
Abstract
Keywords
Introduction
Placement of a breast implant often causes a foreign body response that results in formation of a collagenous capsule. This leads to the common complication of capsular contracture after breast reconstruction, which is accompanied by pain, discomfort, and distortion of the implant and breast. Despite advances in implant material and surgical techniques, capsular contracture still afflicts about 10% of patients who receive a breast implant [1–3]. The presence and severity of capsular contracture can be evaluated clinically using the Baker score, which was devised in 1979. This approach is commonly used and is based on the appearance, texture, and tenderness of the breast [4]. The Baker score is useful for diagnosis, but is a subjective classification that is based on clinical findings, rather than an objective evaluation of the severity of capsular contracture.
Computed tomography (CT), magnetic resonance imaging (MRI), and ultrasound (US) can be used to measure the thickness of the capsule [2, 5]. These methods are useful for diagnosis of capsular contracture since the capsule thickens and hardens with progression of the condition. The thickness and stiffness of the capsule are both related to the degree of capsular contracture, as shown by the thin but stiff capsule described by Prantl et al. [6]. Ultrasound elastography (UE) is a noninvasive imaging technique that can measure tissue stiffness in response to a given force. Elastography measures the mean stiffness of lesions bidimensionally, and thus can quantify the stiffness and thickness of the capsule [7, 8]. Prantl et al. evaluated capsular contracture using an objective stiffness measurement with strain elastography (STE), applied by repeated manual compression of the transducer. Lesion deformation relative to surrounding normal tissue was measured and displayed in color. However, data acquisition and interpretation of elasticity images are largely dependent on the operator and there may be significant interobserver variability [9].
Shear-wave elastography (SWE) uses an acoustic radiation force impulse that allows measurement of the propagation speed of shear waves within tissue to quantify local stiffness. Quantitation by SWE depends less on the individual operator and is highly reproducible [10, 11]. Thus, recent studies suggest that SWE improves the diagnostic accuracy and specificity compared to conventional US in diagnosis of breast lesions [12, 13]. The present study was performed to compare the reliability of STE and SWE for reproducible measurement of capsular contracture after breast implant reconstruction, and to investigate the correlation of data obtained with the two techniques with the Baker score.
Materials and methods
The subjects were 20 patients (27 implants) who underwent breast reconstruction in a two-stage procedure using a subcutaneous tissue expander and standard silicone implants. The age at entry ranged from 24 to 68 years old (mean, 50.45). The exclusion criteria were cases with a non-detectable implant capsule and a history of breast surgery or radiation therapy. All reconstructions were performed by the same senior plastic surgeon. Deformation, texture on palpation, tenderness, and overall Baker score were evaluated by two trained plastic surgeons. In the Baker score, the severity of capsular contracture ranges from grade I, in which the breast is normally soft and looks natural, to grade IV, in which the breast is hard, painful, and deformed.
STE and SWE were performed using a GE Healthcare LOGIQ E9 ultrasound scanner with real-time SWE and a 9L linear (4–9 MHz) probe (GE Healthcare, Amersham Place, Little Chalfont, Buckinghamshire, UK). After the elasticity imaging mode was selected, the patient in the supine position held her breath for 3–5 s for imaging. When the target area was located at the fibrosis capsule just above an outer envelope of the breast implant, the operator launched the STE or SWE sequence (Fig. 1A). For STE, the strain ratio, which compares two separate areas in the same elastogram, was used (Fig. 1B). The average strain in the normal reference area was calculated and then divided by the average strain in the area of interest by the STE software. For SWE, the circular quantitative sampling frame was initiated to measure the elastic modulus of the capsule in a region of interest (ROI) with a diameter of 1–3 mm (Fig. 1C). The system then automatically calculated the elastic modulus mean (in kPa) within the ROI.
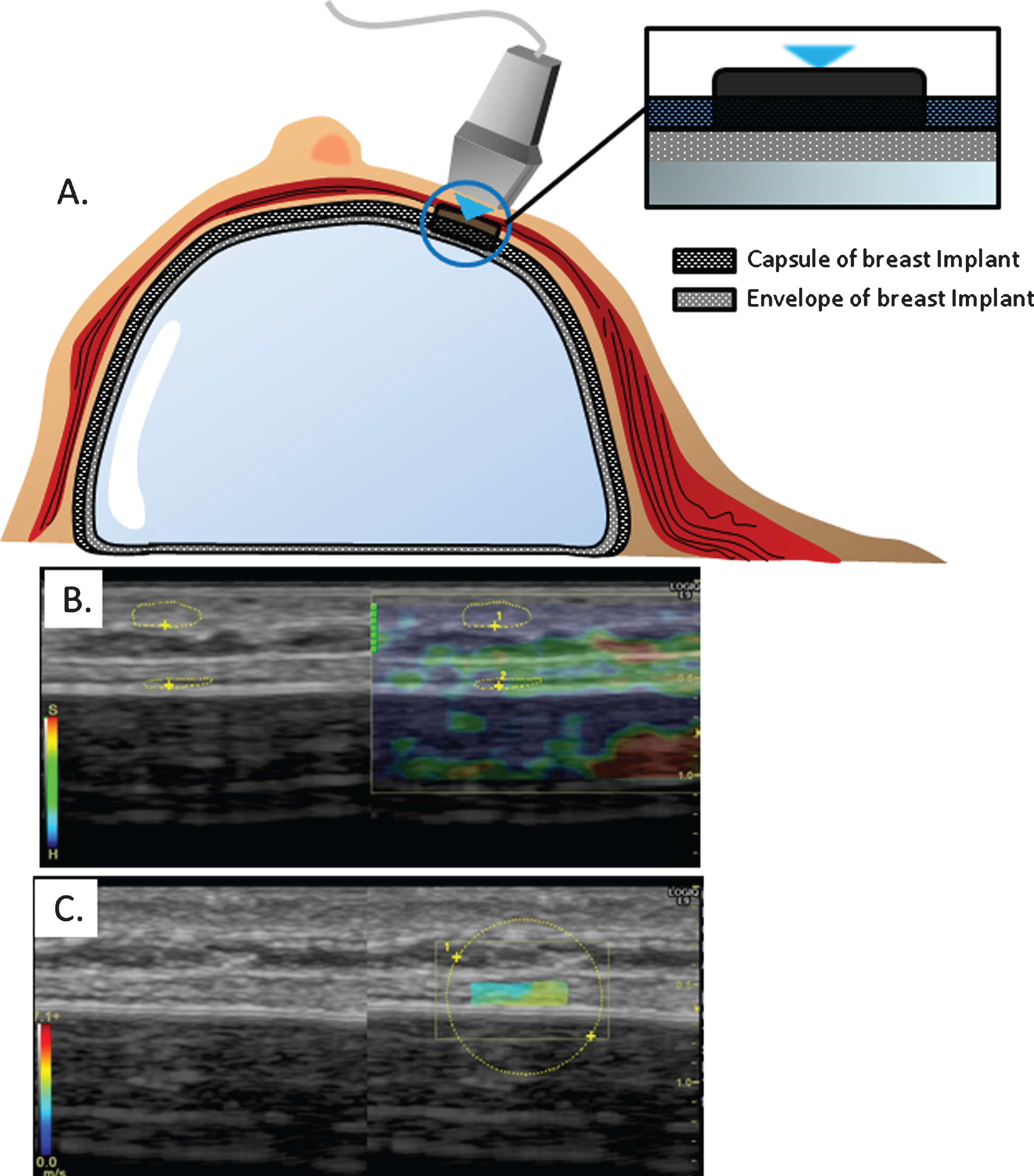
A. Schematic illustration of the measurement of breast capsular stiffness using ultrasound elastography. Typical example of a color-coded presentation of a breast capsule (shear wave speed) superimposed on a B-mode ultrasound image. B. Strain elastography, C. Shear wave elastography.
Data obtained by the same device operator were recorded on the same day three times for the same subject. An intra-class correlation coefficient (ICC) for reproducibility assessment was calculated to evaluate agreement between STE and SWE. Correlations between the two methods and between the Baker score and each method were evaluated by Spearman rank correlation analysis. Instat 1 3.0 software (GraphPad, La Jolla, CA) was used for statistical analysis. ICCs reflect the consistency of measurements: ICC < 0.20 indicates poor consistency, 0.20–0.40 indicates general consistency, 0.40–0.75 indicates good consistency, and ≥0.75 indicates very good consistency. A P value < 0.05 was considered significant.
ICCs were 0.724 (95% CI: 0.552 to 0.851) for STE and 0.878 (95% CI: 0.785 to 0.937) for SWE. The correlation of the mean stiffness in the ROI, including the capsular wall of the breast implant, measured with the two methods was low (r = 0.6788, P < 0.001) (Fig. 2). Significant differences in reproducibility were found between the two methods.
The Baker score classifies the clinical evaluation of deformation, texture, and tenderness of the breast into 4 levels of severity. Of the 27 breasts, 6, 12, 5 and 4 were classified as Baker grades I, II, III, and IV, respectively. Pearson rank correlation analysis showed a significant relationship between the Baker score and capsular stiffness evaluated by STE (0.6983, P < 0.001) and SWE (0.8124, P < 0.001) (Fig. 3). The correlation between the Baker score and SWE results was stronger than that for STE data.

Correlation between STE and SWE results for breast capsular stiffness.
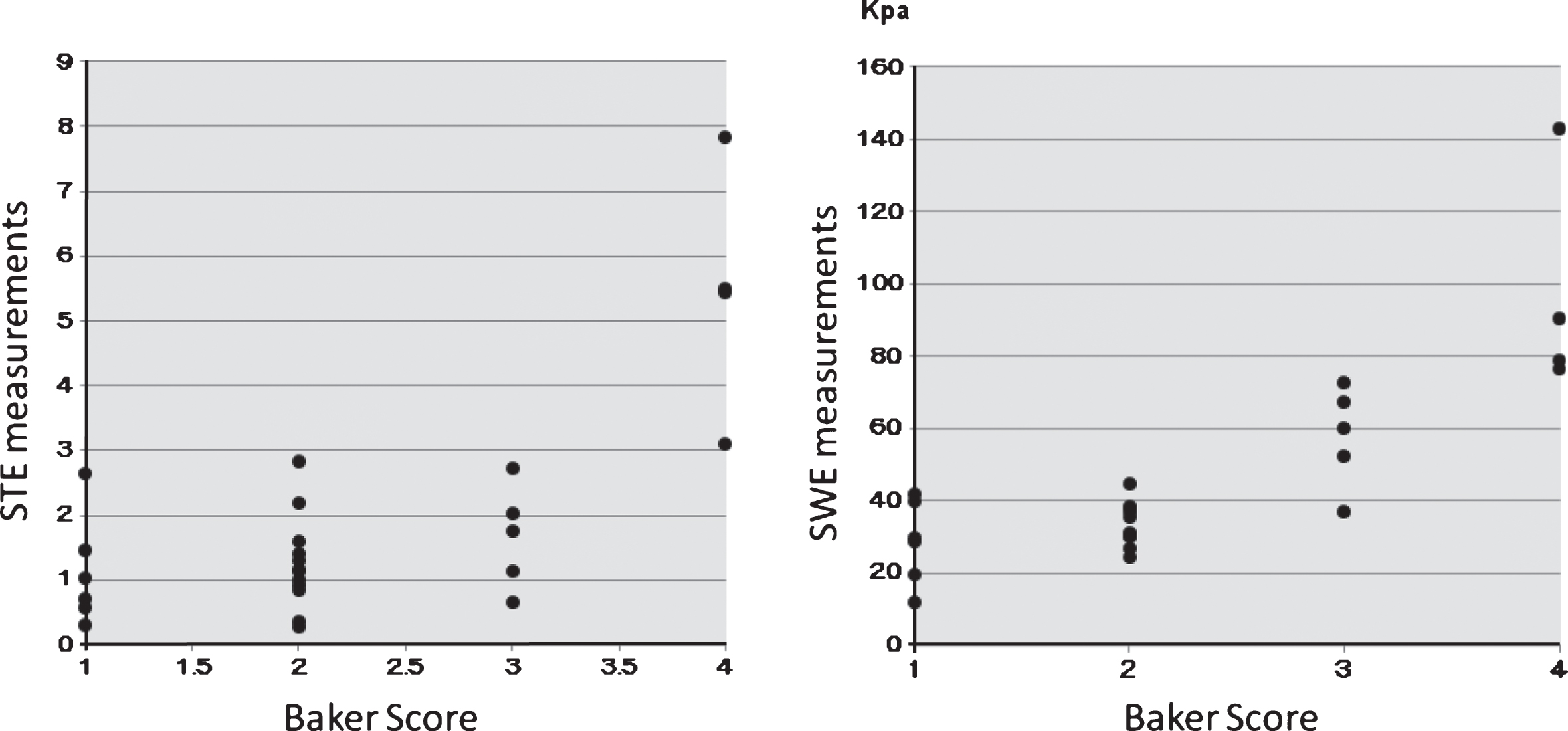
Correlations of Baker score with STE (left panel) and SWE (right panel) results for breast capsular stiffness.
Based on definition of Baker level III or higher as capsular contracture, histograms of SWE values of breast capsular stiffness showed a cut-off of approximately 52 kPa in distinguishing patients with and without capsular contracture (Fig. 4). Additional SWE data and Baker scores in a long-term study may allow more accurate definition of this cutoff point in a new classification of capsular contracture.
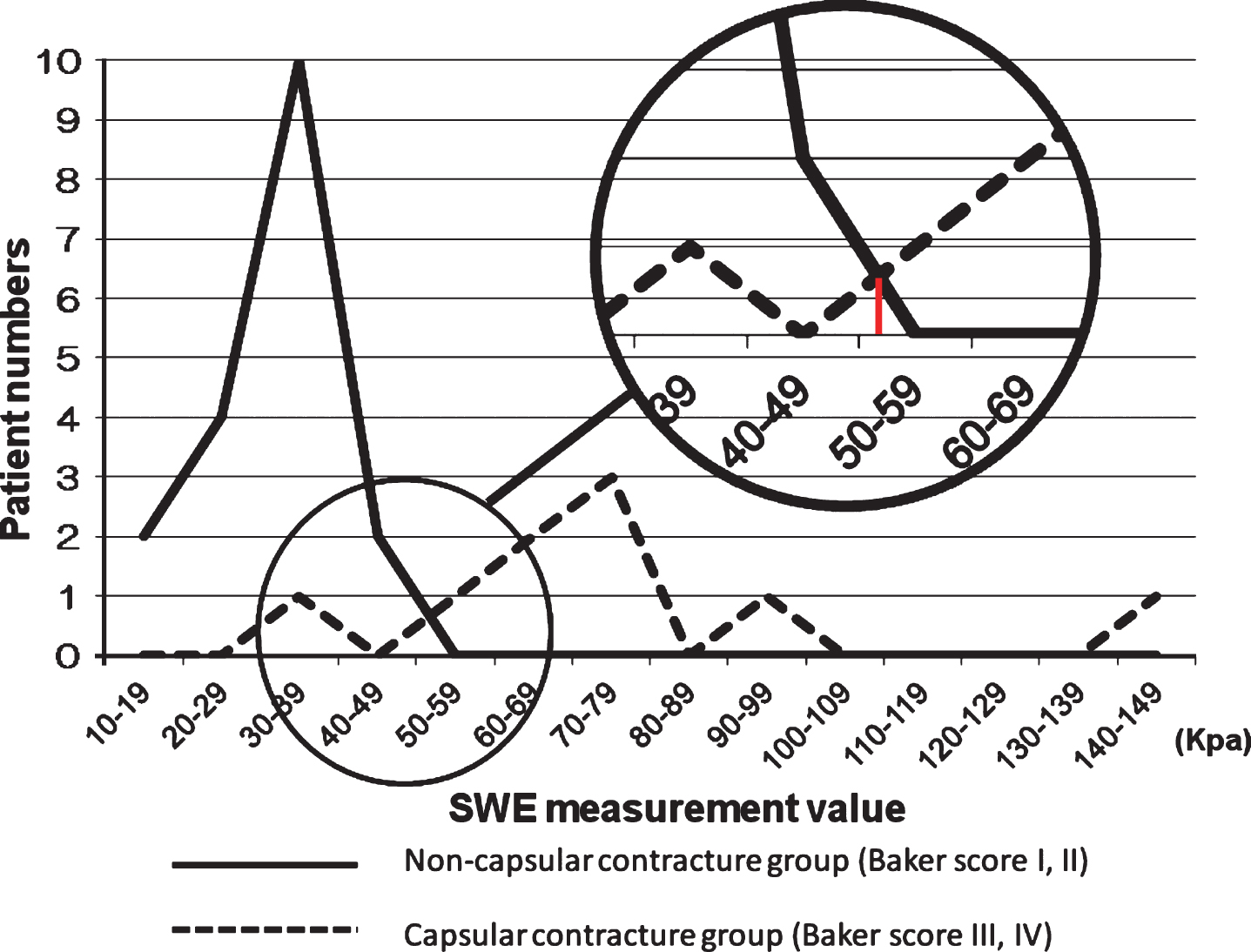
Histograms of SWE results for breast capsular stiffness in patients without (Baker score I, II) and with (Baker score III, IX) capsular contracture, suggesting a cut-off point of approximately 52 kPa for diagnosis of capsular contracture.
Breast reconstruction has become a standard treatment worldwide due to development of safer and simpler procedures. Of the various treatment modalities, use of breast implants is the most widely practiced, but capsular contracture around the implant continues to be a common complication [1–3]. Among several diagnostic scales for capsular contracture, the Baker score based on palpation and visible findings is widely used [4]. The Baker score is dependent on the stiffness of the breast, but evaluation of stiffness by palpation is largely dependent on the examiner and lacks consistency in follow-up of an individual patient and in comparison among patients.
Ultrasound technology is increasingly used for diagnosis of tumors or evaluation of tissue properties. Ultrasound elastography (UE) is a cutting-edge technology that can directly measure the mechanical properties of tissues, including stiffness. Thus, we hypothesized that UE might be able to evaluate capsular contracture around breast implant [7, 8]. Several types of UE techniques are available, of which STE and SWE are most common [14, 15]. In this study, we found that STE is a semi-quantitative method that is less reliable than SWE because of use of the strain ratio, which compares the normative reference area and an area of interest in the same elastogram. The reliability of measurements with STE is also affected by operator technique since the ultrasound probe is manually operated.
Reproducibility is important for widespread adoption of any imaging technique. The current study showed that the reproducibility of SWE (ICC: 0.878) was higher than that of STE (ICC: 0.724), and the correlation coefficient for breast implant capsule stiffness measured with the two methods was low (r = 0.6788). These results support our hypothesis that SWE is the more reliable modality to measure tissue stiffness. Reproducibility is essential for monitoring changes of the capsular wall surrounding a breast implant in daily clinical practice, and thus our results also show that SWE is a better approach for follow-up of capsular contracture. SWE also measures the mean stiffness in a 2D ROI, which reflects both the thickness and stiffness of the capsule.
The severity of capsular contracture after breast implant reconstruction should be evaluated using the pain level, in addition to the stiffness and thickness of capsular tissue. Rzymski et al. showed that breast pain correlates strongly with stiffness in elastography at 4 to 10 days after breast augmentation [13]. In the current study, we found a strong correlation between SWE measurements and the Baker Score, which suggests a strong relationship between subjective clinical evaluation of capsular contracture, including breast pain, and SWE measurements of capsular stiffness and thickness. These results are partly consistent with previous reports showing that increased capsular thickness on MRI and US is correlated with a higher Baker score [2, 15]. Thus, the strong relationship of SWE results with the subjective evaluation also indicates that SWE may be useful for objective postoperative follow-up of a capsule wall surrounding a breast implant.
To the best of our knowledge, this is the first study to compare the reliability of STE and SWE for evaluating the capsule around a breast implant, and to investigate the relationship between UE measurements and Baker score. We note several limitations of the study, including that the results are based on a modest sample size, only SWE and STE were compared among many elastography techniques, and interobserver variability was not assessed. Within these limitations, the results suggest that SWE provides quantitative estimates of tissue stiffness that correlate well with clinical symptoms. A further study is required before this modality can be applied clinically as a standard assessment tool, but our findings suggest that SWE will be useful for evaluation of capsule contracture around breast implants.
Competing interest
The authors have declared that no competing interests exist.
Footnotes
Acknowledgements
The study was approved by the ethics committee of our hospital (Kyoto Prefectural University of Medicine).