
Abstract
BACKGROUND:
Venous malformations tend to retain their slow-flow behavior, even in progressive disease or regression following therapy.
OBJECTIVE:
The aim of this study is to analyze the development of acquired hemodynamic relevant arterio-venous fistulae in patients with slow-flow malformations.
METHODS:
This study is a retrospective analysis based on a consecutive local registry at a tertiary care Interdisciplinary Center for Vascular Anomalies. Patients with venous malformations and development of secondary arterio-venous fistulae were included. Indications for therapy of the vascular malformation were based on patients’ symptoms and complications. The following endpoints were of clinical interest and were assessed: origin of development of arteriovenous fistula, development of secondary comorbidities as a result of the vascular malformation. For analysis we focused on descriptive statistics.
RESULTS:
Out of 1213 consecutive patients with vascular malformations, in 6 patients perfusion changed from slow flow to arterio-venous fast-flow patterns. Four patients developed the fistula after local trauma in the area of the malformation, the other 2 patients developed the fistula due to progression of the disease and recurrent thrombophlebitis. These 2 patients had no trauma or interventions at the time of arterio-venous fistula development.
CONCLUSIONS:
Acquired arterio-venous fast-flow fistula in patients with slow flow vascular malformation is very rare and might be a result of local trauma or the progression of the disease with recurrent thrombophlebitis. Specific evidence-based treatment options for these patients do not exist.
Keywords
Introduction
Congenital vascular malformations consist of dysplastic, malformed vessels with a worldwide prevalence of 0.3–1.5% [1, 2]. They are classified according to the type of vascular channels involved: arterial, venous, lymphatic or capillary vessels, singularly or combined [3–8]. Slow flow malformations compromise venous, capillary and lymphatic vessels. Fast flow arteriovenous malformations consist of direct arteriovenous shunt-connections with increased blood flow. The terms “slow” flow versus “fast” flow indicate the flow patterns in the malformation.
Usually slow-flow malformations do not convert into fast-flow lesions. During a longer disease course, however, the venous malformation may lead to secondary comorbidities such as localized or disseminated intravasal coagulation (LIC/DIC), chronic venous insufficiency (CVI) or major amputation [9]. So far, changes in perfusion patterns have not been described, even after progression or development of secondary comorbidities.
The treatment concept of vascular malformations is built on adequate classification and the distinction between fast-flow and slow-flow lesions: fast flow malformations are treated with embolization and/or resection [10], whereas slow flow are treated by sclerotherapy, electrosclerotherapy, laser and/or resection. Therefore, development of arterio-venous fast-flow fistulas in patients with slow-flow malformations would change the therapeutic concept in these patients.
The aim of this study was to investigate the development of acquired arterio-venous fas flow fistula in patients with slow flow vascular malformations. In particular, we were interested in the frequency of and the potential reasons for slow flow/fast flow conversions in a large cohort of patients.
Methods
Study design
This study is a retrospective analysis based on a local prospective, consecutive registry at the Interdisciplinary Center for Vascular Anomalies at the University Hospital Halle and Regensburg. It includes all patients with vascular malformations and secondary, acquired arterio-venous fast-flow fistulas, who were treated between 01/2012 and 01/2022 by the main physician (WAW) and who are registered in the Halle registry. Since WAW has a decade-long experience in the treatment of vascular malformations across several institutions in Germany, numerous of his long-term patients continued their treatment in Halle, and were registered with their initial date of treatment at hospitals other than Halle. Therefore, in these cases the follow-up phase exceeded the 10-year period of the existence of the Halle registry at the time of this analysis. The study was approved by the Ethics Committee of the University Hospital Halle (reference number 2022-035) and registered at the University Hospital Regensburg Clinical Study Data Base before data analysis (Z-2022-1758-9).
Clinical procedures: Diagnostics and treatment
Patients who were referred to the tertiary care Interdisciplinary Center for Vascular Anomalies received standard diagnostic imaging including sonography, MRI, and/or angiography. All patients with vascular malformations were discussed in an interdisciplinary board involving at least vascular surgeons, pediatricians and radiologists. The decision for intervention was based on patients’ symptoms in consensus.
Patients with slow flow vascular malformations received sclerotherapy, electrosclerotherapy, operative resection and conservative treatment like compression stockings and physiotherapy. In case of development of arterio-venous fistulas, treatment options were mainly embolization and electrosclerotherapy.
Outcome assessment and follow-up
All patients were followed-up 3 months after the intervention and once a year thereafter on a routine base with clinical examination, ultrasound and MRI. The patient records, imaging and documented results of clinical examinations were analyzed. Development of arterio-venous fistulas were assessed by MRI including dynamic contrast-enhanced MR-angiography sequence “Time-resolved angiography With Interleaved Stochastic Trajectories” (TWIST), T2 STIR, T1 TSE - native/with Gadolinium, T1 VIBE 3D and T2 TSE.
Registry and documentation
All malformation patients were diagnosed and treated at a tertiary care center, mainly by one physician (Interdisciplinary Center for Vascular Anomalies Regensburg and Halle). Clinical and imaging data were collected consecutively using the institutional electronic hospital information system (Orbis®, Dedalus Healthcare Group, Florence, Italy) throughout the observation period by trained staff in a standardized way. Data from malformation patients were retrieved from this data base, anonymized and then documented on a study-specific paper-based case report form (CRF).
All patient-related variables were documented by the study physician (DS) and independently checked by a second person (BC). Discrepancies were resolved by cross-checking original data in the hospital information system (source data verification).
Statistical analysis
In the present analyses we focused on descriptive statistics including counts, percentages, medians and interquartile ranges (IQR).
Data were analyzed using SPSS version 26.0 (IBM, Armonk, NY, USA).
Results
Patient characteristics and onset of symptoms
From 01/2012 –01/2022 a total of 1213 patients with vascular malformations were seen by the main physician WAW and entered into the Halle Registry.
Six out of 1213 patients (0.5%) developed changes in perfusion pattern from slow-flow venous malformation to development of arterio-venous fast-flow fistula after trauma or due to progression of the disease (Table 1). Median age at development of acquired secondary arterio-venous fistula was 16.5 (IQR 14.75–20.75) years. At the time of the last follow-up of these 6 patients their median age was 30.5 (IQR 19–48).
Summary of patient characteristics
Summary of patient characteristics
*At the time of last follow-up.
The diagnosis of secondary arterio-venous fast.flow fistulas was triggered by increased local symptoms (mainly pain and swelling), which indicated follow up imaging in ultrasound and MRI. Four patients had developed arteriovenous fast-flow fistula after local trauma in the area of the venous malformation at median age of 16.5 years (IQR 14.5 –26), 2 patients developed arteriovenous fistula due to progression of the extensive disease at median age of 16.5 years (IQR 16.5 –16.5; Fig. 1). Trauma was local injury due to fall from a horse, local trauma with bone fracture in the area of the malformation, fall with knee trauma and venous malformation at the knee, and local trauma with heavy blow at the area of the malformation. Number of previous treatment interventions for the venous malformation in patients with acquired arteriovenous fistula due to progression of the underlying disease was in median 6.5 (IQR 5 –6.5) and in those after trauma was 6.5 (IQR 5 –10.5).
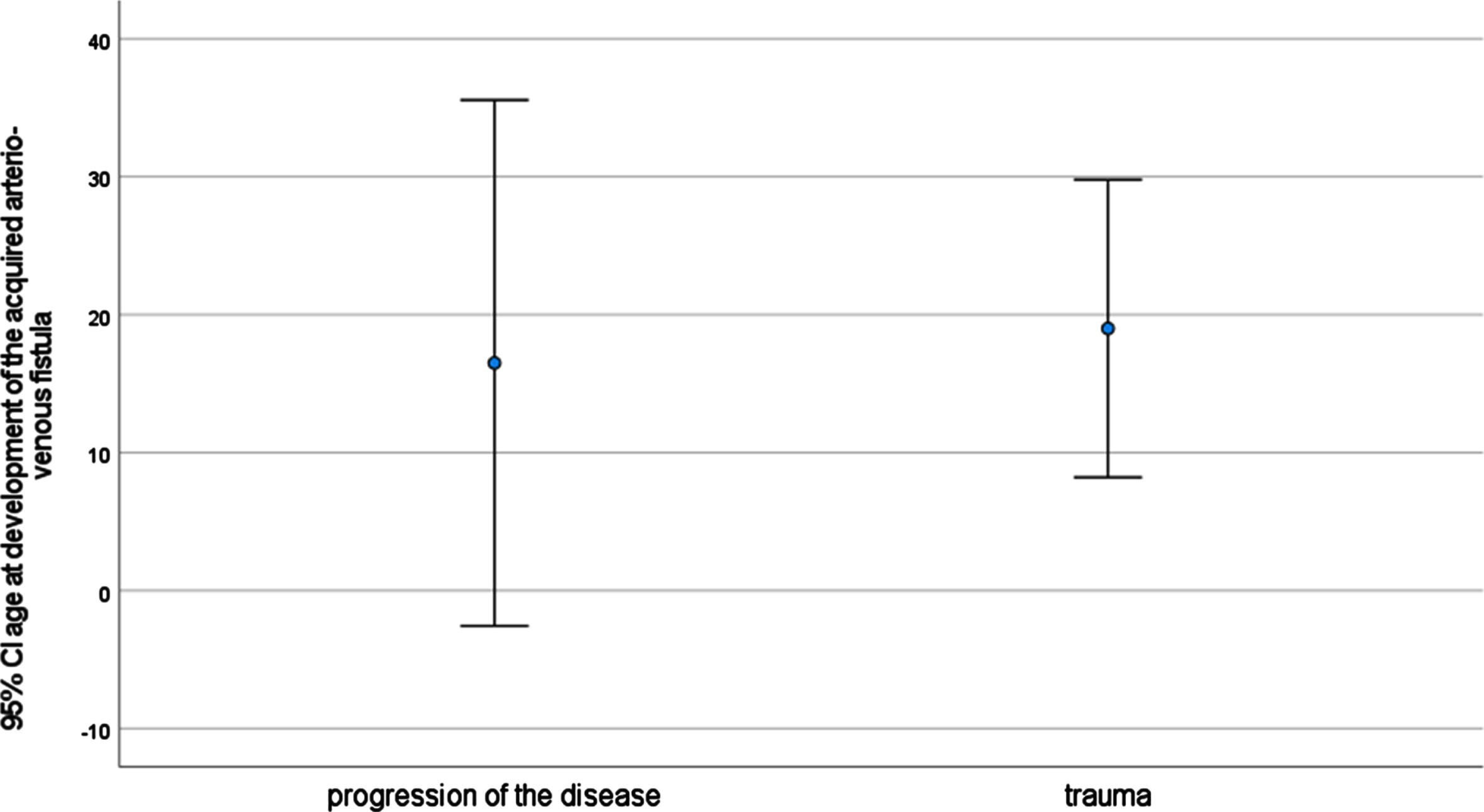
Age at development of acquired arterio-venous fistula. Four patients developed arteriovenous fistula after trauma at median age of 16.5 (IQR 14.5 –26), 2 patients developed arteriovenous fistula due to progression of the disease at median age of 16.5 (IQR 16.5 –16.5).

Number of required interventions to achieve stable disease and development of secondary arteriovenous fistula. Number of interventions was in patients with arteriovenous fistula due to progression of the disease median 6.5 (IQR 5 –6.5) and those ones after trauma 6.5 (IQR 5 –10.5).
The arteriovenous fistula was treated by transarterial embolization in 5 cases (Fig. 3, 4), in one patient the acquired fast-flow fistula was covered by a stentgraft. All patients received additional sclerotherapy for treatment of the slow flow malformation. Closure of the fistula was achieved in all cases. One patient presented 7 years after initial embolization treatment of the fistula with recurrent arterio-venous fast-flow fistula due to again a progression of the disease and recurrent thrombophlebitis (Fig. 5). One patient having undergone transarterial embolization had recurrence of the arteriovenous fistula after one year and received re-embolization and electrosclerotherapy for further treatment which led to ongoing, complete resolution of the AV fistula (Fig. 6).

Embolization of an acquired arteriovenous fistula. A. Acquired arteriovenous fistula of the deep femoral artery after trauma. B. Embolization of the fistula with onyx®.

Diagnostics and embolization of an acquired arteriovenous fistula. A. Diagnostics with ultrasound and B. MRA. C. Angiography of the arteriovenous fistula of the deep femoral artery. C. Sclerotherapy of the fistula.

Acquired recurrent arterio-venous fistula due to progression of the disease: angiography and MRI. The patient developed a huge number of small arterio-venous fistulas, till the microcirculation changes became hemodynamic relevant.

Recurrent arteriovenous fistula. A. Angiography of the recurrent arteriovenous fistula of the deep femoral artery. B. Embolization and electrosclerotherapy of the fistula.
All 6 patients had recurring thrombophlebitis in their malformation. Two patients had localized intravasal coagulation (LIC) and received therapeutic anticoagulation. One patient developed a high-output cardiac state with tachyarrythmia. That patient had a positive outcome after occlusion of the arteriovenous fast-flow fistula and treatment of the malformation with electrosclerotherpy. Closure of the fistula was achieved in all 6 patients, one patient had recurred bleeding due to LIC. That patient did not present for regular follow up after closure of the fistula. She came as an emergency with gastrointestinal bleeding do to progression of LIC 7 years after treatment of the fistula. She received the mTOR inhibitor sirolimus following intervention of the bleeding due to progression of the disease (Fig. 5). For therapy of the intestinal bleeding she received coloscopy with coloscopic-guided interventional sclerotherapy of the venous malformation.
One patient was treated with the mTOR inhibitor sirolimus due to extensive disease. The other patients were all treated interventionally by embolization and sclerotherapy. Four patients received therapeutical anticoagulation due to recurring thrombophlebitis. Out of them, 2 patients developed arteriovenous fistula, due to progression of the disease (Fig. 7).

Classification if vascular malformations. Regarding the flow pattern, vascular malformations are classified into slow flow and high flow malformations. In rare cases, patients with slow flow malformation might develop arterio-venous fistula after local trauma or progression of the disease with increased number of small arterio-venous fistulas.
Secondary comorbidities due to the vascular malformation
In the present study, we investigated the development of fast-flow arteriovenous fistulas in patients with slow flow venous malformation.
The occurrence of the acquired arteriovenous fistula was due to progression of the initially slow-flow venous malformation with increased chronic inflammation-related perfusion of the surrounding tissue due to recurring thrombophlebitis and or following local trauma with suspected laceration / rupture of part of the venous malformation. There was no difference in the number of interventions of the two groups, aquired arterio-venous fistula after trauma or due to progression of the disease. Likewise, number of required interventions to achieve stable disease in patients with acquired arteriovenous fistula due to progression of the disease was the same in trauma and non-trauma patients.
Acquired arteriovenous fast-flow fistulas are generally very rare. Asensio et al found only 201 articles including 291 patients of acquired A-V fistulas, generally after trauma. Most commonly involved were the vessels of the extremities. Secondary arteriovenous fast-flow fistula after treatment of vascular malformations or due to increased perfusion of the malformation due to recurrent chronic inflammation was not documented so far [15].
Acquired arteriovenous fistulae in patients with slow flow venous malformation might be a result of trauma causing penetrating injury with vessel laceration or rupture. Thus in concomitant injury of dysplastic venous malformation and accompanying arteries a direct connection may develop. Another cause may be continuous progression of the disease with chronic local inflammatory reaction due to LIC and recurrent thrombophlebitis. The constant inflammation might develop as a first step changes in micropersufion with small hemodynamically irrelevant arterio- venous fistula. With increased number of these fistulas, the hemodynamic changes are becoming more relevant and may increased to hemodynamically relevant fast-flow AVF over time.
Diagnosis in this series was performed by clinical exam, ultrasound, and MRI. During intervention, conventional ultrasound was performed for intervention guidance. So far contrast-enhanced ultrasound (CEUS) was not performed to detected early development of arterio-venous fistulas. Nevertheless, CEUS might be a valuable diagnostic tool in order to detect small changes in microperfusion in patients with progression of their slow flow malformation [17]. Regarding to the costs, ultrasound diagnosis is less expensive than other diagnostic options, but its quality is physician-dependent. Changing the diagnostic approach to reduce the number of MRI exams might be beneficial. Macroperfusion is assessable with time resolved contrast-enhanced MR-angiography (e.g. TWIST), whereas microperfusion can also be quantified by dynamic contrast enhanced perfusion imaging or arterial spin labeling. Using CEUS, microperfusion changes can be readily detected. The exact localization of deeply situated lesions to guide intervention however might be difficult to visualize.
The treatment options in case of the development of fast-flow arterio-venous fistulae were embolization and coverage by stentgraft [18]. Successful treatment was analyzed during follow up by ultrasound and MRI with MR-angiography: all patients showed venous flow in the malformation, thus regaining their status as slow-flow lesions.
A wide range of treatment options are offered to each patient, including sclerotherapy, electrosclerotherapy, embolization, operative resection or conservative treatment including anticoagulation, mTOR or RAS inhibitors [11–13]. Nevertheless, the development of these fast-flow fistulas could not be prevented in all patients with venous malformations, even in patients with regular follow-up.
Secondary comorbidities with CVI and lymphedema are frequent in patients with vascular malformations [14]. In this study, none of the patients developed chronic venous insufficiency. Two patients developed localized intravascular coagulation and one patient developed a high-output cardiac state with tachyarrhythmia.
In conclusion, the development of acquired fast-flow arteriovenous fistulas in patients with slow flow venous malformations is very rare. When they occur, penetrating direct trauma with vessel injury are the most likely cause for these fistulas. Another cause is the progression of the vascular disease with multiple, chronic local inflammatory reactions might lead to fistula development. Individualized treatment with a combination of interventional and conservative treatment can be offered as treatment options, but due to the rarity of there are no evidence-based treatment standards.
Authors’ contributions
All authors contributed to the conception and design of the study.
All authors revised the article and gave their final approval for the version to be published. All authors gave their agreement to be accountable for all aspects of the work.
Conflict of interest
The authors declare no conflict of interest regarding to this study.