
Abstract
OBJECTIVE:
To evaluate the value of contrast-enhanced ultrasound (CEUS) characteristics based on primary lesion combined with lymphatic contrast-enhanced ultrasound (LCEUS) patterns of SLN in predicting axillary lymph node metastasis (ALNM) with T1-2N0 breast cancer.
METHODS:
A retrospective study was conducted in 118 patients with clinically confirmed T1-2N0 breast cancer. Conventional ultrasound (CUS) and CEUS characteristics of the primary lesion and enhancement patterns of SLN were recorded. The risk factors associated with ALNM were selected by univariate and binary logistic regression analysis, and the receiver operating characteristic (ROC) curve was drawn for the evaluation of predictive ALNM metastasis performance.
RESULTS:
Univariate analysis showed that age, HER-2 status, tumor size, nutrient vessels, extended range of enhancement lesion, and the enhancement patterns of SLN were significant predictive features of ALNM. Further binary logistic regression analysis indicated that the extended range of enhancement lesion (p < 0.001) and the enhancement patterns of SLN (p < 0.001) were independent risk factors for ALNM. ROC analysis showed that the AUC of the combination of these two indicators for predicting ALNM was 0.931 (95% CI: 0.887–0.976, sensitivity: 75.0%, specificity: 99.8%).
CONCLUSION:
The CEUS characteristics of primary lesion combined with enhancement patterns of SLN are highly valuable in predicting ALNM and can guide clinical axillary surgery decision-making in early breast cancer.
Introduction
According to the latest data, the incidence of breast cancer has ranked first among female malignant tumors worldwide [1]. The pathological status of axillary lymph node (ALN) is critical to the treatment and prognosis of breast cancer patients [2]. Sentinel lymph node biopsy (SLNB), which is less invasive, has become the gold standard for staging ALN-negative patients with breast cancer [3]. This allows some patients to be protected from complications such as lymphedema, sensory paralysis, and motor limitation caused by axillary lymph node dissection (ALND) [4]. However, there are still some urgent problems to be solved in SLNB: such as radiation hazards and high false negatives [5, 6]. Therefore, there is a clinical need for a noninvasive and accurate preoperative imaging method to predict ALNM.
The studie to predict lymph node metastasis based on conventional ultrasound (CUS) features of the primary tumor have been validated in thyroid cancer [7]. The morphological characteristics of the primary lesion with breast cancer are closely related to its biological behavior [8]. Studies have confirmed that patients are more likely to have ALNM when the primary lesion has features such as microcalcification, hyperechoic halo, posterior acoustic decrease, burrs on the edge of the lesion, and distortion of the tissue structure [9, 10]. In addition, elastography has also shown good predictive efficacy in lymph node metastasis [11], it has been demonstrated that intratumoral stiffness is associated with lymph node metastasis in patients with breast and thyroid cancer [12, 13]. Although there have been many studies on assessing benign and malignant breast lesions by transvenous contrast-enhanced ultrasound (CEUS) at the level of blood flow information [14–16], the association between CEUS characteristics of the primary lesion and ALNM is still in the exploratory stage.
CUS is recommended as the imaging modality of choice for ALN, However, its diagnostic sensitivity and specificity are not satisfactory, and CUS cannot accurately identify sentinel lymph node (SLN) [17]. A meta-analysis has been reported that radionuclide has a high SLN identification rate (94%) [18]. However, we have to realize that unavoidable disadvantages including radiation hazards and expensive cost [19]. PET/CT was also commonly used to assist SLNB, but its sensitivity and specificity are lower than SLNB [20]. Lymphatic contrast-enhanced ultrasound (LCEUS) is relatively economical, simple, and noninvasive. It has been demonstrated that the success rate of LCEUS in localizing SLN can reach 70% –100% [21]. In addition, it also has great potential for qualitative diagnosis [22]. The current study is mainly to determine whether there was ALNM by observing the enhancement pattern of SLN. The study results confirmed that homogeneous enhancement (type I) and non-enhancement (type III) had high negative predictive value and positive predictive value, respectively [22, 23]. However, benign and malignant SLN overlapped greatly in heterogeneous enhancement (type II), resulting in overall reduced diagnostic specificity [22, 24]. This study made a more meticulous classification of SLN enhancement patterns based on previous studies.
In view of this, The aim of this study was to evaluate the prediction of ALNM in early breast cancer based on the CEUS characteristics of the primary lesion combined with enhancement patterns of SLN to assist surgical decision-making in the axilla.
Materials and methods
Patients
143 patients with breast cancer confirmed by core needle biopsy and negative ALNs on clinical palpation from January 2022 to June 2023 in the Second Hospital of Lanzhou University were prospectively collected. These patients underwent CUS and CEUS of the primary lesion and SLN 1 or 2 days before surgery, and pathological findings were obtained after surgery. The exclusion criteria were as follows: (a) tumor diameter > 5 cm; (b) incomplete preoperative imaging data; (c) patients without axillary surgery plan. 118 eligible patients were finally included in this study for retrospective analysis. Pathologic results of ALN were obtained by SLNB or ALND. Among them, 68 patients were classified as a metastatic group, while 50 patients were classified as a non-metastatic group. The study was approved by the Ethics Committee of the Second Hospital of Lanzhou University and all participants had signed a written informed consent (The approval number of the Ethics Committee: 2022A-217).
CUS and CEUS acquisition of primary tumor
In this study, Siemens (L9-3) and Philips (L12-5) ultrasonic instruments were used for examination respectively, and a low mechanical index was applied in contrast mode to reduce contrast agent destruction.
Patients were placed in the supine position with arms abducted to fully expose the breast and axilla for CUS and CEUS examinations. The location, size, shape, margin, echogenicity, calcification, and Adler flow grade of the lesion were recorded. The richest vessels of the lesion and the appropriate amount of surrounding normal tissues were selected for CEUS. Patients were instructed to breathe calmly during the whole process, and 6.0 ml SonoVue (Bracco, Milan, Italy) was quickly injected through peripheral veins, followed by 5 ml of normal saline (0.9%). Dynamic images were stored synchronously for 3 min for subsequent analysis. Evaluated qualitative characteristics included the following items: (a) enhancement degree (hyperenhancement and iso-/hypo-enhancement); (b) enhancement boundary (clear/unclear); (c) internal homogeneity (homogeneous/heterogeneous); (d) perfusion mode (centripetal/non-centripetal); (e) penetrating vessels (presence/absence); (f) extended range (difference between the maximum diameter of the lesion measured in CEUS and that measured by CUS).
Lymphatic contrast-enhanced ultrasound examination
After disinfecting the areola area, 2.0 ml of contrast agent suspension (0.5 ml at each point) was injected intradermally at four points: 3, 6, 9, and 12 around the areola, and each injection point was gently massaged for 10–30 s. Switched on the contrast mode, when superficial lymphatics were detected on scanning around the areola, the probe started tracing the path of the lymphatics along the axillary direction until the first/group of visualized lymph nodes were SLNs. The enhancement patterns of SLN was recorded by dynamic scanning. Save images for subsequent re-analysis. It is worth noting that patients with breast cancer receiving the COVID-19 vaccine may develop axillary lymphadenopathy, which is usually characterized by diffuse cortical thickening on CUS [25]. Therefore, we did not consider diffuse cortical thickening as a suspicious lymph node sign.
All procedures were performed by a single sonographer with 5 years of experience in breast ultrasound. Image analysis was independently performed by two other senior physicians without knowledge of the clinical data, and agreement was reached through consultation in case of disagreement.
Surgical management of the ALN
All participants underwent axillary surgery. SLNB was mapped with blue dye and Indocyanine green (ICG). All marked SLNs were removed and sent for frozen paraffin pathological examination in the pathology department, and ALND was performed immediately if SLN positivity was confirmed by intraoperative pathology. Macro metastasis (tumor area > 2 mm) and micrometastasis (tumor area > 0.2 and≤2 mm) were defined as metastatic lymph nodes. The procedure was performed by two surgeons with extensive surgical experience.
Statistical analyses
SPSS 26.0 was used for statistical analysis. The continuous variables in this study did not conform to a normal distribution by the Kolmogorov-Smirnov test, so the Mann-Whitney U test was used for comparison between the two groups. The categorical variables were expressed as n (%), and the χ2 test or Fisher exact test was used for comparison between groups. The cutoff values for continuous variables were determined by plotting (receiver operating characteristic, ROC). Independent risk factors were further analyzed using binary logistic regression for indicators with statistically significant differences in univariate analysis, and P < 0.05 was considered statistically significant. ROC curves were plotted to evaluate the value of each parameter and combined index in predicting ALNM.
Results
Patient and tumor characteristics
Among the 118 patients, there were 50 (42.4%) had ALN negative, and 68 (57.6%) had ALN positive. Table 1 shows the clinical characteristics and preoperative pathological diagnosis of patients in the ALN-negative and ALN-positive groups. There were statistically significant differences in age (p = 0.032) and HER-2 status (p = 0.030) between the two groups, and patients aged≥50 years and HER-2 positive were more likely to have ALN metastases. No significant correlations were observed between the two groups regarding menopause (p = 0.108), ER status (p = 0.806), PR status (p = 0.304), Ki-67 level (p = 0.328), and molecular subtype (p = 0.157).
Patient and tumor characteristics between ALN negative group and positive group
Patient and tumor characteristics between ALN negative group and positive group
*Indicates significant values, P < 0.05; ALN, axillary lymph node; PR, progesterone receptor; ER, estrogen receptor; HER-2, Human epidermal growth factor receptor 2.
Among 118 patients, based on the pathological findings as the gold standard, there was a significant difference in tumor size between patients with and without ALNM (p < 0.05), while there was no correlation between location, shape, margin, echogenicity, microcalcification and Adler flow grade of the lesions and whether the ALN was metastasized (p > 0.05) (Table 2).
Correlation of CUS characteristics of primary lesion versus the final pathology results of ALN
Correlation of CUS characteristics of primary lesion versus the final pathology results of ALN
*Indicates significant values, P < 0.05.
In this study, the SLN enhancement patterns was divided into 4 types (5 subtypes): type I showed homogeneous and bright hyperenhancement (Fig. 1A, 1a); type II included type IIa which showed diffuse hypoenhancement (Fig. 1B, 1b) and type IIb which showed annular or semi-annular enhancement (Fig. 1C, 1c), SLNs that showed type II appeared normal on CUS; type III showed focal filling defects (Fig. 1D, 1d); and type IV showed complete no enhancement (Fig. 1E, 1e). In this study, types I and II were classified negative ALN, while types III and IV were positive ALN.
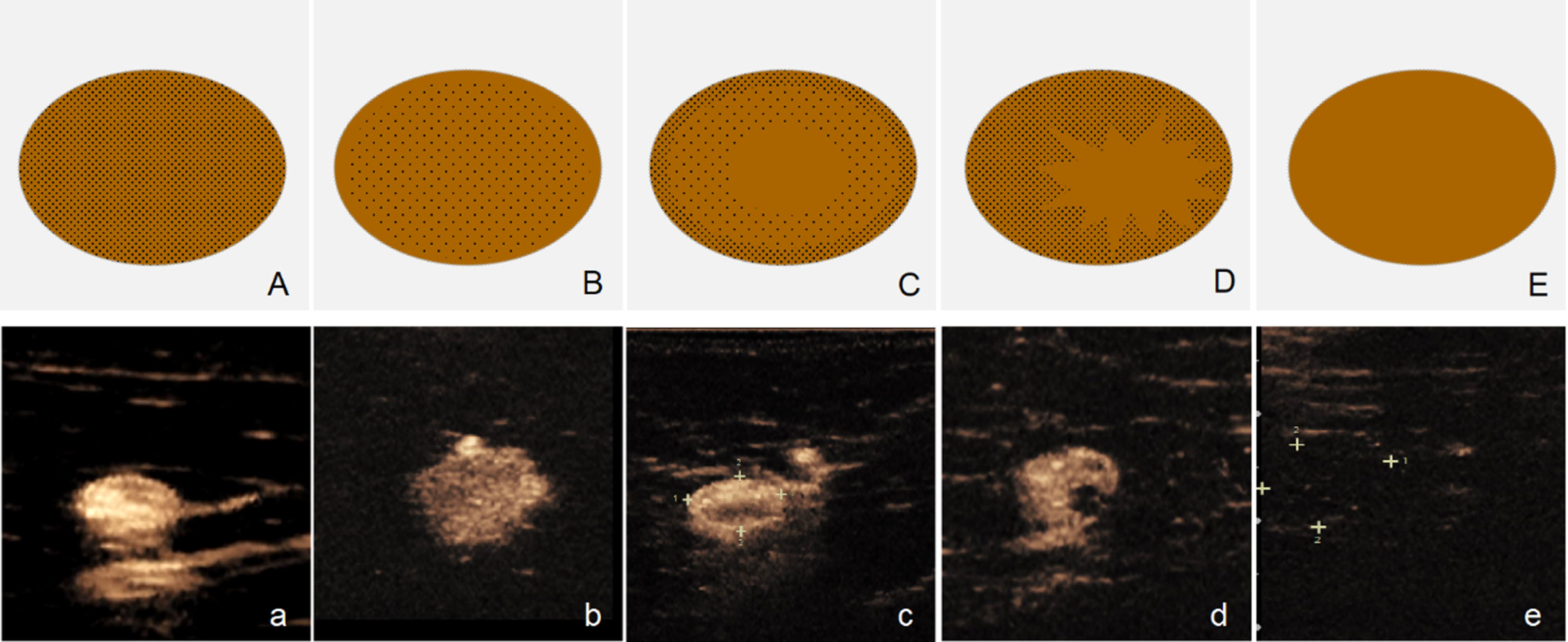
LCEUS showed 4 types (5 subtypes) enhancement patterns of SLN and corresponding schematic diagrams.
As shown in Table 3, different contrast-enhanced parameters (enhancement degree, enhancement boundary, internal homogeneity, perfusion mode, penetrating vessels, extended range) and enhancement patterns of SLN were summarized. The results showed that penetrating vessels (p < 0.05), extended range (p < 0.001) and SLN enhancement patterns (p < 0.001) were significantly different between ALN metastatic and nonmetastatic groups. However, the remaining parameters were not significantly associated with ALN status (p > 0.05).
Correlation of CEUS characteristics of primary lesion and enhancenment pattern of SLN versus the final pathology results of ALN
*Indicates significant values, P < 0.05.
Binary logistic regression analysis was further performed for indicators (tumor size, penetrating vessels, extended range, enhancement patterns of SLN) with statistically significant differences in univariate analysis, and the results showed that the extended range (cut of value: 0.525 cm) and enhancement patterns of SLN (type III and IV) were independent risk factors for ALNM (P < 0.001, Table 4). The combined diagnostic performance of the predictive model after including these two independent factors was better than that of any individual indicator (AUC 0.931, 95% CI: 0.887–0.976) (Fig. 2), demonstrating a sensitivity of 75.0% and specificity of 99.8% .
Binary logistic regression analysis factors predicting ALNM
Binary logistic regression analysis factors predicting ALNM
B, regression coefficients; SE Coeff, standard error of coefficient; OR, odds ratio; CI, confidence interval.
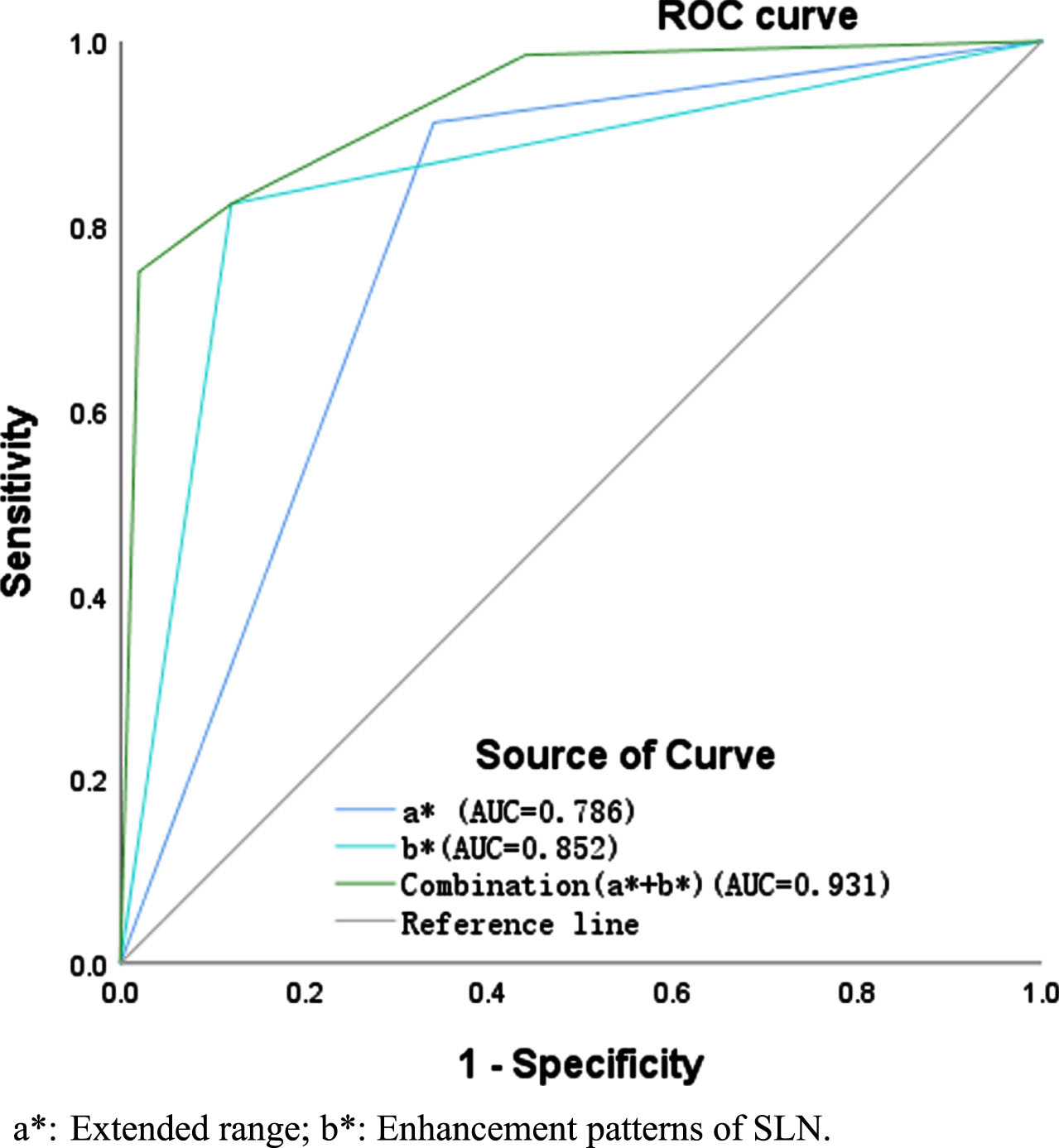
Receiver operating characteristic (ROC) curve of independent predictors and the combined indicators to predict ALNM.
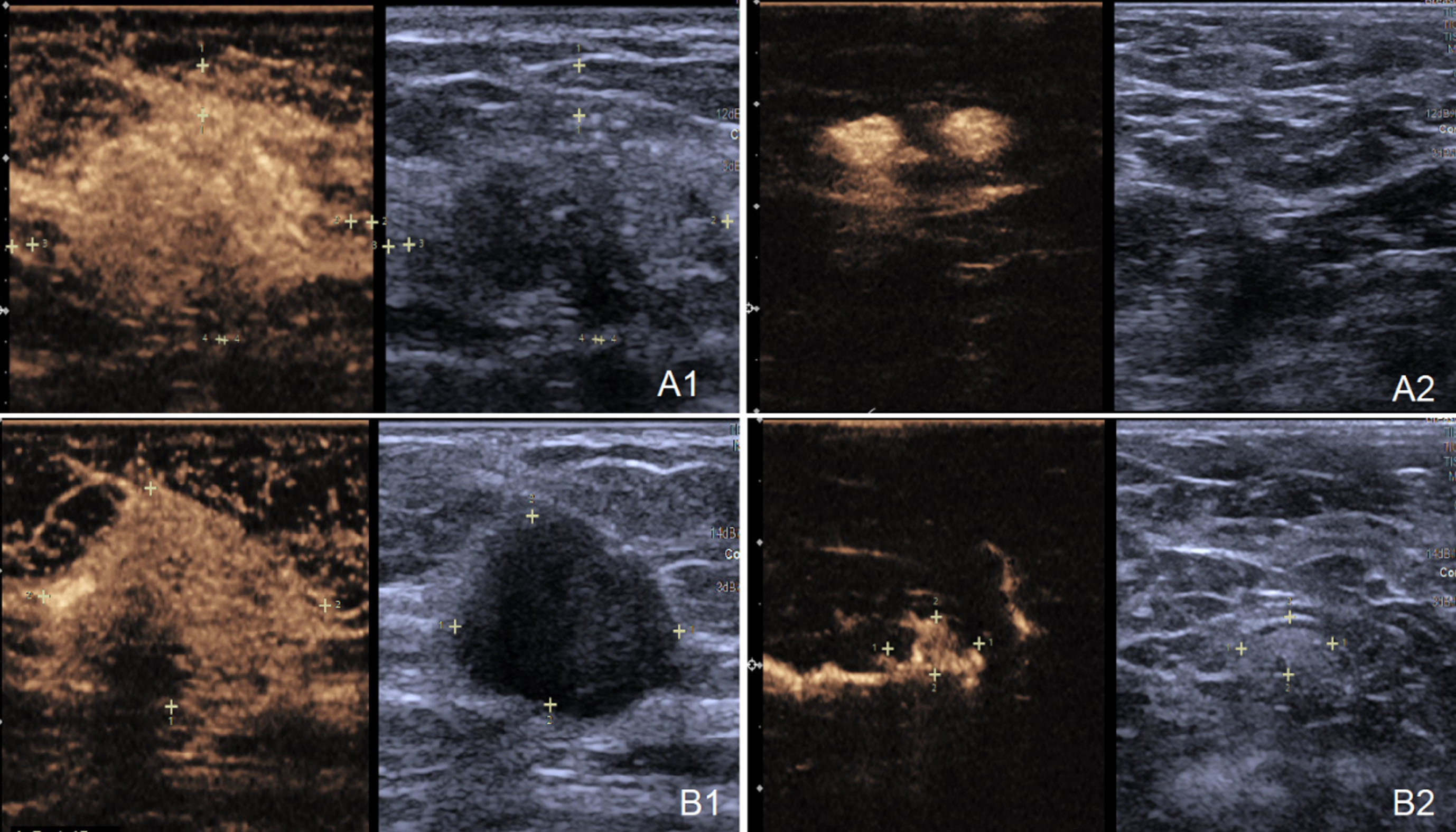
(A1) A 45-year-old woman presented with invasive ductal carcinoma confirmed by preoperative core needle aspiration pathology. The extended range of the lesion was 0.37 cm after CEUS. (A2) LCEUS of the SLN showed a homogeneous and bright hyperenhancement pattern (type I). The final pathologic surgical results were obtained by SLNB and confirmed that there was no ALNM. (B1) A 68-year-old woman presented with invasive ductal carcinoma confirmed by preoperative core needle aspiration pathology. The extended range of the lesion was 0.66 cm after CEUS. (B2) LCEUS of the SLN showed a focal filling defects pattern (type III). The final pathologic surgical results were obtained by ALND and confirmed that there was ALNM.
Conventional ultrasound is the preferred method for ALN assessment [17]. However, it can be challenging to distinguish between normal and metastatic lymph nodes in the early stages of breast cancer [26]. This is because the morphological structure of lymph node doesn’t undergo significant changes during this phase. Therefore, accurate preoperative diagnosis or prediction of ALN pathological status has become an urgent clinical need. In this study, the characteristics associated with ALNM were screened by univariate and binary logistic regression analysis, and predictive models were developed and their diagnostic performance was assessed.
Previous studies have shown that the risk of breast cancer increases significantly with age [27]. Our study also suggests that older breast cancer patients may have an increased risk of ALNM. This reminds attention to axillary management in elderly breast cancer patients is highly desirable. With regard to the tumor size, our findings are consistent with results of previous studies [28–30]. Patients with larger lesion diameters are more likely to have ALNM, and it has also been shown that the size of the tumor diameter can further predict high/low metastatic burden [28]. Univariate analysis showed that patients with thick, twisted nutrient vessels observed intralesionally after contrast injection may be associated with an increased likelihood of ALNM. Tumor angiogenesis is closely related to tumor growth, differentiation, and invasiveness [31]. It has been demonstrated that microvessel density and microvessel area are independent predictors of lymph node metastasis in papillary thyroid carcinoma [32]. The blood supply of breast cancer is divided into two stages: the pre-vascular and vascular phases [33]. Pre-vascular lesions mainly rely on the penetration of normal blood vessels in the surrounding breast tissue, the tumor growth rate is slow and the invasiveness is weak at this stage; After entering the vascular phase, tumor cells secrete a large amount of vascular endothelial growth factor, and a large number of thick and twisted tumor vascular networks are formed in the lesions to provide necessary nutrients for cancer cells to maintain their growth and invasion ability. The external perfusion software (VueBox ™) for CEUS allows quantitative analysis of microvessel formation in the solid component of the lesion and achieves a more precise diagnosis of the lesion blood supply, so future studies can focus on this technique [34].
Binary logistic regression analysis in this study showed that the extended range of enhancement lesion was an independent predictor of ALNM in patients with early breast cancer, which is consistent with the results of Zhu et al. [29]. Previous studies have suggested that HER-2 gene stimulates the formation of tumor neovascularization and accelerates the infiltration of tumor cells into peripheral normal tissues, indicating the high invasiveness of tumors [35]. Therefore, CEUS is more realistic than CUS in demonstrating tumor lesion diameter. At the same time, our results further showed that the risk of ALNM is increased when the enhancement lesion with a more obvious the extended range than 0.525 cm.
In addition, the enhancement patterns of SLN was also an independent risk factor for predicting ALNM. SLN is the first station lymph node reached by the lymphatic drainage of the primary tumor, and its pathological status can represent the involvement of the overall ALNs [36, 37]. On the basis of previous studies [38], we further divided heterogeneous enhancement (type II) into benign enhancement patterns, containing diffuse hypoenhancement (type IIa) and annular or semi-annular enhancement (type IIb) and metastatic enhancement patterns that are focal filling defects (type III) [22, 40]. The reason why SLN showed annular or semi-annular enhancement may be due to some physical factors during lymphatic drainage [41]. The contrast agent first fills the cortical area along the lymphatics and then enters the medullary area, thus showing a tendency to fill from the margin to the center [42]. When massage is inadequate, lymphatic reflux pressure increases, causing the contrast agent to fill only the surrounding cortical area, thus showing semi-annular enhancement; Diffuse hypoenhancement may be associated with excessive contrast agent destruction and inadequate visualization due to untimely tracking after contrast agent injection. Focal filling defects and no enhancement are metastatic infiltrating areas of tumor cells in the SLN [43]. Thus, patients have an increased likelihood of ALNM when SLNs present with type III and IV enhancement patterns.
Sonazoid has a high affinity for reticuloendothelial cells, increasing the imaging time of SLN and favoring intraoperative biopsy over Sonovue as a lymphotracer [44]. It has been shown that LCEUS with percutaneous injection of Sonazoid successfully identifies SLN in patients with early breast cancer, which has high sensitivity and specificity for the diagnosis of SLN metastases [45]. In addition, the concordance between the body surface marking method and the blue staining was 95.8% when the patients remained in the supine position preoperatively and intraoperatively [39]. Therefore, novel intraoperative ultrasound using Sonazoid combined with body surface markers has great potential in SLN biopsy.
This study has some limitations. Firstly, the sample size is small, and future studies require larger sample sizes or even multicenter studies to prove our conclusions; Secondly, there is some subjectivity in the interpretation of SLN enhancement patterns. Thirdly, the predictive value for ALNM burden was not further explored in this study.
In conclusion, accurate preoperative prediction of ALNM risk is an important component in treatment decision-making. In the present study, the patients with a higher likelihood of ALNM are those with more obvious expansion of enhancement range (> 0.525 cm) and SLN presenting with type III and IV enhancement pattern. The predictive value of the combination of the two can provide a reference basis for clinicians to develop personalized treatment decisions.