
Abstract
AIM:
To explore the diagnostic ability of contrast-enhanced ultrasound (CEUS) in distinguishing intrahepatic cholangiocarcinoma (ICC) from hepatocellular carcinoma (HCC).
MATERIALS AND METHODS:
PubMed, EMBASE, Cochrane Library, and Web of Science were systematically searched for studies reporting the diagnostic accuracy of CEUS in differentiating ICC from HCC. The diagnostic ability of CEUS was assessed based on the pooled sensitivity, specificity, diagnostic odds ratio (DOR), positive likelihood ratio (PLR), negative likelihood ratio (NLR) and area under the curve (AUC) with 95% confidence intervals (CIs). The methodologic quality was assessed by the QUADAS-2 tool. Subgroup analyses, meta-regression and investigation of publication bias were performed to identify the source of heterogeneity.
RESULTS:
A total of eight studies were included, consisting of 1,116 patients with HCC and 529 with ICC. The general diagnostic performance of CEUS in distinguishing ICC and HCC were as follows: pooled sensitivity, 0.92 (95% CI: 0.84–0.96); pooled specificity, 0.87 (95% CI: 0.79–0.92); pooled PLR, 7.1 (95% CI: 4.1–12.0); pooled NLR, 0.09 (95% CI: 0.05–0.19); pooled DOR, 76 (95% CI: 26–220) and AUC, 0.95 (95% CI: 0.93–0.97). Different liver background may be a potential factor that influenced the diagnostic accuracy of CEUS according to the subgroup analysis, with the pooled DOR of 89.67 in the mixed liver background group and 46.87 in the cirrhosis group, respectively. Six informative CEUS features that may help differentiate HCC from ICC were extracted. The three CEUS features favoring HCC were arterial phase hyperenhancement (APHE), mild washout and late washout (>60s); the three CEUS favoring ICC were arterial rim enhancement, marked washout and early washout (<60s). No potential publication bias was observed.
CONCLUSION:
CEUS showed great diagnostic ability in differentiating ICC from HCC, which may be promising for noninvasive evaluation of these diseases.
Keywords
Introduction
Primary liver cancer remains a universal health burden as it is the fourth leading cause of cancer-related deaths worldwide [1, 2]. Hepatocellular carcinoma (HCC) makes up roughly 80% of the primary liver cancer, while Intrahepatic cholangiocarcinoma (ICC) occurs at a rate of approximately 15% [3, 4]. The incidence of ICC is increasing in the past few decades [5]. Viral hepatitis and chronic cirrhosis are the well-known risk factors of HCC; however, some research also suggest strong link between cirrhosis or chronic hepatitis and ICC [6]. According to a study [7], ICC accounts for 2–5% of all new nodules in cirrhotic patients. Although they share similar risk factors, the prognosis and treatment planning of HCC and ICC differ significantly. Patients with ICC tend to have poorer outcomes than those with HCC [8, 9]. The treatment options such as local ablative therapy and liver transplantation, which is recommended for patients with HCC are not suitable for patients with ICC. Radical surgical resection remains the sole curative treatment option for ICC [10, 11]. Thus, it is clinically necessary to pre-operatively differentiate ICC from HCC, for optimal treatment planning and prognostic prediction.
Contrast-enhanced ultrasound (CEUS) has been applied to characterize hepatic lesions for more than 10 years. It allows a continuous view of the enhancement pattern and the real-time evaluation of the vascular characteristics of tumors. A prospective multicenter study of German Society for Ultrasound in Medicine (DEGUM) assessed the diagnostic ability of CEUS in detecting HCC in high-risk patients, which enrolled 321 patients from 43 centers. The result confirmed that CEUS possessed excellent diagnostic accuracy for the noninvasive diagnosis of HCC in high-risk patients [12]. It was endorsed by the American Association for the Study of Liver Diseases (AASLD) and the European Association for the Study of the Liver (EASL) as a second-line imaging modality to generate a diagnosis of HCC when the final diagnosis of contrast-enhanced computed tomography (CE-CT) or contrast-enhanced magnetic resonance imaging (CE-MRI) are inconclusive or contraindicated. However, it was removed in the 2010 update due to the theoretical concerns for potentially misdiagnosing ICC as HCC in cirrhotic liver [13, 14]. Controversies remain regarding the decision to remove CEUS was mainly based on a small (21 patients), retrospective and monocentric study. According to the study [15], intrahepatic cholangiocarcinoma (ICC) in cirrhotic patients displayed similar enhancement patterns (arterial-phase hyperenhancement and portal-delayed phase wash-out) to that of HCC on CEUS (47.6%, 10/21).
To investigate the diagnostic accuracy of CEUS in differentiating ICC from HCC, a variety of studies have been performed. However, so far there have been no meta-analyses evaluated the diagnostic abilities of CEUS in making different diagnosis between HCC and ICC. Therefore, the present meta-analysis summarized all current results to determine the ability of CEUS in distinguishing these two diseases. The imaging features favoring a diagnosis of HCC or ICC were also identified with the aim to help differentiate them.
Material and methods
This meta-analysis was conducted base on the guidelines of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) of Diagnostic Test Studies [16]. We registered the protocol in the International Prospective Register of Systematic Reviews (PROSPERO No. CRD42020206751).
Literature search strategy
A comprehensive literature search of Pubmed, Embase, Web of Science, and the Cochrance library from the inception to Sept. 20, 2020 was performed to identify relevant articles evaluating the diagnostic accuracy of CEUS in distinguishing HCC and ICC. The search strategy including the following keywords: (hepatic carcinoma OR hepatic tumor OR hepatic cancer OR hepatic neoplasm OR hepatocellular cancer OR hepatoma OR hepatocarcinoma or hepatocellular neoplasm OR hepatocellular carcinoma OR hepatocellular tumor OR hepatic cell carcinoma OR liver tumor OR liver cancer OR liver neoplasm OR liver carcinoma OR HCC) AND (Intrahepatic cholangiocarcinoma OR ICC OR IHCC) AND (contrast-enhanced ultrasonography OR contrast-enhanced US OR contrast-enhanced ultrasound OR CEUS). The bibliographies of related articles were also searched manually for additional eligible studies. There are no restrictions concerning the study setting or publication date.
Study selection
After removing duplicate articles, the titles and abstracts of articles were screened by two investigators independently for potential eligibility. The full text of the included abstracts got further screened for final analysis. Any conflicts were resolved by discussion with a third investigator. Studies would be included if they fulfilled the flowing inclusion criteria: 1) evaluated the diagnostic performance of CEUS in differentiating ICC from HCC; 2) the final diagnosis was histopathologically confirmed; 3) had sufficient data to reconstruct a 2×2 contingency tables. Studies would be excluded if they were not in English or did not pertain to the field of interest. Types of literature such as review articles, editorials, letters, comments, conference abstracts, case reports and series, meta-analyses and unpublished articles were also excluded. When studies possessed overlapping patients and data, only the study with the largest study population was included.
Data extraction
The following data were retrieved from the selected studies by two independent
reviewers: Study
characteristics, including first author’s name, publication years, country of
origin, patient recruitment durations, study design, reference standard, blind
method and the number of observations; patient characteristics, including the number of patients and lesions, age,
gender ratio, average lesion size and final diagnosis; CEUS characteristics, including the equipment, mode, mechanical
index, the type of contrast agent and its volume; the true-positive, false-positive, false-negative, and
true-negative results which will reveal the diagnostic performance of CEUS were also
extracted.
Any discordance between the two reviews was resolved in consensus with the third reviewer.
Quality assessment
Two reviewers independently assessed the quality of the eligible studies according to the Quality Assessment of Diagnostic Accuracy Studies (QUADAS) tool using Revman, version 5.3.5 (The Nordic Cochrane Centre, Copenhagen) [17]. A third reviewer was available for resolving the discrepancies between the two reviews.
Statistical analysis
A bivariate random effect model was utilized to calculate the pooled sensitivity, specificity, positive likelihood ratio (PLR), negative likelihood ratio (NLR) and diagnostic odds ratio (DOR) with corresponding 95% confidence intervals (CIs), with a generation of forest plots. Besides, the summary receiver operating characteristic (SROC) curve were plotted and the areas under curve (AUC) were computed to get a summary estimates of the diagnostic ability of CEUS. Afterward, the heterogeneity was evaluated by using the Cochran Q test and inconsistency index I2, Heterogeneity was classified as low (I2 = 0% –30%), moderate (I2 = 30% –50%), or substantial (I2 > 50%). The Spearman correlation coefficient was applied to determine potential threshold effect, such that p > 0.05 indicated no significant threshold effect. We also performed subgroup analysis and meta-regression analysis in liver background (mixed liver background vs. cirrhotic liver) and sample size (>100 [sample size median] vs. <100] to further explore the source of heterogeneity. Publication bias was evaluated using the Deeks’ funnel plot, with p < 0.1 indicated significant asymmetry. Statistical analyses were performed using Meta-Disc (version 1.4) and STATA version 15.0 (STATA Corp., College Station, TX, USA) with midas and metandi modules.
Results
Study identification and selection
A total of 562 potentially relevant studies were found in the initial search, of which 233 from Pubmed, 236 from Embase, 82 from Web of Science and 11 from the Cochrane Library. After 143 duplicates were removed, 419 studies underwent titles and abstracts review and 405 publications get further excluded for the following reasons: review articles (120), case reports [32], guidelines [5], conference abstracts [43], letters [8], animal experiments [3], not in English [1] and not in the field of interest (193). Fourteen articles were retained for full-text screening and six articles get further deleted for the reason of insufficient data for calculating estimates [3] and duplicated data series [3]. Finally, eight studies [18–25] were included. The detailed flow chart of studies selection is presented in Fig. 1.
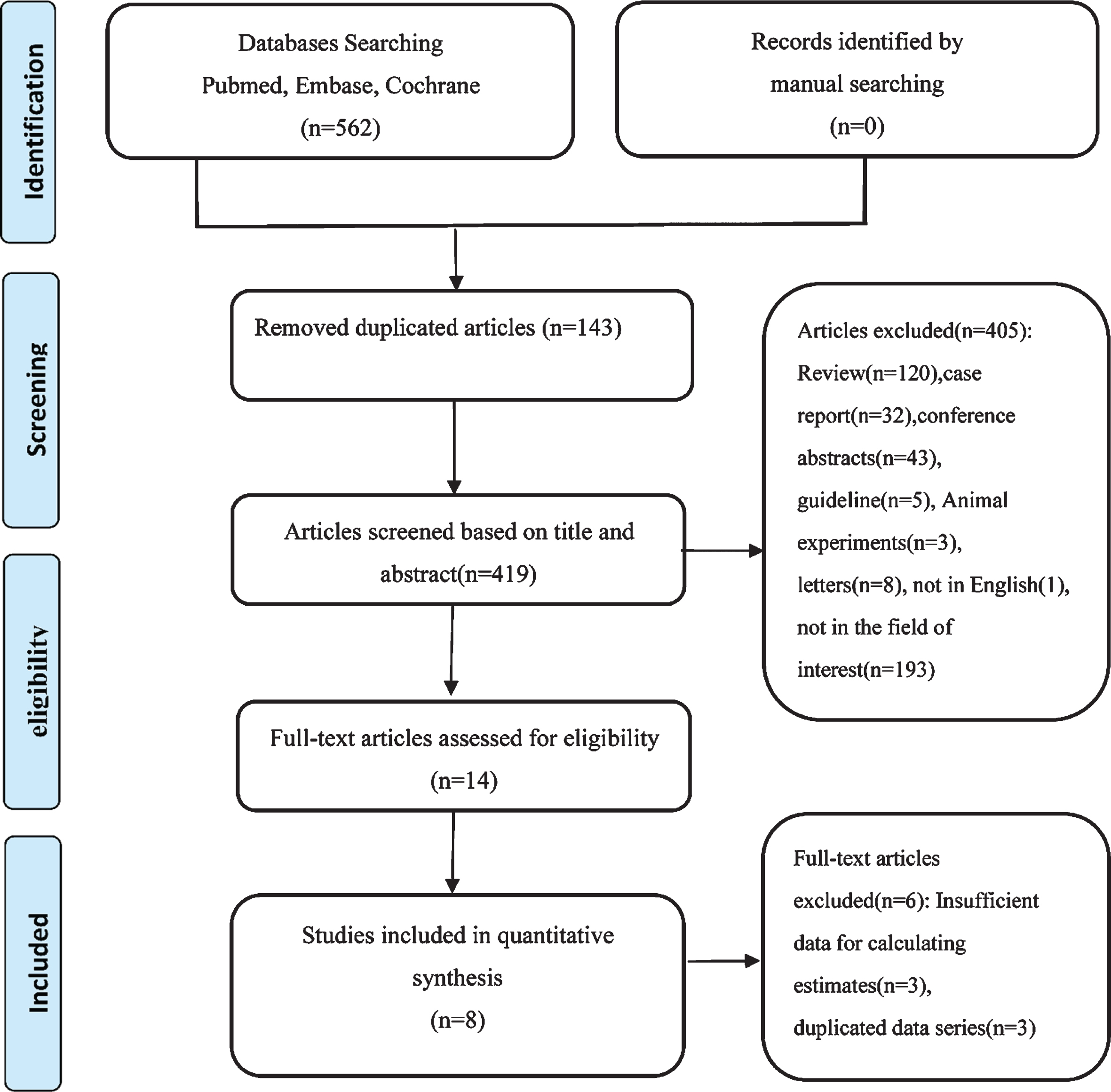
Flow chart of study selection process.
The basic characteristics of selective studies are shown in Table 1. The publication years ranged from 2014 to 2020. Among the selective studies, two studies [18, 20] enrolled only patients with cirrhosis, six studies [19, 21–25] enrolled patients with different liver backgrounds, including normal liver, cirrhosis and hepatitis. The study designs were retrospectively in seven studies [18–20, 22–25] whereas prospectively in one study [21]. Consecutive patient enrollment and histopathologically confirmed were found in almost all studies. A total of 1,645 patients were included in this meta-analysis, comprising 1,116 patients with HCC and 529 with ICC. The mean age of patients with HCC range from 50.0 to 66.6 years old and the mean size range from 20.00 to 73.00 mm. While among patients with ICC, the mean age range from 49.21 to 67.9 years old and the mean size range from 23.00 to 70.00 mm. Table 2 presented the general detailed characteristics of CEUS. All studies used SonoVue (Bracco, Italy) as the contrast agent, with the volume range from 1.2 to 4.8 ml and the Mechanical Index(MI) <0.4. In all eligible studies, the CEUS images were assessed independently by two radiologists with experience in liver CEUS for at least two years.
Basic characteristics of the eligible studies included in this meta-analysis
Basic characteristics of the eligible studies included in this meta-analysis
No., number; HCC, hepatocellular carcinoma; ICC, intrahepatic cholangiocarcinoma; yrs, years; NC, not clear.
Contrast-enhanced ultrasound (CEUS) characteristics
No., number; CPS, contrast pulse sequencing imaging; CHI, Contrast Harmonic Imaging mode; CHE, Contrast Harmonic Echo; NR, not reported; yrs, years.
The quality of the eligible studies was regarded as moderate or excellent (Fig. 2) after assessing by the QUADAS-2 tool yet several methodological shortcomings contributing to the bias still exist. Two studies [18, 21] without appropriate exclusions might introduce potential selection bias. With regard to the index test, two studies [19, 20] might increase the risk of bias because they used the LR-M of CEUS LI-RADS as diagnostic criteria. Two studies [22, 23] had low applicability with respect to flow and timing given the inclusion of only patients with specific sizes. The reference standard in all studies were regarded as low risk of bias.
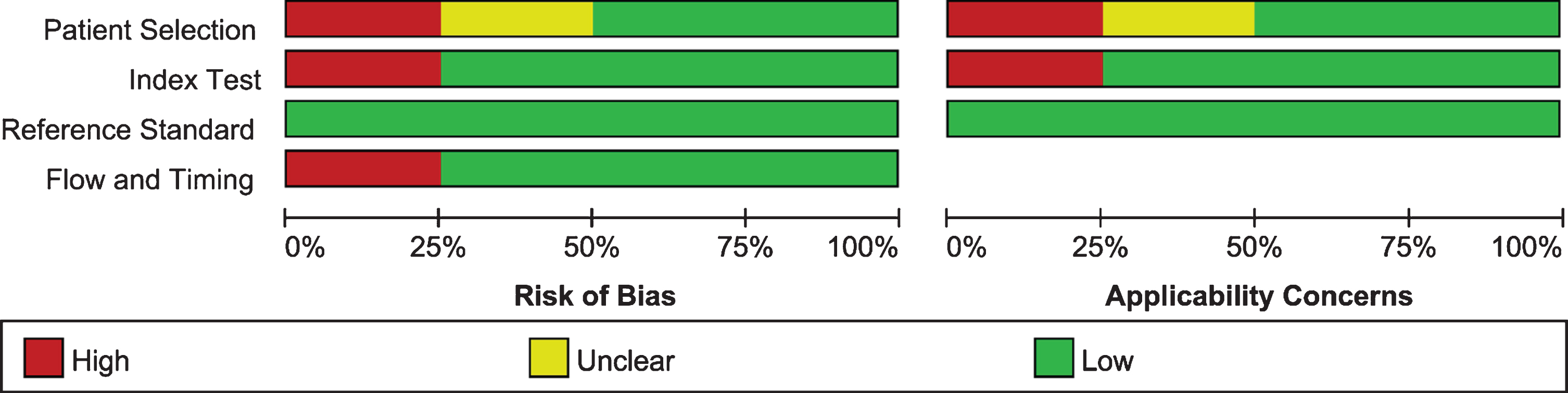
Quality assessment of the included studies.
The pooled sensitivity of CEUS in differentiating ICC from HCC was 0.92 (95% CI: 0.84–0.96) and the pooled specificity was 0.87 (95% CI: 0.79–0.92) (Fig. 4). The summary DOR, PLR and NLR were 76 (95% CI: 26–220), 7.1 (95% CI: 4.1–12.0) and 0.09 (95% CI: 0.05–0.19), respectively. Figure 3 illustrated the SROC curve with AUC to be 0.95 (95% CI: 0.93–0.97). There was no significant correlation between sensitivity and specificity according to the Spearman correlation coefficient (r=–0.238, p = 0.570), which suggested that there was no threshold effect. Significant heterogeneity among the studies were observed in pooling sensitivity (I2 =90.59%, p < 0.01) and specificity (I2 = 94.52%, p < 0.01) (Fig. 4). Sensitivity analysis was performed and one study [25] were excluded, whereas the results were not significantly influenced.

Sensitivity and specificity forest plots of CEUS in differentiating intrahepatic cholangiocarcinoma (ICC) and hepatocellular carcinoma (HCC). The pooled sensitivity and specificity were 0.92 (95%CI: 0.84–0.96) and 0.87 (95%CI: 0.79–0.92), respectively.
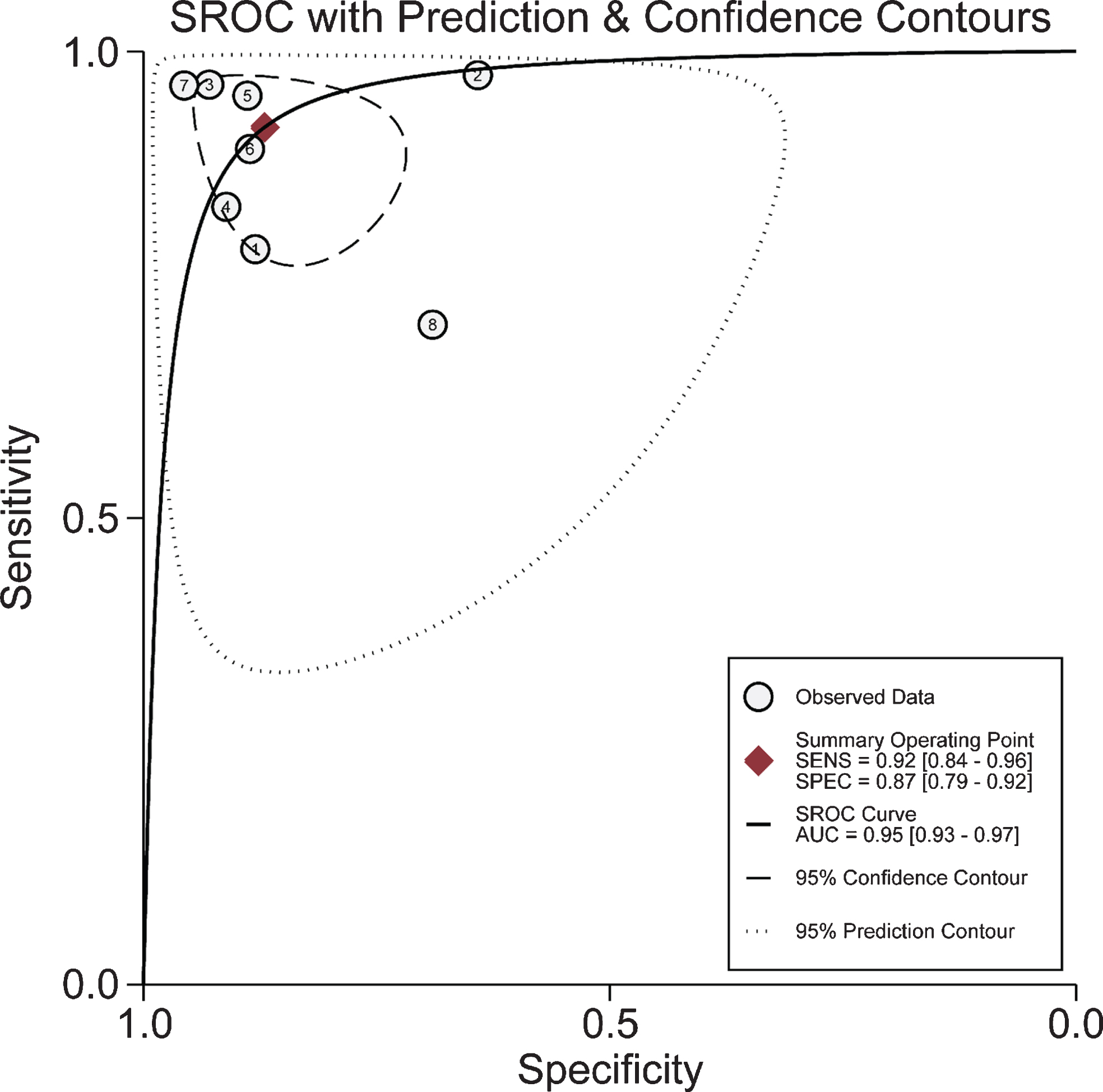
Summary receiver operating characteristic (SROC) curves of contrast-enhanced ultrasonography (CEUS) in distinguishing intrahepatic cholangiocarcinoma (ICC) and hepatocellular carcinoma (HCC).
In our present meta-analysis, we extracted six CEUS features (three CEUS features favoring HCC and three CEUS features favoring ICC), which may be helpful in differentiation ICC from HCC (Fig. 6). Data for the six CEUS features are presented in Table 3. Among the three imaging features favoring HCC, Arterial phase hyperenhancement (APHE) showed high sensitivity (0.93, 95% CI:0.90–0.96) but low specificity (0.39, 95% CI:0.33–0.44). Mild washout was identified in four studies as a useful feature favoring HCC, the sensitivity and specificity were 0.79 (95% CI:0.56–0.91) and 0.56 (95% CI:0.24–0.84), respectively. The imaging feature of late washout (≥ 60 s) revealed high specificity (0.95, 95% CI: 0.91–0.97) while low sensitivity (0.63, 95% CI:0.24–0.90). Among the three CEUS features favoring ICC, the pooled sensitivities of early washout (<60), peripheral rim hyperenhancement and marked washout were 0.95 (95% CI: 0.91–0.97), 0.63 (0.49–0.76) and 0.55 (0.30–0.78), and the pooled specificity were 0.64 (0.25,0.91), 0.96 (95% CI: 0.71–1.0) and 0.96 (95% CI: 0.89–0.99), respectively. High specificity but relatively low sensitivity were observed in the features favoring ICC, except for early washout (<60).
The pooled sensitivity, specificity, diagnostic odds ratio, area under the curve, likelihood ratio, and heterogeneity of individual CEUS features
Data in parentheses are 95% confidence intervals. CEUS, contrast-enhanced ultrasound; HCC, hepatocellular carcinoma; ICC, intrahepatic cholangiocarcinoma; No., number; DOR, diagnostic odds ratio; LR, likelihood ratio.
Subgroup analysis was performed to explore the capabilities of several potential factors in affecting the diagnostic accuracy. DOR integrated data from sensitivity and specificity and can be used to evaluate the diagnostic accuracy of CEUS in different subgroups. As seen in Table 4, liver background and number of lesions both greatly influenced the diagnostic accuracy. The DOR of the mixed liver background group was more improved than the cirrhosis group (89.67 vs 46.87). Great heterogeneity was found in the mixed liver background group (I2 =92.9%), while it was reduced in the cirrhosis group (I2 = 28.3%). The DOR appeared greatly reduced in the small-sample-size group (number of lesions < 100) than in the big-sample-size group (number of lesions≥100; 30.93 vs 90.88). Heterogeneity was almost eliminated in the small-sample-size group (I2 = 0%), while it still existed in the big-sample-size group (I2 = 93.2%). Meta-regression analysis indicated that none of the above-mentioned factors (Table 5) was the major source of heterogeneity.
Subgroup analysis of the DOR of CEUS in the differentiation of ICC and HCC
Subgroup analysis of the DOR of CEUS in the differentiation of ICC and HCC
No., number; CIs, confidence intervals; HCC, hepatocellular carcinoma; ICC, intrahepatic cholangiocarcinoma.
Meta-regression analysis of potential source of heterogeneity
Coeff. coefficient, Std. err. standard error, RDOR relative diagnostic odds ratio; CIs, confidence intervals.
As seen in Fig. 5, the included studies distributed symmetrically in the Deeks’ funnel plot (p = 0.94), indicating that there was no potential publication bias.
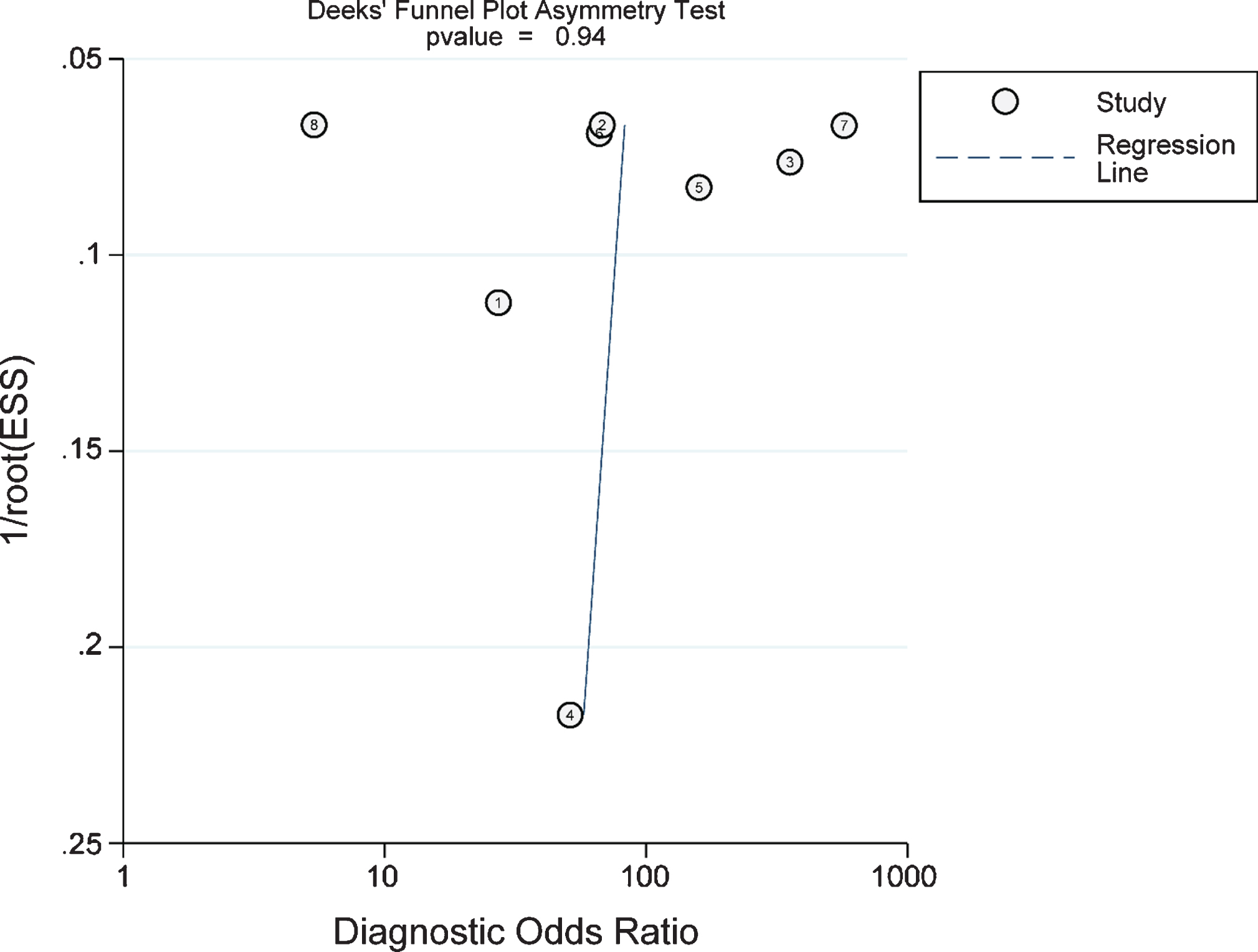
Funnel plot for the evaluation of potential publication bias.
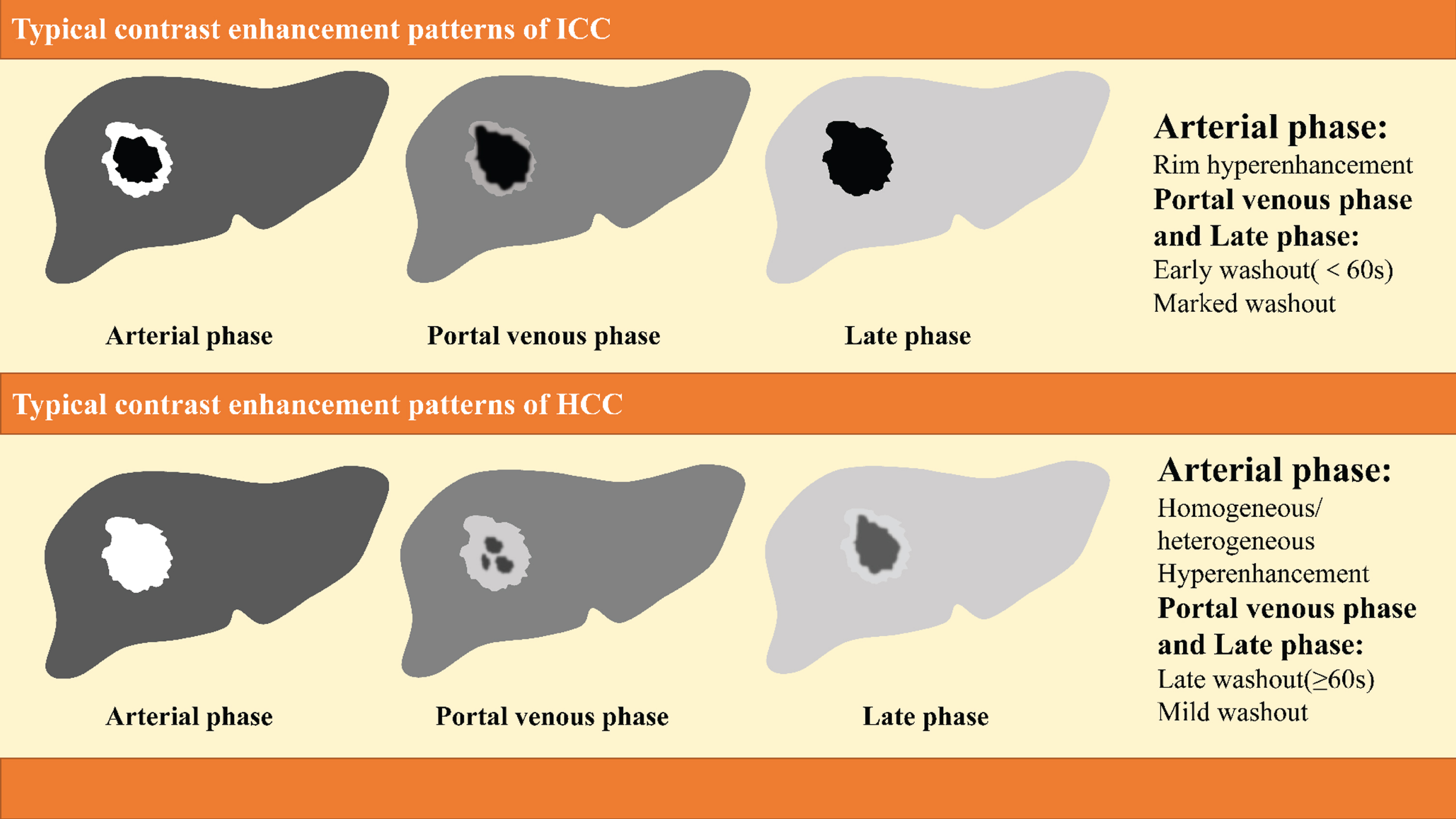
Typical contrast enhancement pattern of intrahepatic cholangiocarcinoma (ICC) and hepatocellular carcinoma (HCC).
Our meta-analysis systematically reviewed eight studies evaluating the diagnostic performance of CEUS in distinguishing ICC and HCC. The results indicated that CEUS possessed high sensitivity (0.92) and specificity (0.87) in differentiating these two diseases. The overall diagnostic ability is high, with the AUC of 0.95. The pooled DOR was 76 which suggested high detection ability. Heterogeneity was observed between studies. Subgroup analysis found that liver background and sample size might be potential sources of heterogeneity; however, meta-regression didn’t support the assumption.
ICC is a primary liver cancer that arises from the biliary epithelium. It shares some similar risk factors to HCC such as liver cirrhosis or chronic hepatitis [26–28]. However, previous studies suggested that the prognosis of patients with ICC is much poorer than those with HCC [8]. The established treatments for HCC, such as liver transplantation or radiofrequency ablation, do not totally apply to patients with ICC [29]. The differential diagnosis of liver nodules on imaging will affect the decision on subsequent work-up and treatment. Thus, it is of critical importance to correctly differentiate ICC from HCC in order to avoid inappropriate treatment.
B-Mode ultrasound (BMUS) is recommended as the surveillance modality in high-risk patients according to the guidelines of the AASLD and the EASL [13, 30]. Although it provides wide available, cost-effective, real-time, and non-invasive detection, the accuracy remains a concern. According to a meta-analysis of Tzartzeva and colleagues, the diagnostic accuracy of BMUS range from 47 to 63% in cirrhotic HCC patients at the early disease stages [31]. Furthermore, it is difficult to distinguish ICC and HCC only base on BMUS because ICC has no specific features on BMUS [29].
With the ability of real-time micro-vascularization visualization, the CEUS technology showed good performance in focal liver lesion characterization, malignancy recognition and exclusion. Modern advanced terminal devices equipped with CEUS technology and contrast harmonic imaging at low energy (low-MI <0.2) enable better penetration to deeper layers with higher resolution and longer contrast enhancement (≥5min). The current contrast agents approved for clinical practice are SonoVue® (Bracco, Italy) and Sonazoid® (GE Healthcare, Norway). Both of the contrast agents consist of a monolayer phospholipid shell encasing inert gas (SF6 and C4F10). A single injection of SonoVue allows 3–5 min enhanced scan of the whole liver. While Sonazoid exhibits an additional Kupffer phase (10∼60min) and allows enough time for scanning the entire liver due to high affinity with Kupffer cells in the liver reticuloendothelial system. Both Sonovue and Sonozoid enable the visualization of the tumor micro-vascularization and contribute to the accurate diagnosis of liver lesions [32, 33]. The development of CEUS perfusion imaging, which standardizes the analysis of enhancement kinetics by using quantification software, strengthens the significance of CEUS in multimodal tumor imaging when comparing with CT and MRI and have exhibited high sensitivity and specificity in assessing focal liver lesions [34, 35]. According to Wildner et al. [36], CEUS perfusion imaging showed good ability to distinguish different malignant liver lesions at peak enhancement and during the washout phases.
In current clinical practice, CE-CT and CE-MRI are also considered as non-invasive imaging modalities for the detection of primary liver cancer. HCC shows typical imaging features such as APHE followed by portal-delayed phase washout on CE-CT or CE-MRI [26]. In characterizing ICC, CT and MRI usually demonstrate arterial rim enhancement and progressive enhancement with no washout in the portal venous phase [37, 38]. However, in some well-differentiated or small-sized HCC, this typical enhanced pattern is not well observed because the arterial tumor vessels have not sufficiently developed [22]. The capacity of CEUS in real-time evaluating the enhancement patterns of a nodule enabled more sensitive detection of APHE than CE-CT or CE-MRI in the early arterial phase [39]. Previous studies have demonstrated that CEUS can characterize nodules showing atypical or non-coincidental typical vascular patterns on CT or MRI and improve the diagnostic accuracy [40]. Hsiao and colleagues [41] performed a trial comparing CEUS, CE-CT and CE-MRI in 66 patients suspected of having small liver tumors (<3 cm). The DOR of CEUS, CE-MRI and CE-CT were 52.8 (95% CI: 11.4–243), 29.29 (95% CI: 7.36–116), and 19.43 (95% CI: 5.44–69.4), respectively. This study result indicated that CEUS outperformed CE-CT and CE-MRI in diagnosing small liver tumors. In our meta-analysis, CEUS demonstrated strength in differentiating ICC from HCC, with a high sensitivity (0.92,95% CI: 0.84–0.96) and specificity (0.87, 95% CI: 0.79–0.92). The AUC (0.95, 95% CI: 0.93–0.97) was close to 1 which mean the high detection ability. Given the practicality and safety, CEUS is nonradiative and can be performed in patients with renal failure because the contrast agent is discharged through the respiratory tract without passing through the liver and kidney. CEUS can also be performed on patients who cannot take MR examination due to health conditions or metal implants. Therefore, CEUS may also be an alternative method in distinguishing ICC from HCC for those show atypical vascular patterns on CT or MRI. However, limitations of CEUS can not be ignored, including limited capability of disease staging and poor performance in some patients with a poor sonic window such as severe steatosis, advanced cirrhosis or obese patients [42]. Further studies are needed to compare the diagnostic performance of CEUS, CT and MRI in the differentiation of ICC from HCC.
Subgroup analyses indicated that liver background and number of lesions might affect the diagnostic performance. In our meta-analysis, the DOR of the mixed liver background group (89.67, 95% CI: 12.77–629.94) appeared more improved than the cirrhosis group (46.870, 95% CI: 20.05–109.55), which indicated CEUS show better detection ability in the mixed liver background group than the cirrhosis group. This finding may be associated with the fact that ICC with a cirrhotic background tends to show an enhancement pattern similar to HCC more often than with the mixed liver background, which might lead to the decrease of discriminative power. According to a study, approximately 50% of ICC in cirrhosis display global APHE followed by washout in CEUS [43]. Yuan et al. demonstrated that 37.5% of ICC showed rim-like enhancement in the arterial phase on CEUS, while 62.5% ICC exhibited non-rim-like enhancement, of which more patients were found with chronic viral hepatitis and cirrhosis [44]. Yuan’s conclusion in consistent with another study by Liu et al, which also found that APHE was more frequently observed in ICC with cirrhosis than with normal liver (46.7% vs 20.8%, p < 0.05), while rim hyperenhancement was more common in ICC with normal liver than with cirrhosis (26.4% vs 4.4%, p < 0.05) [45].
The big-sample-size group (≥100 lesions) revealed a predominance in differentiating ICC from HCC than the small-sample-size group (<100 lesion), which may due to the fact that sonographers in large medical centers with large group of patients tend to have richer experience to distinguish ICC from HCC in clinical practice [46].
Many previous studies revealed that ICC shows rim enhancement in arterial phase followed by marked washout in portal-delayed phase, while HCC display APHE followed by mild washout on CEUS [7, 43]. The CEUS features of HCC and ICC in the enrolled studies are partly in agreement with characteristics mentioned above. Some HCC nodules can even show intra-tumoral blood vessels. We extracted several CEUS features favoring a diagnosis of HCC or ICC. The three CEUS features favoring HCC were arterial hyperenhancement (APHE), mild washout, and late washout (>60s). Unlike HCC, three CEUS features favoring ICCs in this study were rim enhancement in arterial phase, early washout (<60s) and marked washout. These features are partly consistent with the CT or MRI image features. APHE was seen in most HCC lesions while most ICC showed rim hyperenhancement in the arterial phase, this phenomenon may be related to the distribution of malignant cells. Hyper-enhanced areas in the tumor always correspond to an increased density of malignant cells [23, 47]. Xu et al. [48] compared the CEUS findings with pathological findings of 32 ICC. Their work showed that the rim enhancement pattern of ICC is associated with a high degree of malignant cell proliferation in the periphery while necrosis or fibrosis in the center of the tumor on pathology.
Washout is defined as the reduction of enhancement in the nodules when compared with the liver parenchyma, which contained two critical aspects: onset (late vs early) and degree (mild vs marked). The contrast washout of ICC was much more complete than in HCC. Mild washout was identified in four studies as a useful feature favoring HCC, while marked washout was observed in five studies favoring ICC. In terms of the onset time of washout, our studies indicated that ICC (<60s) is prone to wash out earlier than HCC (>60s). These discrepancies may due to HCC have richer blood supply such as hepatic artery, portal venous, abnormal artery, and micro-vascularization than ICC which are predominant hepatic artery supplies [49]. The HCC and ICC features derived from our study were consistent with the LR-5 and LR-M category of CEUS Liver Imaging Reporting and Data System (LI-RADS), which also confirmed the value of our study. LI-RADS criteria for CEUS were proposed to standardize the interpretation of the liver imaging and the reporting of results, which will assist radiologists in the categorization of liver lesions. According to the CEUS LI-RADS, LR-1 indicated that the nodules are definitely benign, LR-2 means probably benign, LR-3 means the lesions have probability to be malignancy, LR-4 suggests the nodule probably be HCC, LR-5 indicates that the lesions is definitely HCC, and LR-M reveals that the nodule definitely be malignant but not HCC specific [50]. Apart from ICC, many other malignancies such as atypical HCC and Combined Hepatocellular Cholangiocarcinoma (CHC) can also be included in the LR-M category and show the imaging features include a mixture of those seen in HCC and ICC. Thus, a biopsy may still be necessary for the nodules that show atypical contrast-enhanced patterns.
Marked heterogeneity among studies was observed. To resolve this issue, we combined sensitivity analysis, subgroup analysis along with meta-regression to find the potential sources of heterogeneity. Subgroup analysis prompted that liver background and number of lesions might contribute to the heterogeneity. However, the result of synthetic regression analysis did not support the above results. Thus, the source of heterogeneity in this meta-analysis couldn’t be identified. This might be due to the study data in this study were from different regions and affiliations. In addition, there was no prespecified diagnostic criterion for sonographers to make the diagnosis. Sonographers with various experience might get different diagnosis when evaluating the contrast-enhanced ultrasonography imaging. Given that, the heterogeneity within our study remains a concern.
The present study has the following potential limitations: First, our study only included a relatively small number of studies. Several studies were excluded due to insufficient data for calculating the pooled sensitivity and specificity. Second, this study mainly enrolled Asian population. Further investigation in different population was required. Third, we only performed subgroup analysis by different liver background and number of lesions, further subgroup analyses based on the size of the lesions, localization, AFP level or CA199 level cannot be performed due to incomplete reporting at the primary study. Since all included studies performed CEUS with the contrast agent (CA) of SonoVue, it is unclear whether the CA type might affect the diagnostic performance.
Conclusions
In conclusion, our meta-analysis suggests that CEUS has outstanding diagnostic value for differentiating ICC from HCC with both high sensitivity and specificity. As for the distinctive imaging features, arterial hyperenhancement, mild washout, and late washout (>60s) were useful features for HCC, while arterial rim enhancement, marked washout and early washout (<60s) were informative features for ICC. The summary of CEUS features present herein may assist in characterizing primary liver tumors.
Footnotes
Acknowledgment
This study was supported by Shanghai Municipal Key Clinical Specialty (Grant/Award Number: shslczdzk03501).
Conflict of interest
The authors declare no conflicts of interest.