
Abstract
BACKGROUND:
Edema and subjective leg complaints (e.g. pain, heaviness) after long standing or sitting, are defined as orthostatic leg complaints or occupational edema. Compression hosiery should help to prevent or decrease those symptoms.
OBJECTIVE:
Assess the effects on leg discomforts and leg volume and wearing comfort in two medical below-knee compression stocking types (A vs. B) with an interface pressure of 18 –20 mmHg and a below-knee-low-pressure support stocking (LPSS) with an interface pressure of 8–10mmHg (C).
METHODS:
Two different types of below-knee medical compression stockings and a LPSS were examined in this randomized, blinded, crossover trial in volunteers having leg discomforts and edema after being in an upright position during the day. Participants were divided into two cohorts, and each type of stocking was worn for three consecutive days in one week with a subsequent washout phase. The assessment of effects and wearing comfort was ascertained by questionnaires. Volume changes in the lower leg were measured with the Bodytronic 600® (Bauerfeind AG, Zeulenroda, Germany).
RESULTS:
A significant reduction of lower leg volume (mean stocking A: 204.7 ml; mean stocking B: 153.5 ml; mean stocking C: 48.2 ml) and a significant reduction of the life-quality dimension leg-complaints (p < 0.0001) was achieved by all three types of stockings. Compared to the LPSS both compression stockings decreased the lower leg volume significantly more (p < 0.001) and had a significant better fit (p < 0.001).
CONCLUSION:
Below-knee medical compression stockings with an interface pressure 18–21mmHg and LPSS with an interface pressure of 8–10 mmHg reduce significantly occupational orthostatic edema and leg discomforts which are due to long standing and sitting activities.
Introduction
People with increased standing and sedentary activities, especially in their working life, often suffer from subjective leg complaints, such as feelings of heaviness, tightness and tingling of the legs combined with objectifiable leg edema. Women are usually more affected than men [1, 2]. Long periods in an upright and seated position can cause stasis in the venous vascular system in the legs, resulting in an increased intravascular pressure, particularly in the postcapillary venules. Due to the increased venous pressure, this chronic stasis leads to raised pressure-related ultrafiltration in the capillary bed with the formation of interstitial edema [3].
Leg edemas arising due to occupational orthostatic load when working mainly in a standing and/or sitting posture are also called occupational orthostatic edemas [4]. Clinical symptoms of occupational leg edema resemble those of chronic venous insufficiency (CVI), particularly lower limb edema and pain. It was evaluated in this RCT whether the use of conservative medical compression stockings for the treatment of occupational orthostatic edema is as beneficial as it has been proven to be in the treatment of symptomatic edema associated with CVI [5, 6].
A study in the Danish population showed an increased risk of being hospitalized due to varicose veins when having to stand at work for long times [7]. In addition, complications such as erysipelas are associated with varicose veins and can cause downtime from work and the need for hospitalizations [8].
This prospective, randomized study aims to substantiate the relevance and efficacy of compression hosiery to prevent occupational orthostatic edema and to assess the effects on leg discomforts, leg volume, and wearing comfort in two medical below-knee compression stocking types with an interface pressure of 18 –20 mmHg and a below-knee-low-pressure support stocking (LPSS) with an interface pressure of 8–10mmHg.
Methods
Study design
Forty-nine healthy volunteers were included in this randomized, blinded, crossover study. After being screened for their suitability, the eligible participants were divided into two cohorts. Both groups had to wear three pairs of below-knee stockings. Each type of stocking was worn for three consecutive days in one week, followed by a subsequent washout phase without wearing any stockings for four days. Thus, the test period for each participant was three weeks. The cohorts were named after the respective sequence of the wearing period (Table 1).
The first group started with compression stocking type A and then continued with compression stocking type B the next week; the second group wore both compression stockings in a reversed order; both groups wore a placebo stocking with no compression properties (type C) during the last week of the trial
The first group started with compression stocking type A and then continued with compression stocking type B the next week; the second group wore both compression stockings in a reversed order; both groups wore a placebo stocking with no compression properties (type C) during the last week of the trial
The primary outcomes were to assess volume changes achieved by the two below-knee medical compression stockings and a LPSS and their effects on the leg discomforts associated with occupational edema. The secondary outcome was the evaluation of the wearing comfort of the stockings.
This study was conducted at the Department of Dermatology of the Universitymedicine Greifswald and an approval of the local ethics committee was given (internal registration number: BB 087/18a), according to the principles of the Declaration of Helsinki.
All eligible participants were healthy adults between the ages of 19 and 63 who were suffering from occupational leg discomforts and occupational orthostatic leg edemas in the evening. Those discomforts included feelings of heaviness, tension, tingling, tiredness and pain. If there were only leg edemas without any leg discomforts reported, volunteers were excluded. Study participants were only included in the study if no additional symptomatic venous disorder could be determined, and they were classified as C0 - C1 according to the CEAP classification [9].
Compression materials
Two different types of below-knee elastic medical compression stockings (stocking A and B) [10] and one below-knee-low-pressure support stocking (=LPSS = stocking C) were used regarding their effects on orthostatic edemas and leg discomforts. Both compression stockings were RAL tested (Reichs-Ausschuss für Lieferbedingungen, Sankt Augustin, Germany) [11] and approved medical devices (CE) with an interface pressure of 18 –21 mmHg at the ankle with a declining pressure from distal to proximal [12]. Stocking type B differs slightly from stocking type A in offering a modified heel and instep area that could increase comfort by reducing constriction and wrinkling. The LPSS (stocking C) had an interface pressure of 8–10 mmHg, measured by PicoPress® (Microlab Elettronica, Roncaglia di Ponte San Nicolò (PD) Italy) [13].
Measurements and questionnaires
Volume of the lower leg
Volume measurements of the lower leg, from level B to level D, were determined with the Bodytronic®600 (Bauerfeind AG, Zeulenroda, Germany) via three-dimensional imaging. The system consists of a rotating plate, a scanning system and a control unit [10]. The study participants were positioned according to marked spots on a rotation platform and instructed to hold onto a frame with both hands. When the platform starts rotation counter-clockwise it turns 360° for less than a minute while pictures are taken at specific points of the rotation forming a point cloud, out of which a three-dimensional image of the lower body is constructed and volumes, lengths and circumferences are calculated [14]. We focused on the volume measurements of the lower leg in our study.
Measurement of interface pressure
The interface pressure of the LPSS was measured by PicoPress® (Microlab Elettronica, Roncaglia di Ponte San Nicolò (PD) Italy) [13]. The measurement was done in a standing position while placing a silicone sensor cushion on the lateral lower leg proximal to the Malleolus lateralis (at the level of B1) between the stocking and skin. The values were given in mmHg [15].
Assessment of clinical symptoms, side effects and wearing comfort
Participants had to fill in different questionnaires to assess clinical discomforts, side effects and wearing comfort.
I. Questionnaire about wearing comfort
Study participants had to fill out a questionnaire to evaluate the wearing comfort and side effects of the respective stocking for each day of every wearing period (completed in the evening). This questionnaire consisted of 61 items. In the first part there were 48 items about leg-complaints such as constriction, tightness, formation of wrinkles, pain, heat/cold sensations, burning, tingling, numbness and itching. Followed by 6 items regarding skin changes such as dry skin, redness, skin colorations, small wounds and blisters. The last part (7 items) concentrated on questions about wearing-comfort such as the general fit and required time and effort needed to put on the stockings. The answer to each question was given on a visual analog scale (VAS), which was 10 cm long (0 = no complaint/excellent fit; 10 = very strong complaint/poor fit).
II. Questionnaire about quality of life
This questionnaire also consisted of 61 items and was based on the “Tübinger Life Quality Questionnaire” by Klyscz et al. [16] and had to be completed during the screening visit to evaluate discomforts connected to occupational orthostatic leg edemas. Participants were only included if symptoms were present.
The same questionnaire had to be filled at the end of every wearing period and concentrated on the effects of the stockings on occupational orthostatic leg discomforts described previously. It was handed in with the three daily questionnaires at the end of every week.
The questionnaire was divided into 4 different parts, starting with 24 items about general leg discomforts/complaints connected to occupational orthostatic leg edemas such as tension of the lower legs, heavy legs, feeling of tiredness in the lower legs, tingling, leg pain and numbness of the lower legs before/after compression therapy. Study participants had 6 different response options (0 = complaint not present to 5 = complaint present, very severe).
The second part was concerned with the functional status (restrictions during everyday life) due to occupational orthostatic leg edemas before/after compression therapy. The 16 items included long sitting, walking, long standing, sleeping problems, housework, putting on shoes and climbing stairs. Answers could be given on a VAS of 10 cm (0 = complaint does not affect me at all; 10 = complaint affects me very severely).
In the third part, study participants were asked about general quality of life regarding leg complaints before/after compression therapy. Those 16 items included general well-being, satisfaction with daily life, anxiousness, exhaustion due to leg complaints and stress.
Additionally, 5 items were included to assess treatments, satisfaction with treatment and consequences before/after compression therapy. The last two parts of this questionnaire were also answered on a VAS of 10 cm (very satisfied/not affected very much; 10 = very dissatisfied/severely affected).
All 61 items were then assembled into six Life Quality Dimensions (LQD), in accordance to the “Tübinger Life Quality Questionnaire” by Klyscz et al. (Table 2) [16].
LQD and the included items for each dimension
LQD and the included items for each dimension
This RCT was conducted between July and December 2018. There was a total of 7 visits: one screening visit and two visits each week during the wearing period (3 weeks) (Fig. 1). All visits and volume measurements of the legs were according to the working schedule of the individual study participant. When working during daytime, they were done between 6:30–8:30 a.m. (screening visit) and 4:00–6:00 p.m. (all other visits) after work. When working during nighttime, measurements were taken before work between 9:00–10:00 p.m. (screening visit) and 6:30–7:00 a.m. (all other visits) after work.
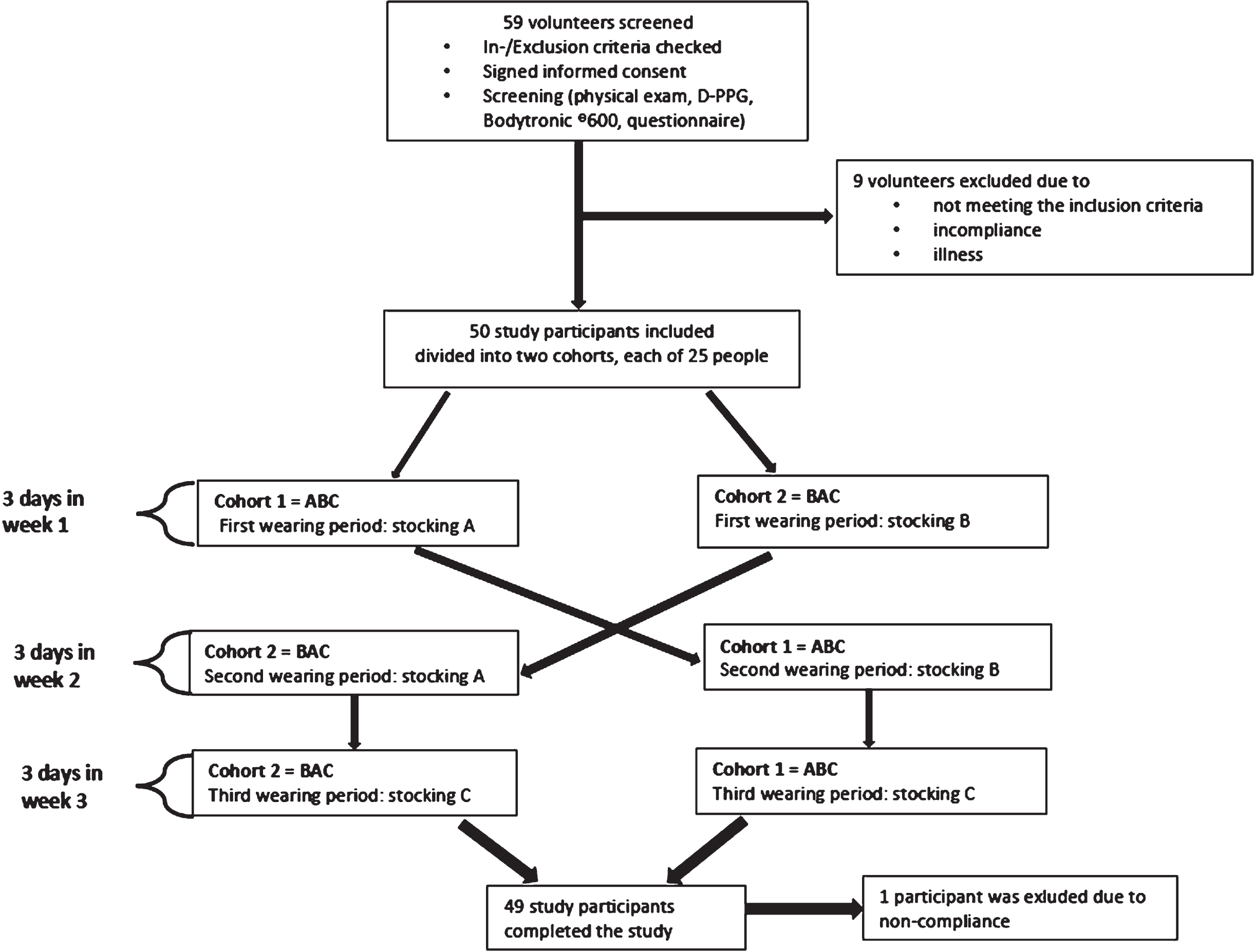
Consort diagram.
Screened participants were divided into two cohorts. Each cohort had a randomized sequence for all three stockings (ABC or BAC = Stocking A/B = medical compression stocking, interface pressure 18–21 mmHg and stocking C = LPSS, interface pressure 8–10 mmHg). The cohorts were named after the respective sequence of the wearing period (ABC/BAC). Each type of stocking was worn for three consecutive days in one week. There was a four-day break between each stocking to ensure that effects of the previous stocking did not influence the wearing period of the next stocking (wash-out phase) (Fig. 1).
All participants were evaluated in a screening visit. The visit was divided into two parts to measure volume changes of the lower leg (Bodytronic®600, Zeulenroda, Germany) before work and after an eight-hour day at work. Volunteers were also checked for inclusion and exclusion criteria and physically examined by a dermatologist. Before being included, the venous function was tested via DPP-G (Vasoquant® 1000 D-PPG, ELCAT GmbH, Wolfratshausen, Germany) [17–19]. Subjects with a venous refilling time <25 s and venous drainage <2.5 % were excluded (Table 3).
Inclusion and exclusion criteria
Visit 1, 3 and 5 were done after work on the day before the respected wearing period. During these visits, volume measurements of the lower legs were done via Bodytronic®600 (Bauerfeind AG, Zeulenroda, Germany) and a new pair of stockings to wear for the upcoming three days was handed out (Fig. 2).
Visit 2, 4 and 6 were also done after work, on the last day of each wearing period and included volume measurements of the lower legs wearing the stockings and the collection of the questionnaires (Fig. 2). Pictures were taken at each visit to document any side effects of wearing the stockings and other changes to the leg.
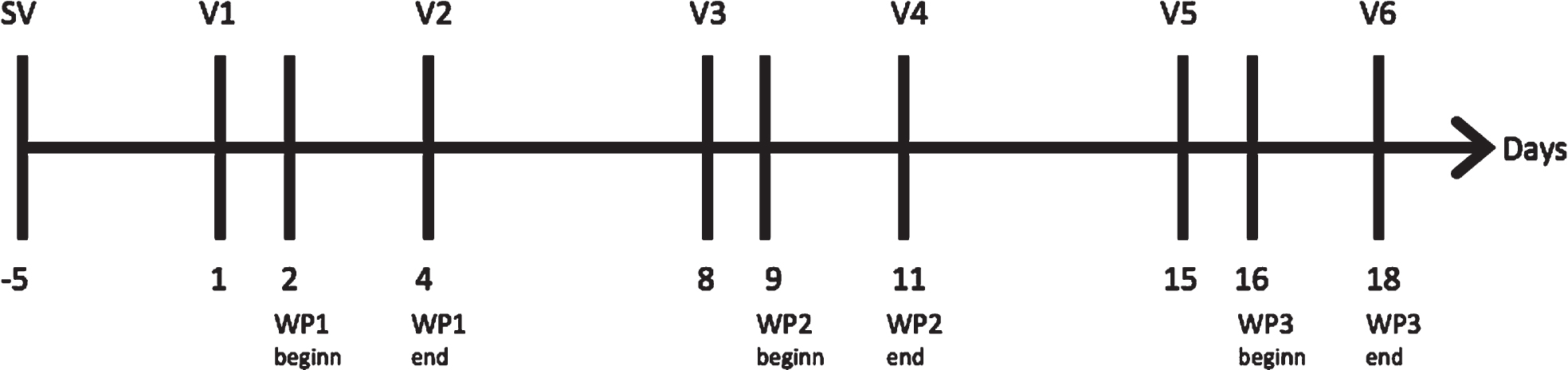
Timeline of the study visits showing the days of the visits and wearing periods. Between V2/V3 and V4/V5 were 4 days break (wash-out phase) SV = screening visit; V = visit; WP = wearing period.
The number of study participants needed was calculated based on the data from studies by Blazek et al. [1] and Blättler et al. [21]. A cohort size of n = 44 was calculated by a power analysis for an alpha value (significance level) of 5 % and a power of 80 %. The statistical analysis was done with the statistical analysis system and some R-packages. For example, randomization was done by the R-package blockrand [22].
Volume values were expressed in absolute volumes in liters (L) and milliliters (mL). Mean and median as well as standard deviations were calculated for all volume changes and shown via scatter-plots. The t-test was used to show significant changes in leg volume and the paired t-test was used to show significant changes in LQ-dimensions and wearing comfort due to the stockings. Questionnaires were analyzed and depicted with box-plots (Fig. 3) showing the median, upper quartile, lower quartile, lower whisker and upper whisker. A significance level of 5% was defined as being statistically significant for all tests.

Schematic drawing of a boxplot ©Herrmann Haase.
Participants and demographics
Fifty-nine volunteers were screened for this study. Fifty venous-healthy participants could be included after screening and nine volunteers had to be excluded due to various reasons, such as incompliance or illness.
Forty-nine participants finished the study, and one participant was excluded during the last week because of incompliance. The majority was made up by women (43 females vs. 6 males) and all were based in the city of Greifswald and its suburbs (Fig. 4).
Most participants (n = 34) were working in the medical sector, which included nurses, physicians, medical students and medical assistants. Fourteen were working mostly at desk jobs, such as secretaries, postdocs, engineers and administrative workers and one was a social worker with 50 % desk-work and 50 % field work (Fig. 5).
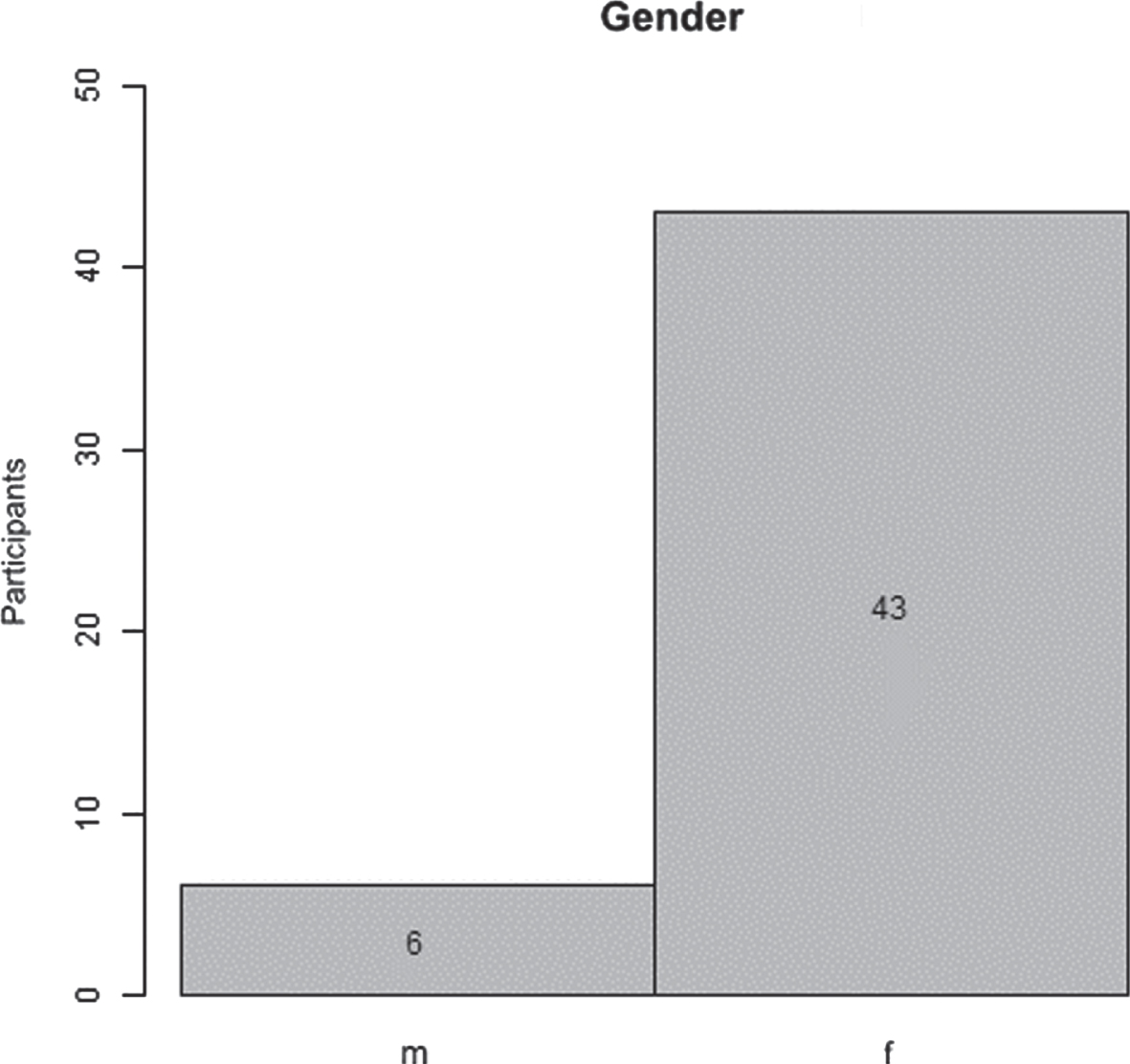
Gender distribution of all 49 study participants (m = male, f = female). Forty-three were female and six were male participants.
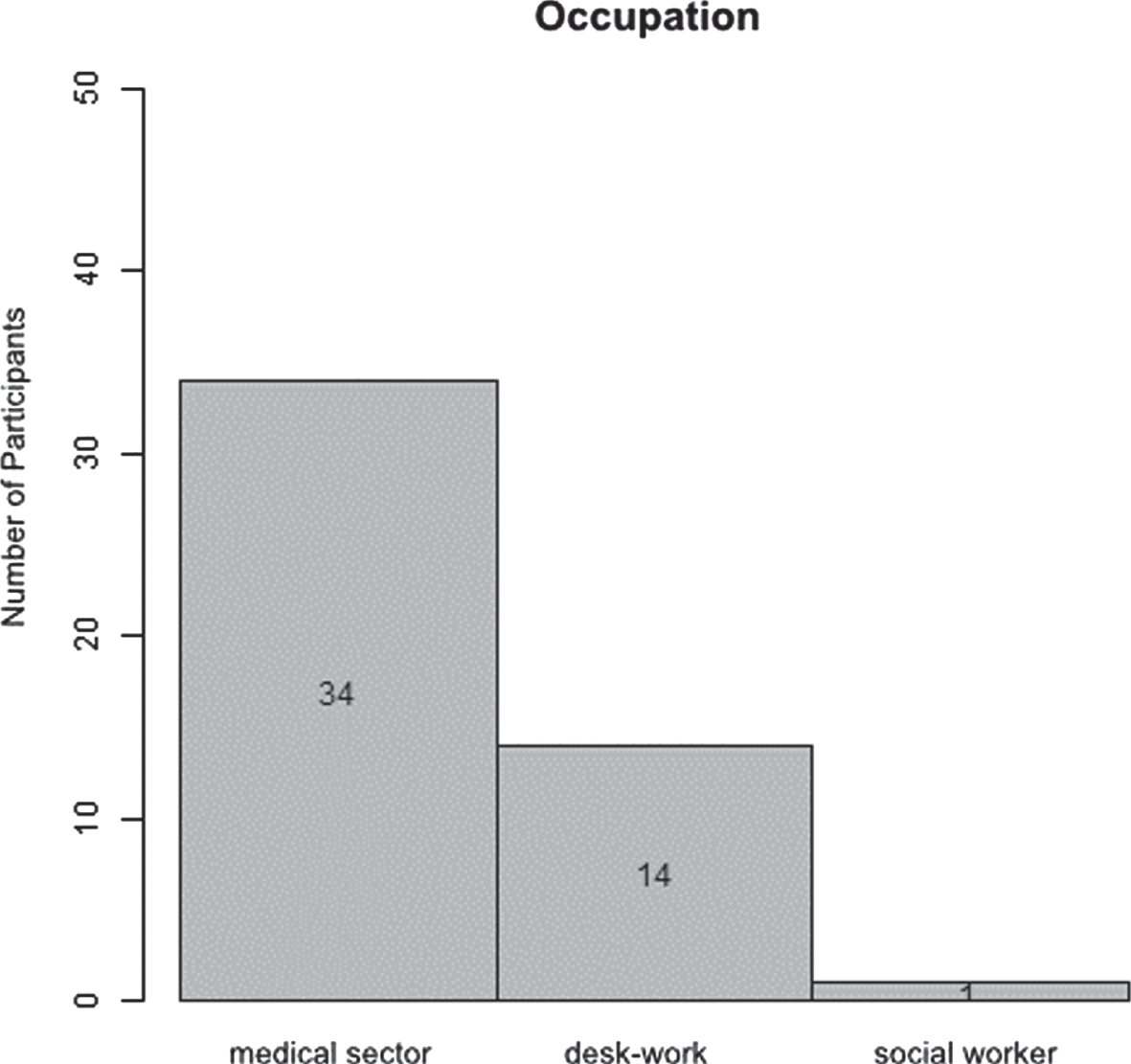
Thirty-four participants were working in the medical sector. One was working as a social worker and the other 14 were doing desk work
Changes in the lower leg volumes before and after each respective wearing period showed a significant reduction while wearing both types of below-knee compression stockings (p < 0.001) as well as the LPSS (p < 0.001). The mean volume reduction in stocking A was 205 ml (≜7.63 %) and 153 ml (≜5.77 %) in stocking B. The volume reduction in the LPSS was 48.2 ml (≜1.5 %), showing a significant reduction in all stockings but also between stocking type A and B (p = 0.001) (Fig. 6, Table 4).
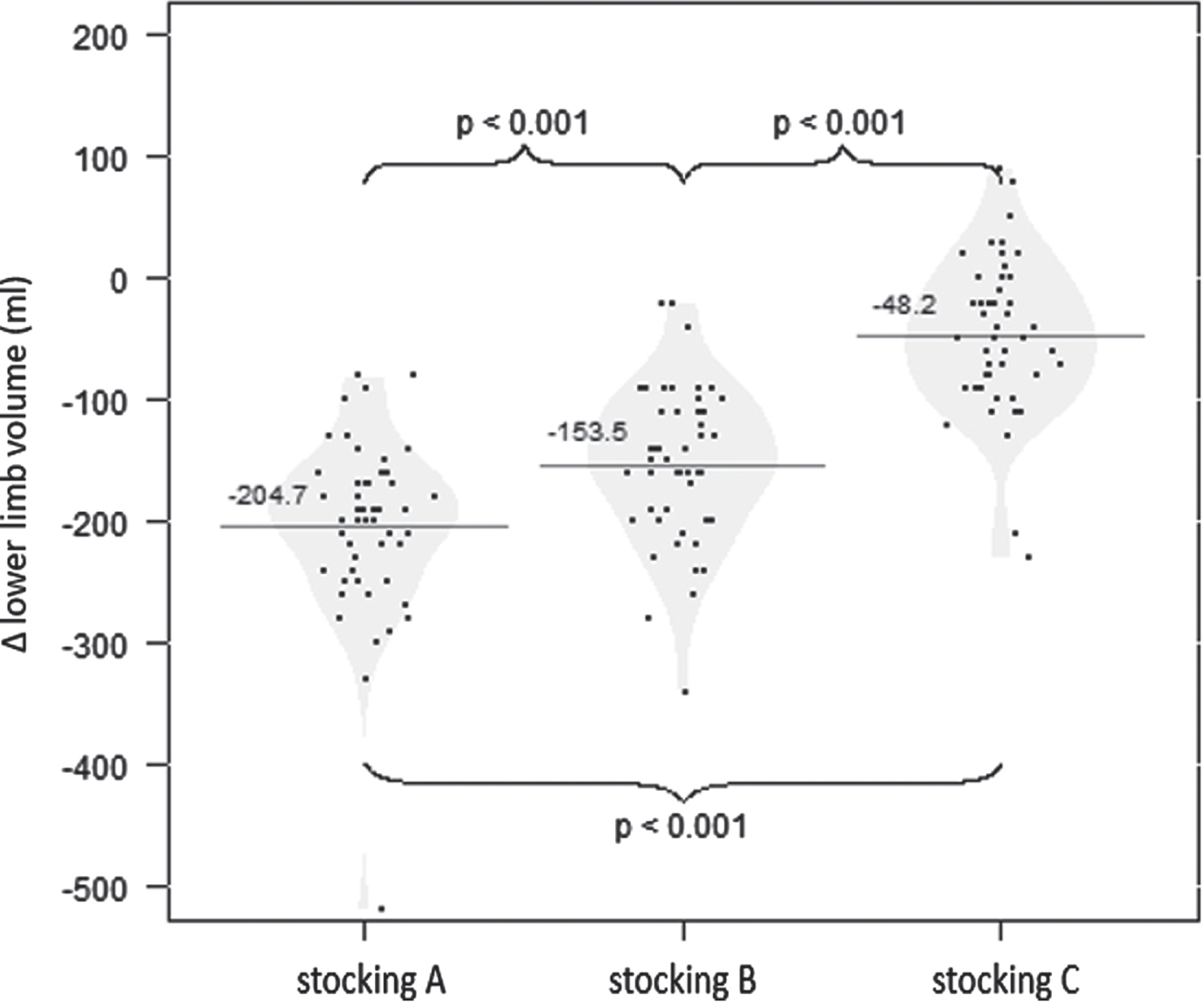
Volume changes in the lower leg in all three stockings. The mean volume reduction in stocking A was –205 ml and –153 ml in stocking B. The volume reduction in stocking C was –48.2 ml. A/B = below-knee medical compression stockings, C = LPSS
Averages, quartiles and standard deviation regarding the volume reduction in the lower leg in all three stockings in ml
Study participants were asked during the screening visit about complaints associated with orthostatic leg edemas due to occupational load and given a questionnaire to indicate whether the complaint is present and, if it is present, rate it on an NRS from 1 –5 according to its severity. Those complaints included, for example, the feeling of tension, tingling, pain and heaviness. The participants had to fill in a daily questionnaire during the wearing period rating each complaint on the same NRS while wearing each pair of stocking. These complaints were then assembled as the LQD “leg complaints” (Table 2).
Significant improvement (p < 0.0001) was seen for all three types of stockings at the end of the trial compared to the initial values (Fig. 7).
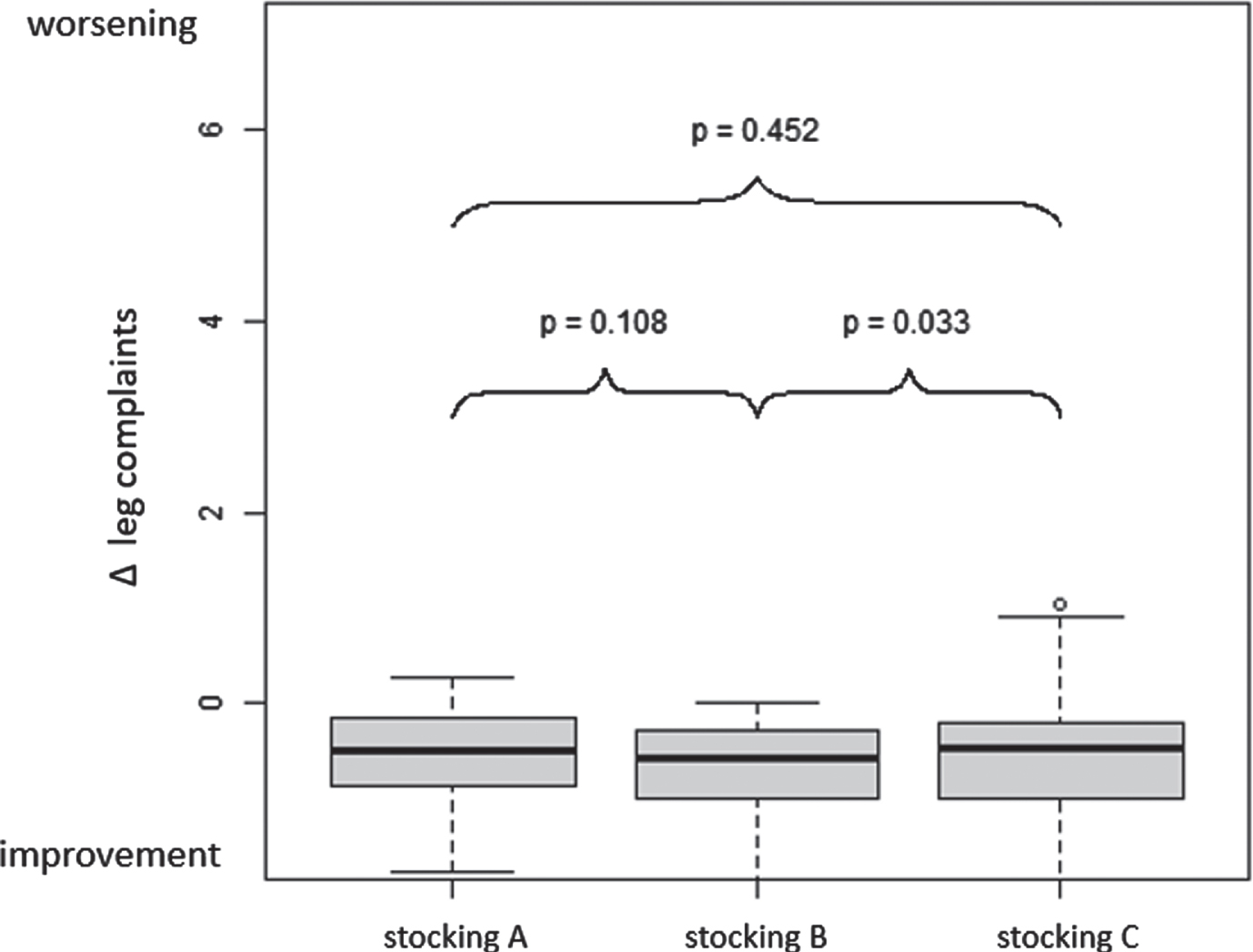
Delta of changes in the LQD “leg discomfort” shows significant improvement for all three stockings (p < 0.0001). The delta was determined by comparing the mean of all responses belonging to the LQD “leg discomfort” after wearing each stocking with the mean of the baseline leg discomfort scores (mean end of 3-day wearing period for each stocking- mean of baseline discomfort). Responses were given on an NRS of 1–5 according to the severity of discomfort. When comparing the different stockings, there is a significant (p = 0.033) difference between the compression stocking B and the LPSS. Stocking A/B = medical lower leg compression stocking with a contact pressure of 18–20 mmHg, Stocking C = LPSS with a contact pressure of 8–10 mmHg.
Regarding the LQD “functional status” (Table 2), a significant improvement in all three types of stockings (stocking A+B p < 0.0001; stocking C (LPSS) p = 0.0023) for complaints such as impairment of long walking/sitting/ standing but also putting on shoes and housework was seen (Fig. 8). There was no significant difference between all 3 types of stockings.
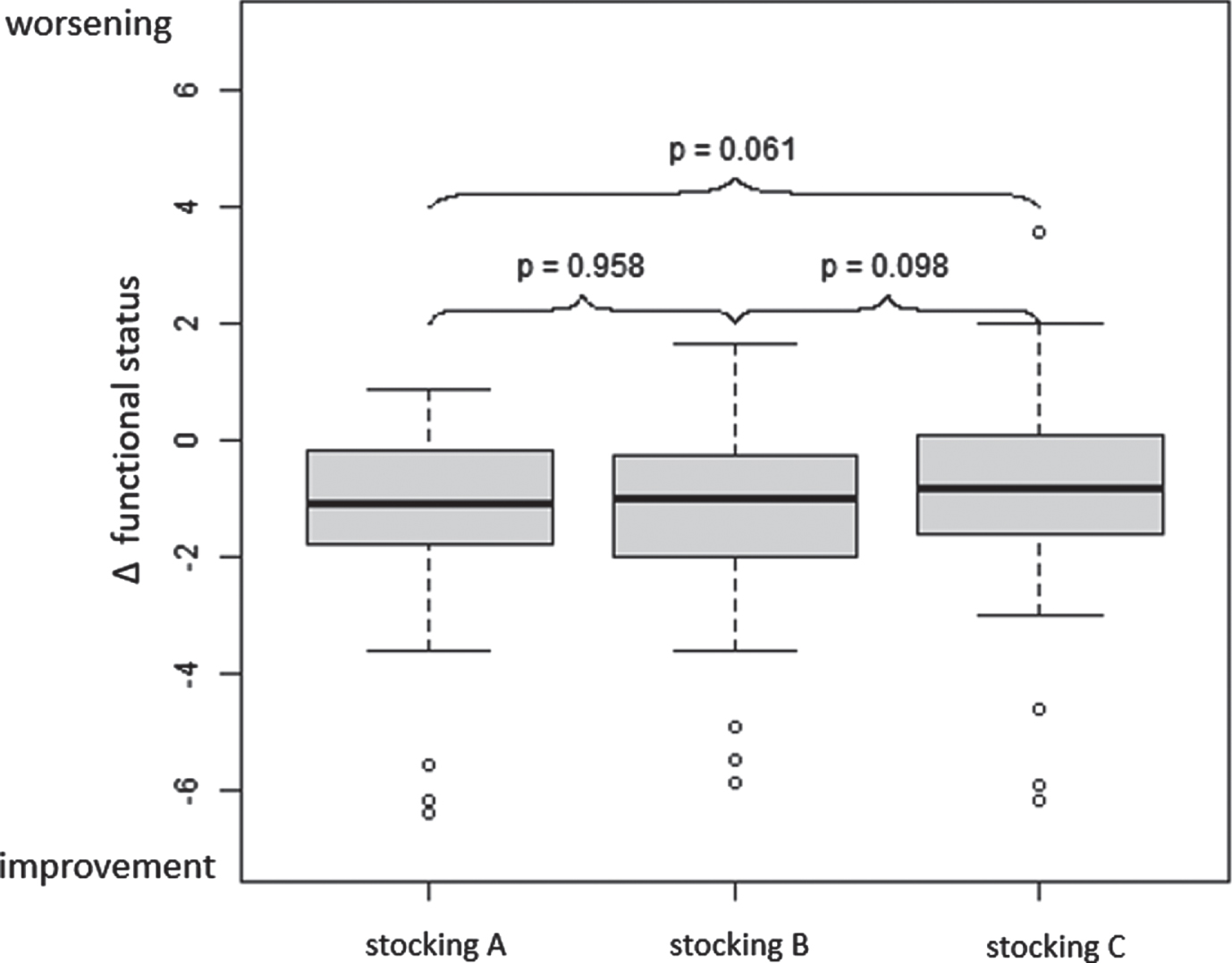
Delta of changes in “functional status” related to restrictions in daily life due to occupational orthostatic leg edema before/after compression therapy shows significant improvement for all three stockings (Stocking A and B p < 0.0001; Stocking C p = 0,00023). Answers to questions about functional status (16 items included) could be reported on a VAS of 10 cm (0 = discomfort does not affect me at all; 10 = discomfort affects me very severely). The delta was determined by comparing the mean of all responses after wearing each stocking with the mean of the baseline leg discomfort scores (mean end of 3-day wearing period for each stocking - mean of baseline discomfort). When comparing the different stockings, there is no significant (p = 0.061) difference between the compression stockings A and B and the LPSS. Stocking A/B = medical lower leg compression stocking with a contact pressure of 18–20 mmHg, Stocking C = LPSS with a contact pressure of 8–10 mmHg.
A VAS was used to assess the wearing comfort in all three types of stockings. Regarding the general fit of both below-knee compression stockings, no significant difference was seen but both were significantly better fitting than the LPSS (Fig. 9).
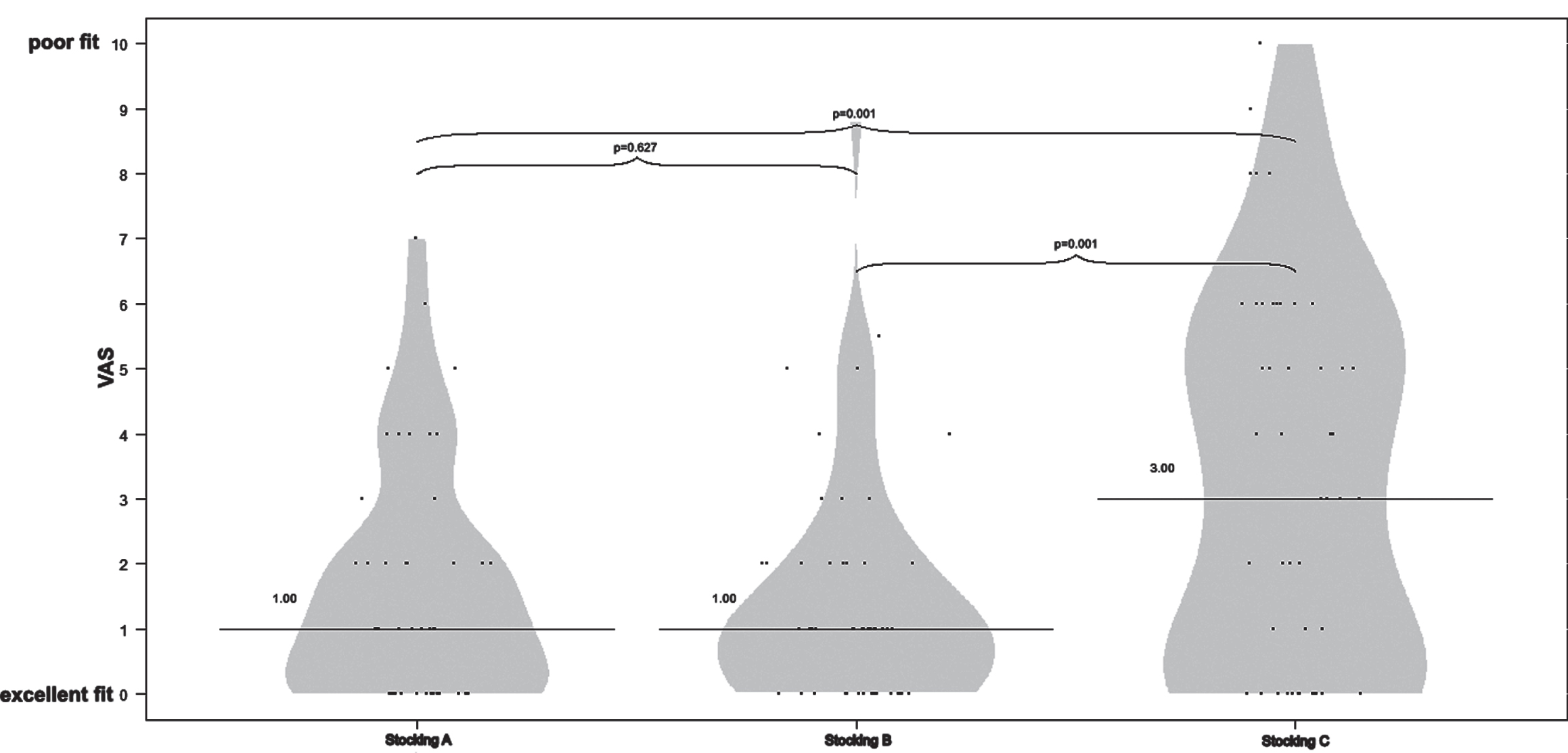
The median of the general fit of all three types of stockings on a VAS. There was no significant difference between the different compression stockings (p = 0.627). Both compression stockings have a highly significantly (p = 0.001) better fit than the LPSS. A/B = below-knee medical compression stockings, C = LPSS 0 = excellent fit, 10 = poor fit.
Stocking type B has a modified heel and instep area intended to increase wearing comfort, but both below-knee compression stockings performed equally well in terms of tightness, constriction and feelings of pain in the bond, instep and heel area and no significant difference could be established (p > 0.05). However, Study participants preferred wearing the compression stockings rather than the LPSS (p < 0.003), especially due to the slipping off the stocking and formation of wrinkles especially in the toe area. There was no significant difference between the two compression stockings (p = 0.934).
People frequently develop leg discomforts often accompanied by edemas of the lower legs when they have sedentary occupations or are standing for a long time during their work. The development of these occupational orthostatic edemas is not necessarily based on primary vascular or lymphatic vessel changes, as it is in the typical edemas caused by CVI or due to lymphedema. Increased hydrostatic pressure on the intracapillary wall due to sitting or standing positions causes an increased ultrafiltration into the interstitial space in orthostatic edemas. The excessive fluid cannot be removed sufficiently via the lymphatic system and cannot be reabsorbed into the venous system at the same rate as it is produced [1–4, 23]. Although orthostatic edemas and the accompanying leg discomforts are reversible after elevation of the legs or changing position, it remains questionable whether the repeated stress on the intracapillary walls could trigger a cascade of inflammatory responses in the tissue, as seen in progressive CVI. Maybe it is possible that long-term occupational orthostatic edema that is not treated could cause nonreversible mechanical damage to the capillary walls and result in tissue hypoxia. This, in turn, would lead to the release of proinflammatory cytokines, such as IL-1 and TNF-alfa, by activated mast cells and neutrophils and a further increase in the permeability of the vessel wall through leukotriene stimulation [24]. The possibility of developing chronic edemas and leg discomforts due to occupational standing and sedentary activities shows the need for a targeted therapy.
Compression therapy in combination with manual physical therapy constitute the main principles in the conservative treatment of edemas due to venous and lymphatic pathologies. Compression stockings, bandages and other compression systems reduce swelling, discomforts and secondary changes in the tissue, and complications, such as ulcerations, increased affinity to infections of the tissue (e.g. erysipelas) [5, 26]. The aim of this RCT was to ascertain, whether low pressure below-knee compression stockings (18–21 mmHg) and a LPPS (8–10 mmHg) are also suitable achieving effective changes in lower leg volumes and edema-associated leg discomfort that are due to long standing and sitting activities at work. The wearing comfort of the three stockings and changes in quality of life were evaluated as a secondary outcome.
A significant volume reduction (p < 0.001) in the lower legs, after a short wearing period of 3 days, in all stockings (stocking A = 205 ml, stocking B = 153 ml, C = 48,2 ml) was seen.
People suffering from occupational orthostatic edemas often complain about discomforts in the lower legs, such as tiredness, leg pain, feelings of tension and tingling, which improved significantly by wearing low-pressure below-knee compression stockings and LPSS. Especially for the leg complaint “leg-swelling” a significant reduction could be established comparing the low-pressure below-knee compression stockings and the LPSS. While a reduction in volume, feeling of heaviness with the resulting feeling of tension can be readily explained by improving the ultrafiltration of excess fluid in the interstitial tissue, the only direct correlation in this study could be made between volume changes and the improvement of tension in the legs. Other discomforts were also getting better but no direct correlation could be made to changes in the lower leg volume. Pathophysiological backgrounds, such as neurological changes, have been proposed in other studies to explain this phenomenon [1, 21]. It is possible that edema of the lower legs influences the nervous function by compressing nerves and the nervous system is regenerating at its own rate when using compression therapy. Another possibility is the release of trigger substances due to increased capillary wall permeability into the tissue that can cause changes in the nervous system, especially the sensory function, which is also improving under compression therapy.
The results of this study, when looking at the reduction in lower leg volume and leg discomforts associated with orthostatic edema, show that below-knee compression stockings with a low interface pressure of 18 –21 mmHg as well as LPSS with an interface pressure of 8–10 mmHg can have a significant effect on the reduction of orthostatic edemas and symptoms associated with them. In a study by Blazek et al. [1] a cohort of hairdressers was investigated regarding edemas and leg discomforts associated with long-time standing while working. The authors found that wearing low-pressure compression stockings with an ankle pressure of 15 –20 mmHg could reduce discomforts and leg volume considerably. Compared to the present study, the hairdressers participating wore stockings for three weeks, while in the present study, each stocking was worn only for three days, demonstrating that a short wearing period can already have a significant effect on occupational edemas and discomforts of the lower legs.
Other studies have also shown that there is no evidence that compression stockings with a higher interface pressure also intensify the improvement of symptoms [27, 28].
Nevertheless, patients are often prescribed compression stockings with an interface pressure of >21 mmHg rather than with lower compression properties, which may be due to existing dogmatic propositions as to which compression class should be prescribed for a specific diagnosis [29]. Medical compression hosiery should be prescribed according to symptoms and not only diagnosis [25].
In addition to the type of hosiery, it is important to consider the interface pressure of the compression material regarding donning and the individual physical conditions of the patient since those factors influence and reduce the compliance. It is a lot easier and takes less time to don knee-length compression stockings with an interface pressure of 18 –21 mmHg than it does compression stockings with an interface pressure of 23 –32 mmHg, as was shown by another study at the Department of Dermatology at the Universitymedicine Greifswald. Not only was it significantly (p = 0.004) easier and took less time to don the stockings, but the wearing comfort of the hosiery with lower compression properties was also significantly better (p = 0.045), particularly in patients with additional physical limitations [30, 31].
Although Stocking type B has a modified heel and instep area intended to increase wearing comfort, both below-knee compression stockings performed equally well in terms of tightness, constriction and feelings of pain, which is an indication of the high qualitative standards in conventional compression stockings.
In this RCT both custom-fit compression stockings showed a significant better fit than the standard-fit LPSS. According to study participants, the LPSS started slipping and formed wrinkles during the wearing day, which was perceived as being “annoying”. When ascertaining the wearing comfort of stockings, a big part plays the fit of the stocking. The easier donning and greater wearing comfort can be a huge advantage in increasing patients’ compliance and adherence to compression therapy.
Limitations
All participants in this study were recruited on a voluntary basis and might have known before the start of the study about possible positive effects of compression therapy on occupational leg edema and associated discomforts, which could have caused an involuntary bias towards the compression stockings.
The summer of 2018 was very hot in Germany, which made it a difficult time for wearing compression stockings for the study participants. The temperature in the area of Greifswald, Germany, in the summer months of July to October went up to 36.4°C [32], causing increased sweating and heat buildup under the stockings. This could have resulted in less wearing comfort but possibly also a general increase in edema formation and leg discomforts due to the increased permeability of the capillary walls.
The 3D-imaging system (Bodytronic®600, Bauerfeind AG, Zeulenroda, Germany), which was used to measure the lower leg volume, is susceptible to factors such as the lighting of the room while measurements are taken. We tried to keep this factor to a minimum by always having the blinds of the room closed during the use. Another aspect that had to be considered is the avoidance of dark, loose or reflecting (e.g.silk/satin) underwear as well as any movement by the study participants during measurements. Before any measurements were taken with the Bodytronic®600 (Bauerfeind AG, Zeulenroda, Germany), these factors were explained in detail to each study participant to decrease any measurement errors.
In both groups, the two below-knee compression stockings type A and B, which the participants of the study could not distinguish from one another, were worn in the first two weeks and the LPSS during the third week. The appearance of the LPSS stocking with an interface pressure of 8–10 mmHg was different to the compression stockings (18–21 mmHg). The optical and haptic distinguishability could have influenced the participants’ assessment.
Another external factor, that we cannot know about and control, is the possibility that the study participants’ individual living circumstances and the orthostatic loads were not identical during each wearing period.
Conclusion
Below-knee medical compression stockings with an interface pressure 18–21mmHg and LPSS with an interface pressure of 8–10 mmHg significantly reduce occupational orthostatic edema (stocking A: 204.7 ml; mean stocking B: 153.5 ml; mean stocking C: 48.2 ml) and leg discomforts which are due to long standing and sitting activities. Especially a significant reduction of the life-quality dimension leg-complaints (p < 0.0001) was achieved. Because of the custom fit, medical below-knee compression stockings are having a significant better wearing comfort than commercial LPSS (p < 0.006) and should be preferred when prescribing compression stockings to prevent occupational edema.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
The compression material for the study was provided by Bauerfeind AG, Zeulenroda.
Sophie Hecko received the Doctoral Prize 2020 by the German Phlebology Association sponsored by Bauerfeind AG, Zeulenroda.
Ethics approval
This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the Ethics Committee of the University of Greifswald (internal registration number: BB 087/18a).