
Abstract
BACKGROUND/OBJECTIVE:
Oral malformations of the tongue are exceedingly rare. The aim of this study was to evaluate the effectiveness of individualized treatment for patients with vascular malformations of the tongue.
METHODS:
This retrospective study is based on a consecutive local registry at a tertiary care Interdisciplinary Center for Vascular Anomalies. Patients with vascular malformations of the tongue were included. Indications for therapy of the vascular malformation were macroglossia with the impossibility to close the mouth, bleeding, recurrent infection and dysphagia. Size regression of the malformation (volume measurement) and symptom improvement were investigated.
RESULTS:
Out of 971 consecutive patients with vascular malformations, 16 patients suffered from a vascular malformation of the tongue. Twelve patients had slow-flow malformations and 4 fast-flow malformations. Indications for interventions were bleeding (4/16, 25%), macroglossia (6/16, 37.5%), and recurrent infections (4/16, 25%). For two patients (2/16, 12.5%), there was no indication for intervention due to absence of symptoms. Four patients received sclerotherapy, 7 patients Bleomycin-electrosclerotherapy (BEST) and 3 patients embolization. Median follow-up was 16 months (IQR 7–35.5). In all patients, symptoms had decreased after two interventions at a median (IQR 1–3.75). Volume reduction of the malformation of the tongue was 13.3% (from median 27.9 cm3 to median 24.2 cm3, p = 0.0039), and even more pronounced when considering only patients with BEST (from 86 cm3 to 59.1 cm3, p = 0.001).
CONCLUSION:
Symptoms of vascular malformations of the tongue are improved after a median of two interventions with significantly increased volume reduction after Bleomycin-electrosclerotherapy.
Keywords
Introduction
Congenital vascular malformations (VMs) were errors in vascular development and consist of dysplastic vessels [1, 2]. Malformations are divided into slow-flow lesions (capillary, venous and lymphatic), fast-flow anomalies (arterio-venous) or combined malformations [3–8]. Progression of VMs may occur during follow-up, with accentuation after trauma or during adolescence [9]. The frequency of oral malformations is 1.3% of all VMs [10]. Among the oral malformations, often the tongue is affected. Clinically vascular malformations of the tongue lead to macroglossia, dysphagia, pain, bleeding as well as impairments of speaking or even breathing [11]. Macroglossia is defined as enlargement of the tongue that results in its protrusion beyond the teeth or alveolar ridge in its natural resting state [1, 12].
The treatment options for all patients including children for VMs are based on flow properties of the lesions. In the presence of hemodynamically relevant shunting, as in arterio-venous malformations (AVMs), embolization and/or operative resection is suggested [13]. In slow-flow malformations, the gold standard is sclerotherapy [14, 15]. Recently, we could show clinical response in 87.5% of AVMs of the face after image-guided embolization [16] and the effectiveness of Bleomycin-electrosclerotherapy (BEST) in recurrent venous malformation [17].
So far, there are no guidelines for treatment of VMs of the tongue. Therefore, the aim of this study was to evaluate effectiveness of individualized treatment for patients with VMs of the tongue: image-guided embolization in case of fast-flow malformations and sclerotherapy or BEST in case of slow-flow malformations.
Methods
Study design
This study is a retrospective analysis based on a local prospective registry of the Interdisciplinary Center for Vascular Anomalies and includes patients with VMs in the tongue, who were treated between 10/2017 and 10/2022. The study was approved by the Ethics Committee of the University Hospital Halle (reference number 2022–205) and registered at the University Hospital Regensburg Clinical Study Data Base before data analysis (Z-2021–1683–4).
Clinical procedures: Diagnostics and treatment
Patients who were referred to the tertiary care Interdisciplinary Center for Vascular Anomalies received standard diagnostics including clinical examination, imaging including sonography, magnet resonance imaging (MRI), and/or angiography. All patients with vascular malformations of the tongue were discussed in an interdisciplinary board involving at least vascular surgeons, pediatricians and radiologists. The decision for intervention was based on patients’ symptoms in consensus.
Symptomatic patients received sclerotherapy, BEST, or embolization, whereas asymptomatic patients were monitored in clinical follow-ups. BEST was used off-label; all patients and/or their guardians provided written informed consent.
Outcome assessment and follow-up
Nine of 16 patients underwent routine clinical and MRI follow-up. Due to the SARS-COV-2 pandemic and clinical restrictions, clinical and MRI follow-up could not be conducted in seven patients. Here, patient records were completed by telephone interviews. While we targeted for follow-up periods of 9 months after intervention, individual circumstances caused varying periods ranging between 4 –27 months. The patient records, imaging and documented results of clinical examinations were analyzed. To assess treatment related complications, the patients received color-coded Doppler sonography of the neck vessels before and after treatment. Treatment response was assessed by estimating the volume of the malformation in the tongue based on axially acquired fat-saturated T2-weigthed MR images (typically obtained from T2-weighted short tau inversion recovery (STIR) sequences, but also from conventional T2-weighted turbo-spin-echo sequences with fat-saturation pulses if STIR sequences were unavailable) before and after intervention (during follow-up). To reduce contributions of partial volume effects, the MR images were interpolated (type: cubic interpolation) along the slice axis to provide isotropic spatial resolutions ranging between 0.7 mm and 0.85 mm prior to the manual delineation of the malformation using ITK-SNAP (http://www.itksnap.org). Clinical morphological success is defined by volume reduction, and less bleeding, infections and/or dysphagia.
Registry and documentation
All patients with malformations were diagnosed and treated in a specialized tertiary care center for VMs (Interdisciplinary Center for Vascular Anomalies Halle). Clinical and imaging data were collected consecutively using the institutional electronic hospital information system (Orbis®, Dedalus Healthcare Group, Florence, Italy) throughout the observation period by trained staff in a standardized way. Data from malformation patients were retrieved from this data base, anonymized and then documented on a study-specific case report form (CRF).
All patient-related variables were documented by the study physician (MG) and independently checked by a second person (BC). Discrepancies were resolved by cross-checking original data in the hospital information system (source data verification).
Statistical analysis
In the present analyses, we focused on descriptive statistics including counts, percentages, medians and interquartile ranges (IQR). Statistical difference between malformation volumes before and after intervention is probed using Wilcoxon signed-rank test. Data were analyzed using SPSS version 26.0 (IBM, Armonk, NY, USA).
Results
Patient characteristics and onset of symptoms
From 10/2017 –10/2022 a total of 971 patients with vascular malformations were seen at the Interdisciplinary Center for Vascular Anomalies Halle by two physicians (WAW, MG). Out of them 16 patients (1.6%) had a vascular malformation of the tongue (Table 1). Two patients exhibited no symptoms and received regular follow-up. Median age of these 16 patients was 6 years (IQR 2–8,5).
Demographics of included patients. Based on 917 patients, 16 patients showed malformations of the tongue
Demographics of included patients. Based on 917 patients, 16 patients showed malformations of the tongue
The individualized treatment schedule for malformations affecting the tongue is graphically outlined in Fig. 1. Table 2 summarizes the demographics and intervention procedure of our patient cohort suffering from malformations of the tongue. Embolization was performed in patients with fast-flow malformations (3/16 patients). One AVM patient with macroglossia and bleeding received BEST additional to unsatisfactory embolization result (patient 1). In case of slow-flow malformations, sclerotherapy was performed (7/16 patients). Patients with complicated VMs have received addition medical therapy with mTOR inhibitor Sirolimus (patient 2, 3, 5, 7, 8, 16). Exemplarily, a patient with slow-flow malformation is shown before and after therapy in Fig. 2 and the interventional procedure from another patient with fast-flow malformation is illustrated in Fig. 3.

Individualized treatment scheme for treating vascular malformations of the tongue.
Individual patients with malformation of the tongue
Pat. No. Patient number, y years, f female, m male, AVM Arterio-venous Malformation. LM Lymphatic Malformation VM Venous Malformation VLM Veno-lymphatic Malformation BEST Bleomycin-electrosclerotherapy.
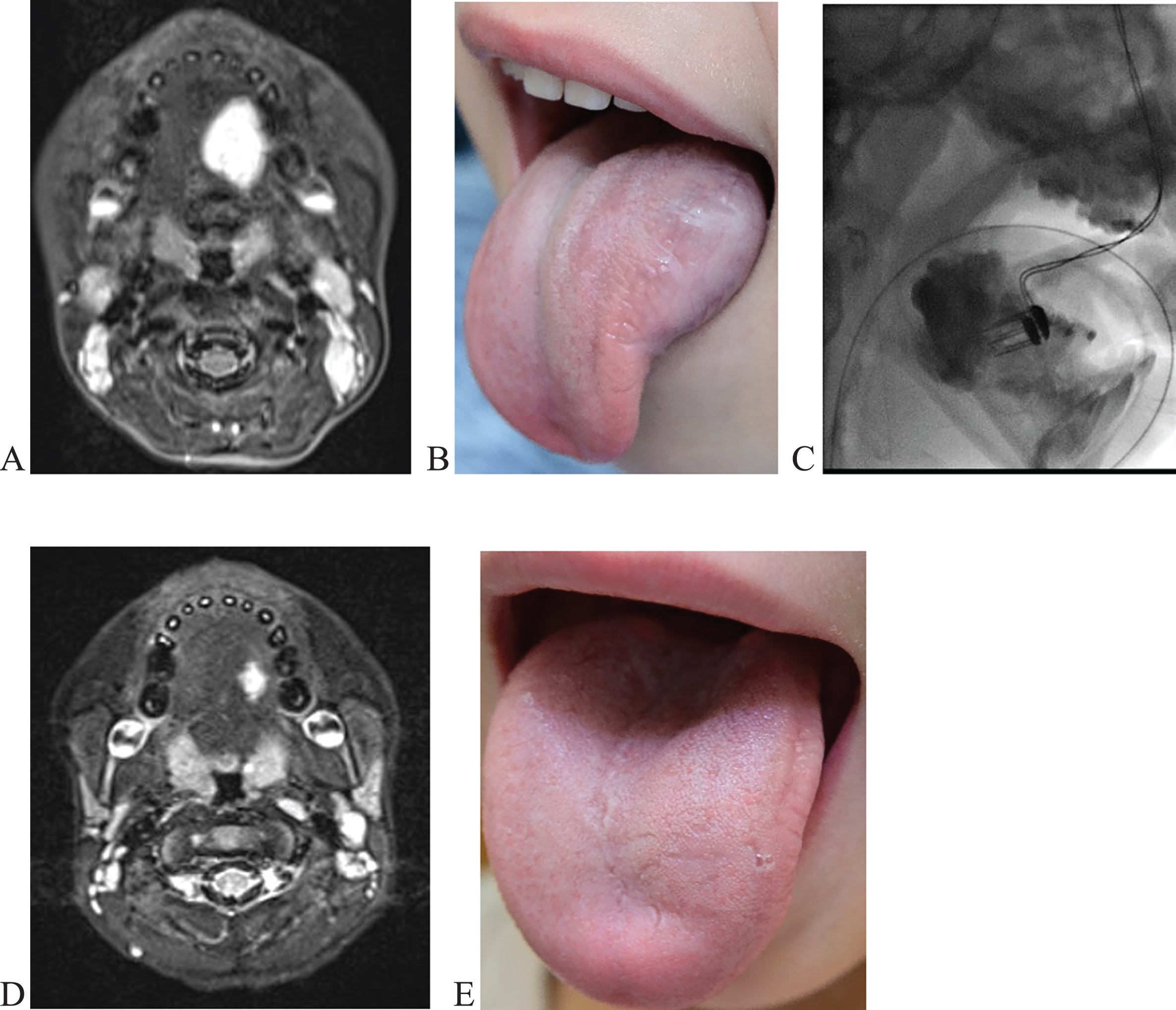
6-year-old boy with venous malformation of the tongue (patient #12). A,B Pre-therapy shows venous malformation of the tongue left sided. C Digital subtraction angiography demonstrates intraoperativ BEST. D,E Nine months follow-up shows significant reduction.

6-month-old boy with arterio-venous malformation of the tongue (patient #14). Digital subtraction angiography images demonstrate intraoperative embolization. A before and B after embolization of the right arteria lingualis with histoacryl and lipiodol embolization with complete occlusion.
Color-coded Doppler sonography of the neck vessels before and after treatment revealed no deep venous thrombotic process was detected. Complications like impairment of sensibility, palsy or adverse reactions such as bleomycin-induced pneumonitis or interstitial lung disease were not observed.
In median, the follow-up period was 16 months (IQR 7–35.5). In all patients, less severe clinical symptoms were observed after 2 interventions at the median (IQR 1–3.75). All patients showed improved mobility of the tongue.
The lesion volumes, measured in 9 patients before and after intervention (Table 1, Fig. 4), were significantly lower after treatment (p = 0.0039). The median lesion volumes before and after treatment were 27.9 cm3 (IQR 12–85 cm3) and 24.1 cm3 (IQR 6.5–59.1, 0.68–83.78 cm3), respectively. Lesion volume reduction was even more pronounced when only focusing on interventional BEST (n = 5, from 86 cm3 to 59.1 cm3, p = 0.001).

Volume of the lesion before and after intervention. Wilcoxon signed-rank test indicates a statistically significant reduction of the lesion after interventions.
In the present study, we investigated the outcome of patients’ individualized treatment in VMs of the tongue; including volume measurements and clinical symptoms. While the development of standardized guidelines for treatment of VMs has started in 2022 (AWMF reference number 01VSF21001), there are no guidelines yet for the treatment of VMs of the tongue.
Recently, we could show a therapy response in 21 of 24 patients (87.5%) with fast-flow malformations of the face, treated with image-guided embolization [16]. No patients with VMs of the tongue were included in that study. Encouraged by our favorable results after BEST in case of recurrent slow-flow malformations [17], we designed a patient individualized treatment algorithm for patients with malformations of the tongue: in case of macroglossia, patients received embolization for fast-flow malformations. In slow-flow malformations in the absence of macroglossia, patients were treated with either BEST or sclerotherapy.
Certain case reports have been published on the treatment of VMs of the tongue and only a few small case series [18–20]. Outcome measurements were only based on clinical examination [18, 20]. So far, there are no further studies assessing outcome of BEST and/or volume measurement pre- and post-intervention of the tongue.
Fat-saturated T2-weighted imaging (e.g. using STIR or fat saturation pulses) reveals the lesion of the malformation and its relationship to the involved anatomic architecture. Slow-flow VMs consistently display high signal on fat-saturated T2-w images and no flow-related signal voids. The high signal is the result of the stagnant liquid content of the VMs. On T2-w images, there may also be surrounding edema if a spontaneous thrombosis is present. In T1-w contrast-enhanced imaging, no arterial or early venous enhancement, but a slow gradual peripheral enhancement is demonstrated in venous malformations [21]. MRI is most suited to evaluate imaging outcomes after successful treatment. Based on fat-saturated T2-w images, volume reduction was in total 13.3% across nine patients and even 40.2% after BEST when only considering patients with BEST of the tongue. After intervention we observed signal intensity (SI) decreases in the former lesions resulting in diminishing SI areas or regions with elevated heterogeneity. In general the signal intensities within the former malformation were lower in the follow-up; caused by the reduced vascular density after intervention [17]. A more direct way to assess microcirculation of the malformation is to carry out fat-saturated T1-weighted imaging without and with gadolinium-based contrast agent. The specific time-resolved contrast agent enrichment in larger and mesoscopic vessels, accessible via contrast-enhanced dynamic MRI, provides access to the different hemodynamic characteristics of vascular anomalies [22].
Microcirculation changes may also be detected using specific ultrasound (US) imaging techniques like contrast-enhanced ultrasound (CEUS) or superb microvascular imaging (also known as microvascular flow imaging). These US-techniques were, for instance, able to improve the differentiation between benign from malignant solid breast lesions [23] or to detect intraplaque neovascularization in patients with atheromatous carotid artery plaque [24]. In principle, these ultrasound-based techniques can also be applied to detect microcirculation changes in patients with vascular malformation [25, 26]. Because of the limited ultrasound access to the whole tongue examinations using US at the tongue are complicated and less effective. US of the tongue may only be useful for local issues like biopsy or abscess draining [27, 28].
In our experience, one disadvantage of BEST is the occurrence of more pronounced swelling and pain as compared to conventional sclerotherapy. Increased swelling and pain were observed in all of our patients; in two patients circumscribed small necrosis of the tongue occurred without the need for surgical correction. All side-effects disappeared by conservative therapy. No major complications were observed. None of our patients showed tricytopenia which would be a contraindication for BEST.
A significant percentage of patients will suffer from their VMs again after treatment. In our study, the number of interventions that were required to reduce clinical symptoms was 2 at a median. In 6 patients more than two interventions (range 3 –9) were performed due to recurrence of the disease. Extensive treatment might lead to angiogenesis and microcirculation changes, hence, patient individualized restrictive treatment has been suggested [12]. Interventional therapy alone may not be enough for treating those patients. The relapse was stopped by additional BEST in 4 cases and specific medication with mTOR inhibitors in 6 cases. Sirolimus is known as safe and effective drug for complicated vascular anomalies [29]. The success of Sirolimus in combination with sclerotherapy has been demonstrated, recently [30]. Most AVMs in the tongue will not be controlled by embolization alone, and additional surgery may be required [19]. Hence, biomarkers for better identification of patients with high potential of recurrence are urgently needed.
In conclusion, a patients’ individualized treatment in case of vascular malformation of the tongue leads to symptom reduction and volume reduction of the tongue in particular in case of additional macroglossia. BEST leads to the most significant volume reduction of the vascular malformation.
Authors’ contributions
All authors contributed to the conception and design of the study.
All authors revised the article and gave their final approval for the version to be published. All authors gave their agreement to be accountable for all aspects of the work.
Conflict of interest
The authors declare no conflict of interest regarding to this study.