linear matrix transducers with transmission frequencies from at least 6–15 MHz are useful as a higher frequency records the level of details close to the surface; while lower frequencies guarantee a sufficient depth of penetration. MRI can be helpful in early detection of capsular fibrosis and their graduation as well as silicone leakage [15].
Availability and technical requirements, particularly a detailed, artifact-free resolution, plays a crucial role for the MRI. The advantage of MRI is the imaging of the implant including its completely surrounding tissue and the axilla. In addition to the standard sequences, the diffusion-weighted sequences and the special silicone-sensitive sequences are used. Other studies suggested that late peri-implant fluid collection and/or masses could be identified at silicone implant protocol of breast MRI 24 months or later after reconstructive surgery [10]. An additional contrast medium application can help to detect tumors early. However, gadolinium application can be associated with side effects, whereby contraindications such as limited kidney function also must be considered. Earlier and irregular contrast enhancement followed by an early washout is characteristic of a malignant process. The benefits of diffusion-weighted sequences should not be underestimated: a signal rise at higher b values and a signal reduction in the ADC image can be a sign of a malignant process.
The use of the dual source multi slice CT is still experimental. It can be helpful to detect an external implant rupture, a silicone leakage and a silicone deposits in lymph nodes. However, radiation exposure remains critical.
Regarding lymph node diagnosis the imaging requirements are to find early symptoms like reactive inflammatory changes, possible silicon deposits and the development of tumor lymph node.
The regular palpation by an experienced physician is indispensable. The high-resolution ultrasound can be helpful to detect changes between the cortex and the hilus of lymph nodes. Characteristics of reactive changes in lymph nodes are a wide cortex and the presence of the fat hilus. Tumor lymph nodes are round and with reduced or lack of fat hilus. Another possibility to examine changes of lymph nodes is the examination of the microvascularization with high-resolution transducer of the color-codes Duplex Sonography (FKDS) or the Power Doppler (PD) and particularly the use of CEUS. Ultrasound elastography can also be helpful to detect reactive or tumor lymph nodes. Both are characterized by irregular induration.
If the lymph node diagnostics are performed with contrast enhanced CT or MRI it is important to note the size and the extent of contrast enhancement. Often a differentiation of reactive and malignant lymph nodes is only possible in PET-CT. Finally, the diagnosis can be confirmed histopathologically.
In our study, we were able to expand the ultrasound diagnosis of capsular fibrosis and the techniques of ultrasound elastography. Induration of the tissue can be presented with compound technique in pseudo color scales and are therefore more accessible for a correlation with clinical findings. The results can be better documented for follow-up. The shear wave technology reliably analyzes the fibrosis grade in liver tissue [16]. The current literature suggests that ultrasound strain elastography represent a valuable measurement tool to evaluate different properties of idle breast implant. This could be an additional help for clinical investigation and could be correlated with Baker's classification [17]. Ultrasound elastography represents also a useful tool to evaluate the compressibility of the peri-implant capsule, the implant and the surrounding tissue and can be used as a complementary method to MRI, especially in patients where radiographic- or MRI-contrast medium injection is contraindicated [18, 19].
Our research has shown that this technology can also analyze periprosthetic tissue indurations with reproducible measured values. Further multi-center analyzes need to be conducted to determine the exactly critical measured values.
CEUS represents a new ultrasound imaging with the use of special microbubbles and without the risk of generating a renal dysfunction [20]. Therefore, the numbers of clinical studies are increasing using CEUS for tumor detection and characterization, for detection of sentinel lymph nodes, for assessment reactive inflammatory changes and in our own investigations also in terms of detection of endoleakages [21-25]. Consequently, new modern imaging technology of implant diagnostic including modern digital mammography, high-performance ultrasound diagnostics, MRI, CT and PET-CT and needs a critical analysis by clinically experienced physicians and a multi-center analysis for establishing diagnostic certainty and practicality [26].
Conclusion
To prevent early complications after breast implant surgery a regular palpation and a clinical examination especially by an experienced physician are indispensable. Diagnostic imaging methods complement each other and in case they are multimodal, it is easier to identify complications. Modern diagnostic modalities like ultrasound and magnetic resonance imaging expand the spectrum and improve diagnostic safety.
Conflict of interest
The authors have no conflict of interest to report.