
Abstract
BACKGROUND:
Analyzing responsiveness to P2Y12 therapy is vital to preventing thrombotic and hemorrhagic complications in patients with cardiovascular diseases.
OBJECTIVE:
This study evaluates a new Anysis-P2Y12 assay system against VerifyNow-P2Y12 in cardiac patients and analyzes the P2Y12 low-response rates of the two devices with various cutoff values.
METHODS:
In total, 125 citrated blood samples were collected from cardiac patients referred for a P2Y12 antiplatelet response test. In the Anysis assay, the test result was the migration distance (MD) until the blood flow stops, which is comparable to both P2Y12 reaction units and percent inhibition obtained using VerifyNow.
RESULTS:
The MDs without and with P2Y12 were 182±30 and 264±12 mm, respectively (p < 0.0001). Compared to VerifyNow-P2Y12, the sensitivity and specificity of Anysis-200 were 96.8% and 88.7%, respectively. Cohen’s kappa coefficient between the two devices was 0.761, indicating a high agreement. However, there was an apparent difference in the low-response rate to P2Y12, which was 36.5% for VerifyNow and 5.9% for Anysis.
CONCLUSIONS:
The performance of the newly developed platelet function assay, Anysis-P2Y12 was equivalent to that of VerifyNow-P2Y12 in terms of sensitivity and specificity. The Anysis-P2Y12 assay may help screen patients with abnormal P2Y12 non-responsiveness.
Introduction
Several methods and devices are now available to assay platelet function associated with antiplatelet therapy. The VerifyNow assay (Accumetrics, San Diego, USA) is one of the most widely used of these tests, but the clinical feedback on this test was found to be somewhat negative and unreliable. Dual antiplatelet therapy (DAT) has been employed for platelet thrombus prophylaxis prior to deployment. DAT consists of the cyclooxygenase (COX) antagonist aspirin and P2Y12 adenosine diphosphate (ADP) receptor antagonist clopidogrel. However, even with DAPT employment, 10%–38% of the patients did not adequately respond to the antiplatelets [1, 2]. The low response rates also varied widely depending on the study methods, devices used, and adopted cutoff values [3, 4]. Furthermore, many endovascular surgeons struggle with assay results that are inconsistent with clinical outcomes [5, 6]. Thus, innovative changes in the current research paradigm of thrombosis are highly required.
As an alternative, the Anysis-200 analyzer (Rheomeditech, Seoul, Korea) has been recently introdu-ced in cardiovascular surgery to manage bleeding risk [7] and antiplatelet therapy [8]. The bleeding risk assay can be used to detect either epinephrine- or ADP-induced platelet activation, whereas the antiplatelet therapeutic assay can be used to detect either platelet inhibition through the COX–arachidonic acid (AA) pathway or P2Y12 receptor inhibition. Anysis-200 is a new platelet assay system with innovative mechanisms of upstream activation and downstream aggregation [9–12] and provides the migration distance (MD) of the blood flow through the micro-channel to analyze platelet function. The MD is comparable with either the P2Y12 reaction units (PRUs) or percent inhibition (%INH) obtained using VerifyNow. Thus, this study aims to evaluate the feasibility of the Anysis-P2Y12 assay for antiplatelet therapeutic response and to analyze the difference in low response rates of P2Y12 between devices.
Materials and methods
Patient samples
In total, 125 citrated blood samples were collected at the Korea University Guro Hospital between April 2020 and December 2020. Similar to our previous studies [7, 8], we adopted several exclusion criteria for this study as follows: platelet count < 100×109/L, hematocrit (Hct) < 35% and > 60%, abnormal prothrombin time or activated partial thromboplastin time values a month prior to the study, pregnancy, and use of anticoagulation agents. The samples were divided into two groups: P2Y12-treated experimental (n = 63) and non-treated control (n = 62) groups.
The study was approved by the Institutional Review Board of Korea University Guro Hospital (IRB No. 2019GR0390). The blood samples were collected in sodium citrate tubes (BD Vacutainer Systems, Franklin Lakes, NJ, USA) by venipuncture using 21-G needles. After blood collection, the tubes were gently inverted (five to six times). During transportation, special care (room temperature, shear rate < 400 s–1) was taken to avoid undesired platelet activation. Prior to testing, blood samples were allowed to stand still at room temperature (24°C) for 30 minutes without any movement. All the tests were completed within 2 h after blood collection to minimize the risk of time dependent platelet malfunction.
Anysis-200 platelet function analyzer
Anysis-200 is a new antiplatelet assay system with a disposable microfluidic chip (Fig. 1). The microfluidic system is designed for platelet thrombosis assays using upstream activation and downstream aggregation of platelets. The chip consists of a sample chamber, a tube packed with fib-rinogen-coated microbeads, a straight running tube, and a vacuum generation system. The sample chamber is coated and lyophilized with reagents such as ADP (2μM) as an agonist and prostaglandin E1 (PGE1, 0.6 nM) as an antagonist. The sample chamber was filled with citrated blood, and the P2Y12 receptor of platelet might be activated with the reagents. With applying a vacuum pressure, the blood sample with activated platelets was then aspirated into the fibrinogen-coated-beads section and then kept flowing until the end of the running tube. If any occlusion occurred in the bead-packed section, the blood flow stopped, and the blood migration distance (MD) was determined using an image processor. The MD, as an indicator of platelet adhesion and aggregation was comparable to the PRU obtained in the VerifyNow assay. According to the manufacturer’s instructions, the cut-off value of MD is 225. Any values > 225 mm are considered abnormal or indicative of P2Y12-inhibited platelet function.
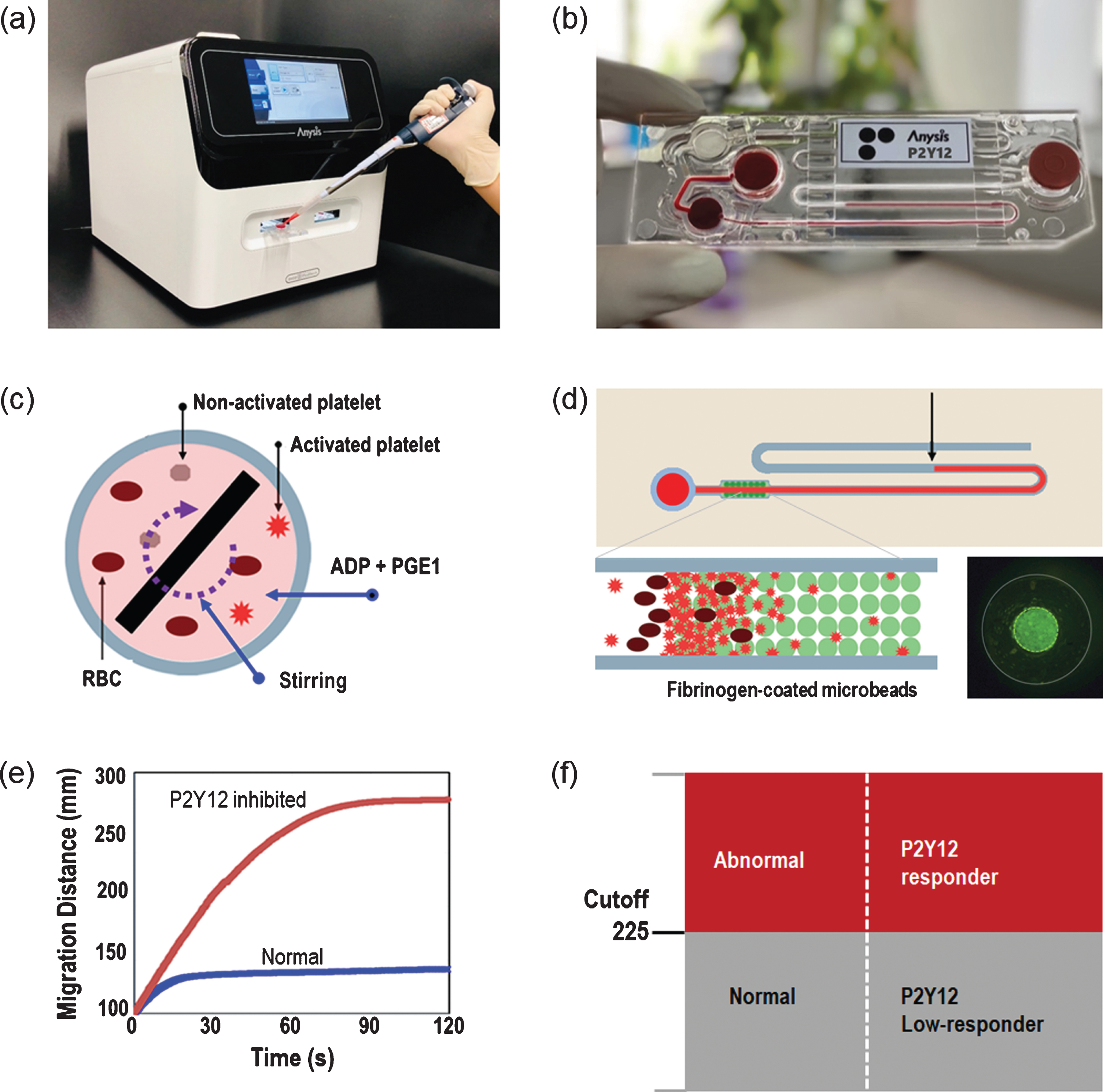
Anysis-200 platelet function analyzer. (a) Anysis-200 instrument. (b) Anysis-P2Y12 microfluidic chip consisting of a sample loading chamber, sample chamber with a stirrer containing ADP and PGE1, microbead-packed tube, and running tube. (c) The stirrer mixes ADP and PGE1 with blood in the sample chamber. (d) Densely packed fibrinogen coated microbeads in a test section. (e) Migration distance (MD) of blood samples with respect to time for normal and P2Y12-inhibited blood samples. (f) Determination of Anysis-P2Y12 using MD as the cutoff.
The fibrinogen-coated microbeads were packed into a rigid tube (inner diameter = 0.45 mm, length = 2 mm), which was inserted into a flexible tube (di = 0.8 mm). The diameter of the microbeads was carefully determined to be 50±5μm to allow all blood cells to freely pass through the pores formed in the microbead-packed tube. However, adhesion and aggregation of platelets to the beads reduces the effective pore diameter, eventually clogging all pores. It used to take couple of minutes to get clogged with minimal blood volume (< 250μL). Anysis-P2Y12 assay adopts upstream activation and downstream aggregation of platelets in a microfluidic flow system that mimics the in vivo hemodynamic environment of the vasculature [8–11]. In fact, the upstream activation by agonist and downstream adhesion and aggregation of platelets has been increasingly recognized for its clinical significance in thrombotic analysis [13–15].
The VerifyNow system consists of an instrument and a disposable assay chip for measuring platelet aggregation. The instrument is an automated turbidimetry-based optical detection system. The disposable assay chip consists of microfluidic channels, a heating chamber and four test chambers. Each test chamber includes a magnetic steel ball and a reagents-clustered balls including fibrinogen-coated beads, ADP, and PGE1 as an antagonist. In the VerifyNow, the concentration of ADP is 20μM and that of PGE1 is 22 nM. These reagents were provided in a pellet form in each chamber. When a citrated whole blood sample is automatically filled into a sample chamber, a magnetic ball mixes the reagent pellet with the blood sample. Activated platelets tend to aggregate with fibrinogen-coated microparticles via glycoprotein IIb/IIIa receptors. The VerifyNow-P2Y12 assay results are reported in either PRUs or percent inhibition (%INH). According to the Guro Hospital guidelines, normal controls are defined as PRU > 194 and who do not take P2Y12 inhibitor, whereas positive groups are defined as %INH > 10 and who take P2Y12 inhibitor. According to the manufacturer’s guideline, any values of PRU < 180 were considered abnormal or indicative of P2Y12-inhibited platelet function.
Statistical analysis
The sensitivity and specificity were analyzed considering the results of VerifyNow as reference. The pairwise agreement between the two assays was assessed using Cohen’s kappa coefficient [16]. All statistical analyses were performed using MedCalc version 12.1.4 software (MedCalc Software, Mariakerke, Belgium).
Results
Descriptive characteristics and hematologic parameters
A total of 87 male and 36 female patients aged 63.9±9.7 years (mean±1SD) were included (Table 1). Among them, 47, 42, and 65 patients were diagnosed with hypertension, diabetes, and dyslipidemia, respectively. The clinical characteristics of the patients are shown in Table 1. The platelet count was 247±57×109/L (mean±1SD). Thirty-three patients were found to use aspirin alone, while thirteen patients were taking only P2Y12 inhibitors, namely Plavix (75 mg) and clopidogrel (75 mg). The number of patients taking both aspirin and P2Y12 was 50. Thirty-three patients 33 and 63 were taking aspirin and P2Y12 inhibitors, respectively. There were two types of P2Y12 inhibitors: Plavix (75 mg) and clopidogrel (75 mg).
Baseline patient characteristics
Baseline patient characteristics
Continuous data are shown as mean±1SD.
Anysis-P2Y12 measured MDs in two groups of patients not using P2Y12 inhibitors (negative control) and patients using P2Y12 inhibitors (positive group) (Table 2). The mean values in the negative control and positive group were 182.0±30.4 mm and 264.9±12.0 mm, respectively. The p-value between these two groups was < 0.001. Similarly, the mean values of VerifyNow PRU in the negative control and positive group were 162.0±50.6 and 259.0±38.9, respectively, and the corresponding p-value was 0.042. Additionally, those of VerifyNow %INH in the negative control and positive group were 28.7±18.7 and 0.08±0.64, respectively, and the corresponding p-value was < 0.001.
Comparison of migration distances between negative control and patients using P2Y12 inhibitors
Comparison of migration distances between negative control and patients using P2Y12 inhibitors
Abbreviation: SD, standard deviation.
The sensitivity and specificity of Anysis-P2Y12 were analyzed using the VerifyNow-P2Y12 assay as the reference. As described earlier, the negative control group determined with VerifyNow PRU, showed PRU > 194, as shown in Fig. 2(a). Among them, Anysis-MD identified the negative control group with MD < 225 with a specificity of 88.7% (95% CI, 73.5%–92.4%). In addition, the positive group detected with VerifyNow-%INH (> 10) was also identified with Anysis MD (> 225 mm), as shown in Fig. 2(b), with a sensitivity of 96.6% (95% CI, 88.5%–99.6%). With the provided cutoff value, Anysis-P2Y12 results are further analyzed using the receiver operating characteristic (ROC) curve against those of VerifyNow (Fig. 2(c)). The area under the curve (AUC) for Anysis-200 was 0.959 (95% CI, 0.907–0.986), which indicates that Anysis-P2Y12 has nearly the same performance as VerifyNow P2Y12. It is worth noting that the ROC analysis recommended an optimal cutoff value of Anysis MD, which is 250 rather than 225 of the manufacturer’s value. With the recommended cutoff value, the specificity of the Anysis P2Y12 assay increased from 88.7% to 93.8%, whereas the sensitivity slightly decreased (from 96.7% to 95.0%), as shown in Fig. 2(d).
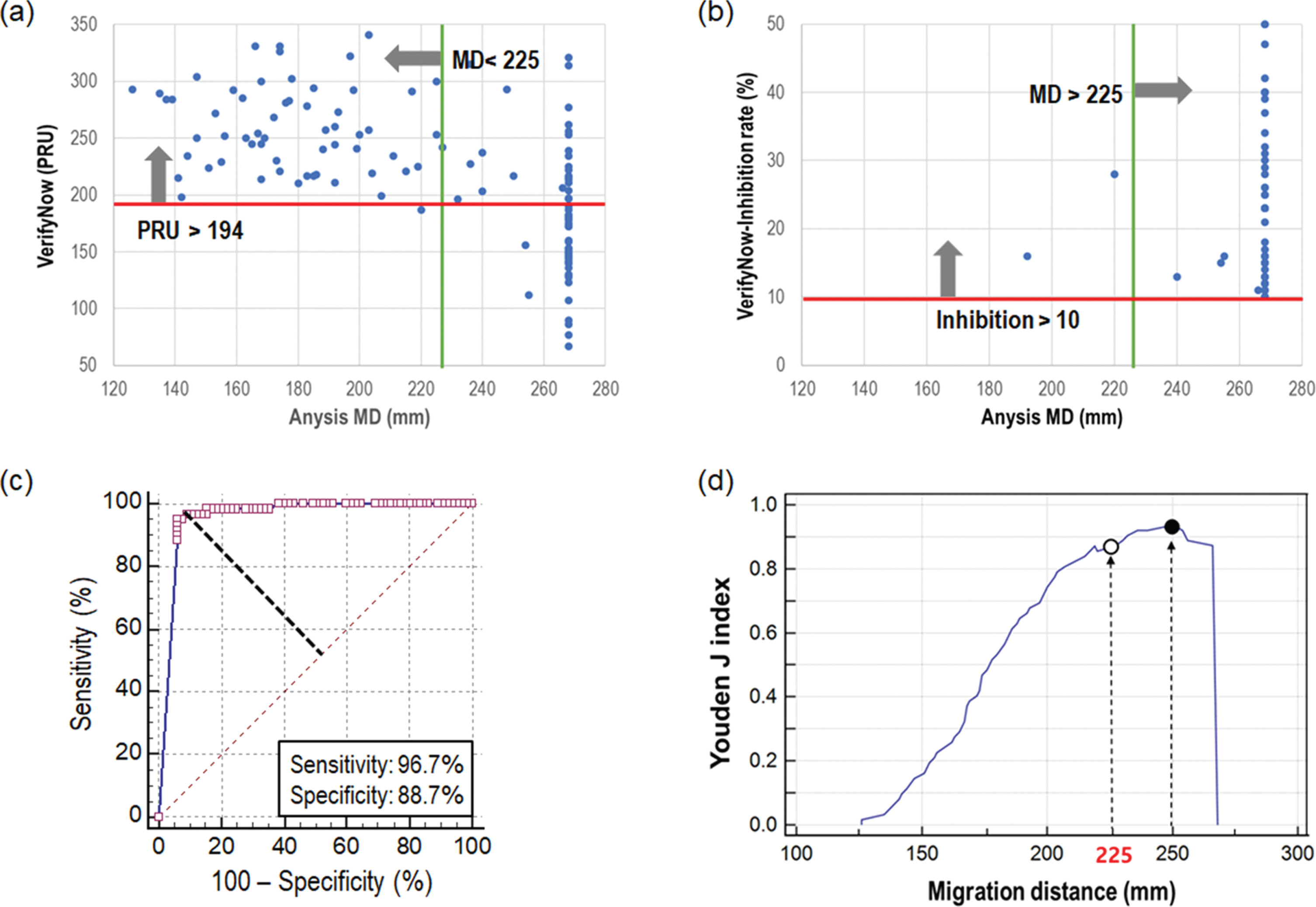
Analysis of specificity and sensitivity of tested results. (a) Determination of specificity with a cutoff of PRU > 194, (b) Determination of sensitivity with a cutoff of %INH > 10. The cutoff value of Anysis-P2Y12 is fixed at MD = 225, (c) Receiver operating characteristic curve comparing Anysis-200 and VerifyNow, (d) Youden J index vs. migration distance. AUC: area under the curve.
The correlation between Anysis-P2Y12 and VerifyNow-P2Y12 was strong (Pearson correlation coefficient r = –0.705, p < 0.001). Furthermore, Cohen’s kappa coefficient between the two devices was 0.761, which is the substantial agreement. In seven repeated measurements with Anysis-P2Y12 assay, the intraclass correlation coefficient was 0.960 (95% confidence interval [CI], 0.948–0.970), confirming the high reproducibility.
Of the 63 patients who used P2Y12 inhibitors, the low-response rates (LRRs) of the P2Y12 inhibitor are compared between the two devices (Table 3). The LRR is 36.5% (23/63) with the VerifyNow %INH cutoff (< 10%) and 25.4% (16/63) with the VerifyNow PRU cutoff (> 194). The LRR of the P2Y12 inhibitor is only 5.9% (5/63) with Anysis-200 MD (> 225 mm).
Measurement comparison of patients using P2Y12 inhibitor between (a) VerifyNow and (b) Anysis-200
There is a clinical need for a reliable test of platelet response to P2Y12 therapy as a guide to individualized dosing regimens. Platelet test results are frequently contrasting to clinical outcomes; thus, the overall clinical efficacy of the P2Y12 test is questionable [3–6]. This clinical confusion may be caused by the cutoff value to determine the low response to the P2Y12 inhibition therapy [3]. The test results of VerifyNow-P2Y12 are described in either PRU or %INH, which may be selectively chosen and used in combination. Even though the cutoff value of the VerifyNow-P2Y12 test is given as 180 PRU according to the manufacturer’s guidelines, many hospitals have their own cutoff values based on clinical validation [3]. Furthermore, the different clinical outcomes reported between the races with potent P2Y12 inhibitors may be related to racial differences in pharmacokinetic and pharmacodynamic profiles [17].
Therefore, we adopted our hospital guideline of PRU > 194 for normal control and %INH > 10% for the experiment group, which yields sensitivity and specificity of 96.7% and 88.7%, respectively (Fig. 2). The present cutoff is a combination of PRU and %INH, considering each diagnostic capability performance of normal and abnormal groups. This is similar to that reported in [18], where a combination of two indexes (PRU and %INH) resulted in excellent prediction performance in patients with ACS undergoing PCI compared to a single use of either PRU or %INH. In general, these two indexes of PRU and %INH are inversely proportional to each other and frequently agree for diagnostic decisions. For instance, with a reference of PRU = 194, the sensitivity and specificity of Anysis-P2Y12 were 91.5% and 80.5%, respectively and with PRU = 180, those were 78.3% and 89.7%, respectively.
As given in Table 3, LRRs of P2Y12 inhibition therapy were 36.5% in VerifyNow and 5.9% in Anysis. However, the biological definition of low-response to P2Y12 inhibitors remains controversial. A previous study reported that the assessment of platelet function inhibition by P2Y12 inhibitors is highly test method-dependent and have poor agreement between different platelet assays [19, 20]. For instance, the rates of non-responders were 13% with PAP4 Aggregometer (Biodata Corporation, France), 39% with Platelet VASP (Stago, France), and 33% with VerifyNow [19]. These different LRRs are mainly due to the different test methods adopted in each device. Since massive clinical studies such as the MACE [18], OPTIMIZE, and EXCELLENT trials [20–22] have adopted VerifyNow, the results of the low response to P2Y12 inhibitor might have been overestimated for decades.
It is worth noting that the initial low responder rate (23.6%) was significantly reduced to 5% when the maintenance dose was doubled [23]. Both the P2Y12 assays of VerifyNow and Anysis used the same reagents, such as ADP as the agonist and PGE1 as the antagonist. ADP activates the platelets by binding the ADP molecules to purinergic receptors P2Y1 and P2Y12 on the platelet membranes, whereas PGE1 blocks the P2Y1 receptor, preventing ADP-induced platelet activation. Both ADP and PGE1 work in a concentration-dependent manner [27, 28]. Thus, the appropriate combination of ADP and PGE1 allows the precise examination of the P2Y12 inhibitor response. The ADP concentration in the VerifyNow was 20μM compared to 6.3μM in the Multiplate analyzer (Roche Diagnostics, Basel, Switzerland) and 2.0μM in the Anysis. Since the ADP concentration in VerifyNow is 10-folds higher than that in the Anysis, the same dose of P2Y12 inhibitor (for instance, 75 mg clopidogrel) may not sufficiently block the P2Y12 receptor from external ADP-induced activation. Thus, the LRR of P2Y12 might be relatively high compared to that obtained via the Anysis assay. Meanwhile, the PGE1 concentration in VerifyNow is 22 nM versus 9.4 nM in Multiplate and 0.6 nM in Anysis. Even though there are significant differences in the PGE1 concentration between the assays, as per Hulshof et al. (2020) [29], such differences do not influence the correlation between the P2Y12 assays.
Because the conventional platelet analyzers, including VerifyNow, are strongly dependent on Hct [24, 25], correcting for hematocrit is highly recommended for an accurate diagnosis. Hence, we also examined the effects of Hct on the PRU of VerifyNow and MD of Anysis system. As shown in Fig. 3(a), PRU showed a strong dependence on Hct due to the optical turbidity operating principle. However, the present MD is not affected much by Hct in the tested range (32%–50%). Similar results were reported in our previous study [12]. Therefore, the results of Anysis-P2Y12 measurement does not require any correction for Hct and can directly use the output value.
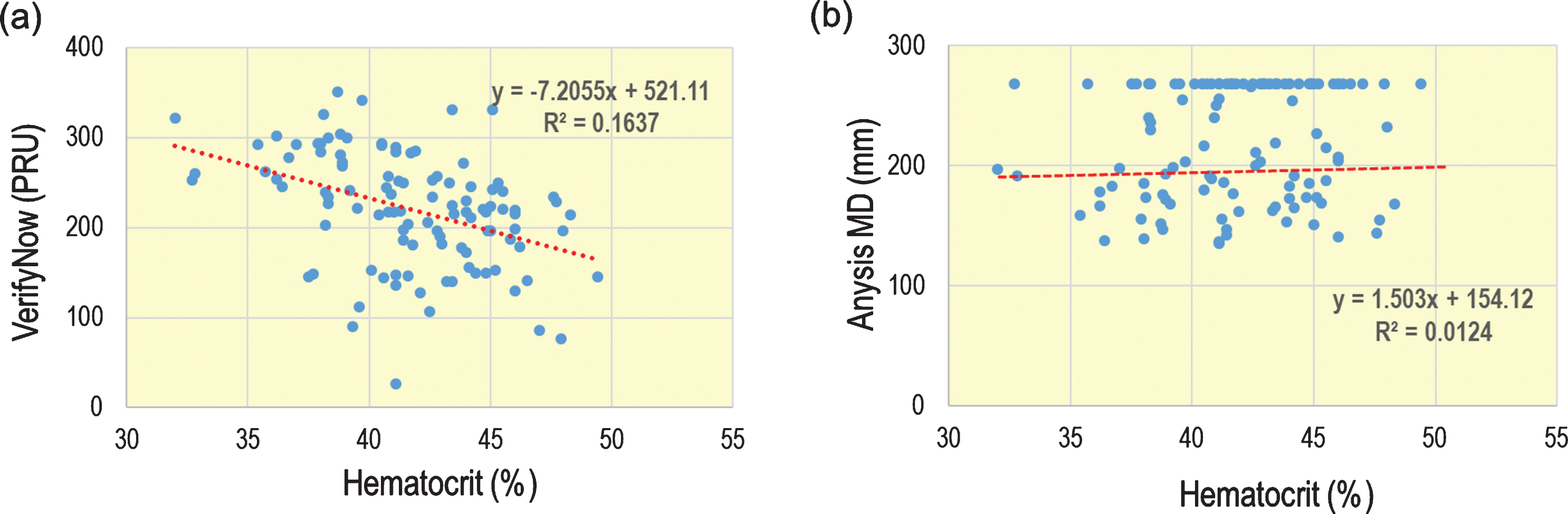
Effect of hematocrits on (a) VerifyNow-PRU and (b) Anysis MD.
The present study confirmed that the performance of the newly developed platelet function assay Anysis-P2Y12 was equivalent to that of VerifyNow-P2Y12 in terms of sensitivity and specificity. Owing to the adoption of innovative technologies, Anysis-P2Y12 is one of the most user-friendly antiplatelet assays and can provide rapid and precise results at any clinical environments. Cohen’s kappa coefficient (κ= 0.761) and Pearson correlation coefficient (r = –0.705) confirm that Anysis-P2Y12 has a good agreement with VerifyNow-P2Y12, having equivalent accuracy and precision. Further, the proposed antiplatelet assay can significantly improve diagnosis by identifying patients who do not respond adequately to P2Y12 inhibiting drugs to prevent thrombosis and replace drugs with other effective treatments.
P2Y12 low-responders were defined as having values of %INH < 10 according to the internal hospital guidelines. However, the cutoff values for distinguishing responders from non-responders are based on the results of studies with relatively small sample sizes. Therefore, these cutoffs should be used with utmost care. Nevertheless, in this study, the sensitivity and specificity of Anysis-200 were analyzed considering the results from VerifyNow as reference. Moreover, the comparison between VerifyNow and Anysiswas made only with respect to P2Y12. Lastly, in the elderly (> 75 years), agonist-induced platelet aggregation is reduced due to the chronic increase in the activation of circulating platelets [26]. Therefore, care should be taken when interpreting the analysis of platelet function in these populations.
Footnotes
Acknowledgments
This research was supported by the Seoul R&D Project (no. BT200171).