
Abstract
AIM:
To assess the feasibility and efficiency of contrast-enhanced ultrasound (CEUS) real-time guided fine needle aspiration (FNA) for sentinel lymph node (SLN) of breast cancer.
MATERIALS AND METHODS:
This retrospective study reviewed 21 breast cancer patients who scheduled for surgical resection performed CEUS real-time guided SLN-FNA and intraoperative SLN biopsy (SLNB). The success rate of CEUS real-time guided SLN-FNA was analyzed. The FNA diagnostic efficiency of SLN metastasis was analyzed compared to SLNB.
RESULTS:
Twenty-six SLNs were detected by intradermal CEUS whereas 130 SLNs were detected by SLNB. The median SLNs detected by intradermal CEUS (n = 1) and by SLNB (n = 5) was significantly difference (p < 0.001). All 26 CE-SLNs of 21 patients were successfully performed intradermal CEUS dual image real-time guided SLN-FNA including 5 SLNs of 4 patients which were difficult to distinguish in conventional ultrasound. Compared to SLNB, FNA found 2 of 5 cases of SLN metastasis, the diagnosis sensitivity, specificity, positive predictive value, negative predictive value, false negative rate, false positive rate and Yoden index were 40%, 100%, 100%, 84.2%, 60%, 0%and 40%, respectively.
CONCLUSION:
SLN-FNA real-time guided by dual CEUS image mode was technically feasible. Patients with a positive SLN-FNA should be advised to ALND without intraoperative SLNB according to Chinese surgeon and patients’ conservatism attitude. But a negative SLN-FNA did not obviate the need of conventional SLNB because of the high false negative rate.
Introduction
The most common metastasis site of breast cancer was axillary lymph nodes (ALN). Status of ALN metastasis was closely related to the survival of breast cancer patients and may influence treatment plans and prognosis assessment [1–4]. Anatomically, the definition of sentinel lymph node (SLN) was the first node that receives lymphatic drainage of relevant organ or tissue. Thus, SLN of breast cancer was defined as the first lymph node to receive lymphatic drainage of the tumor [5, 6]. According to the recommendation of American Society of Clinical Oncology (ASCO) and National Comprehensive Cancer Network (NCCN), SLN biopsy (SLNB) was suggested for tumor staging [7, 8]. Compared to traditional ALN dissection (ALND), SLNB was less traumatic, and ALND brought too many complications such as edema, movement restricted and numbness [9, 10].
Currently, the common tracer of standard SLNB of breast cancer patient were technetium-labeled nanocolloid and blue dye. Surgeons found and removed the SLN according to the indication of the tracer after the injection around the areola or the tumor [10–12]. But the shortcomings were not negligible concerning radioisotope and blue dye for SLNB. Blue dye was easy to enter the next lymphatic nodes or lymph vessel because of its small molecular weight, causing unnecessary removal of too many non-sentinel lymph nodes (nonSLNs). Using of radioactive colloid prolonged the SLNB procedure and patients and healthcare workers have to endure to expose to radiation. Otherwise, in some countries, the use of radioisotopes was restricted [9, 12–14].
Conventional ultrasound and CEUS have been widely used in lymph node detection [15, 16]. Recently, application of ultrasonic microbubble in SLN has been reported. The lymphatic channel from breast to axilla and SLN was clearly displayed after intradermal injection of ultrasonic contrast agent. According to previous study, the identification rate of SLN detected by contrast enhanced ultrasound CEUS (CE-SLN) was from 70%to 100%[17–24]. Further, Zhong et al. reported that translymphatic CEUS combined with fine needle aspiration (FNA) of SLN was a accurate and less invasive procedure to assess ALN status preoperatively. They claimed that similar with SLNB, this procedure might be a reliable indicator for ALND [23].
Clinically, ultrasound guided FNA was usually applied in distinguishing benign and malignant nodules and identifying lymph node metastasis [24, 25]. Most SLNs can be displayed on both conventional ultrasound and CEUS images. However, some SLNs were similar to the echo of surrounding tissue and cannot be easily distinguished by conventional ultrasound. Sever et al reported that 40%of the assumed SLN can be recognized only on CEUS imaging mode [24]. Theoretically, FNA of the above SLNs can be realized by applying CEUS real-time guidance. Although CEUS was able to identify SLN, it had not been reported whether CEUS can display the puncture needle in real time when FNA was guided by CEUS with a lower mechanical index. The aim of the present study was to investigate the feasibility and efficiency of preoperative assessment of SLN metastasis of CEUS real-time guidance of FNA in SLNs of breast cancer.
Patients and methods
Patient selection
This retrospective study was approved by the local institutional ethics committee (Code:2020-P2-177-01), and informed consent was exempted. A review of Ultrasound Department and Breast Surgery Department database of breast cancer inpatients from December 2018 to November 2019 was performed. Female breast cancer patients without ALN metastasis, performed intradermal CEUS real time guided SLN-FNA and intraoperative SLNB, finally performed breast removal and/or ALND were included in the present study. There were no radiological or clinical signs of ALN metastasis preoperatively. Patients with lymph node or distant metastases, history of radiotherapy, neo-adjuvant chemotherapy, related surgery of corresponding breast or axilla, local infections and deeper layer of axillar lymph nodes were excluded.
CEUS real time guided SLN-FNA
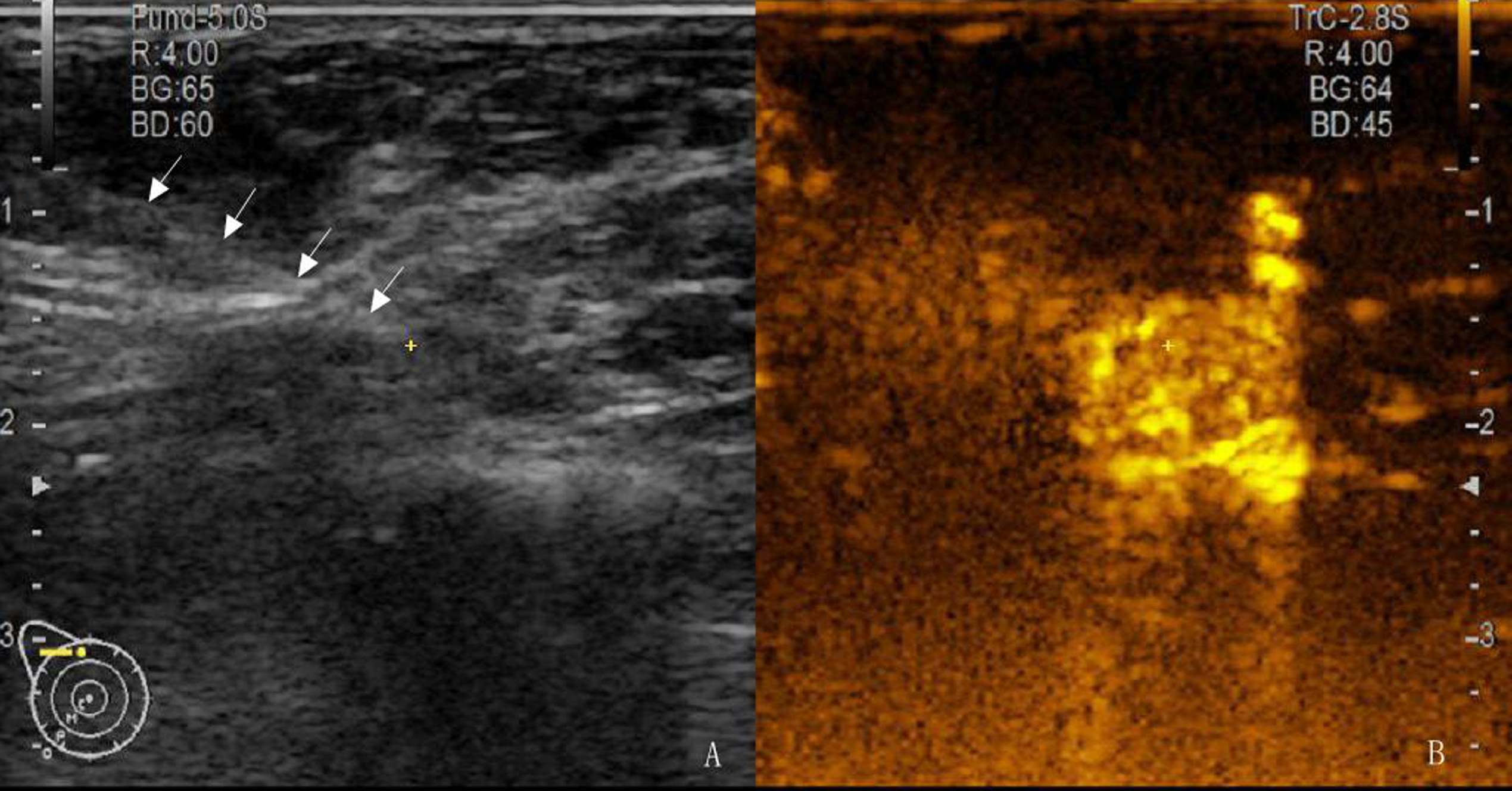
Conventional ultrasound examination of breast and axilla was performed using the Hitachi Arietta 70 (Hitachi medical, Japan) before intradermal CEUS with a linear phased-array transducer (L64, 18-5MHz). Tumor features of conventional ultrasound were recorded, and the tumors were classified into different categories according to ultrasound Breast Imaging Reporting and Data System (BI-RADS US) issued by American College of Radiology in 2013 [26]. CEUS imaging was performed with another lower frequency linear phased-array transducer (L34, 7-3MHz). The using of CEUS was permitted by the local institutional ethics committee of Beijing Friendship Hospital, Capital Medical University (Code:2017-P2-156-02). Ultrasonic microbubble were prepared by mixing 59 mg Sulphur hexafluoride powder (Bracco Imaging SpA, Naples, Italy) and 5 ml sterile saline, and vigorously shaking no less than 15 s. After injection intradermally into 3, 6, 9, 12 o’clock near the areola with 0.5 ml per point, gently massage was performed on the injection site to facilitate movement of CEUS agent into the lymph nodes. CEUS examination then started. The screen was divided into left and right parts real time imaging of scanning zone. The left was grayscale imaging mode with a consistent MI of 0.07, the right was contrast-enhanced imaging mode with a consistent MI of 0.09 (Fig. 1). Tracking the enhanced lymphatic ducts from areola to axilla, the first enhanced lymph node(s) was (were) identified as the SLN(s). Related ultrasonography and intradermal CEUS were performed by three experienced senior doctors. Two experienced senior nurses performed injection of microbubble. In theory, there may be risks of injection such as induration, bleeding, bent or broken of needles, and allergies. In fact, only 4 patients experienced slight bleeding at the injection site and stopped the bleeding after a short period of compression. There were no other adverse reactions.

A 61 years old woman breast cancer patient in right breast. Dual display of a sentinel lymph node (SLN) of intradermal contrast-enhanced ultrasound. (a) SLN was difficult to distinguish in conventional ultrasound. (b) A enhanced lymph node clearly displayed after intradermal injection of contrast agent near the areola (arrow).
When CEUS identified the SLN, one doctor hold the probe and another doctor performed the FNA procedure according to the real time dual CEUS image mode with 25G puncture needle (Hakko, Osaka, Japan) (Fig. 2). The number of lymph nodes shown by CEUS model, that can be shown by grey scale model and that cannot be shown by gray scale model were recorded in detail. Multipoint FNA performed on each SLN according to dual CEUS image mode. The suspected areas of SLN were sufficiently biopsied. All cytological smears were read by the same team of cytopathologists. Negative FNA results defined as no tumor cell found in all slices. When a tumor cell was found in any slice of a case, the FNA results defined as positive (Fig. 3).
Contrast enhanced ultrasound real-time guided fine needle aspiration procedure for the same patient of Fig. 1. (a) The needle was clearly displayed in gray-scale image. (b) The enhanced sentinel lymph node. The synchronous yellow cursor of left and right imaging was helpful to confirm whether the needle tip is in the sentinel lymph node.
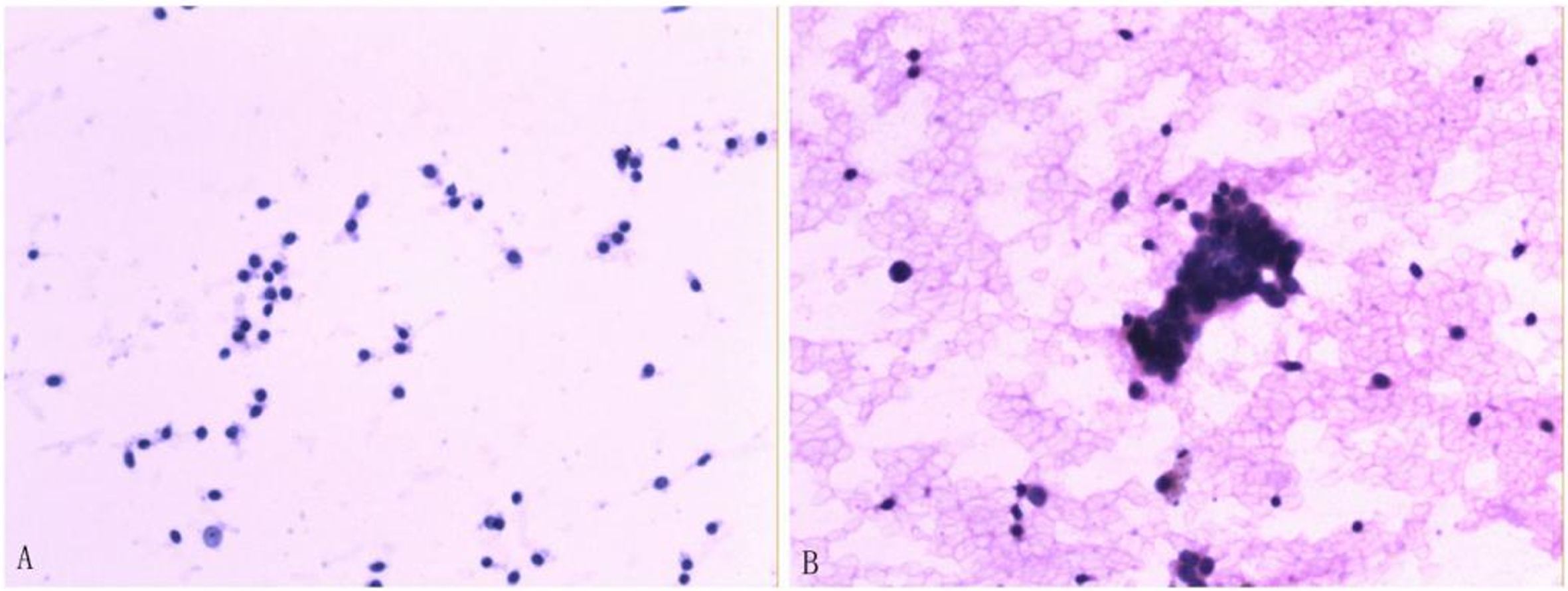
Cytologic smear of the sentinel lymph node (SLN) specimen. (a) Lymphocyte but none tumor cells were identified within the node (hematoxylinand eosin, ×200). (b) Tumor cells were found within the node (hematoxylin and eosin, ×200).
Within 48 h after FNA, intraoperative SLNB was performed by two experienced senior surgeons during breast tumor resection. One ml 1%methylene blue (Jiangsu Jumpcan Pharmaceutical Co., Taixing, Jiangsu, China) was used as tracer agent. Five minutes later of intradermally injection near the areola, the surgeon explored and removed the first blue-stained lymph node(s). The aforementioned lymph nodes were regarded as SLNs and frozen for fast pathological examination. The removed SLNs were fixed with 10%buffered formalin and sectioned into 2 mm slices for final histopathological examination. Histopathological results were diagnosed by the same team of histopathologists and were considered as gold standard for final diagnosis of SLN metastasis.
Statistical analysis
Analyses were performed with SPSS, standard version 17.0 (IBM, Armonk, NY, USA). Skewed distribution data assessed with Wilcoxon signed-rank test. Sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), false-negative rate (FNR), false positive rate (FPR) and Youden Index (YI) were used to assess efficiency of axillary metastatic status diagnosed by SLN-FNA. All differences were considered to be statistically significant at probability (p) value < 0.05.
Results
Characteristics of patients
From December 2018 to November 2019, a total of 26 patients performed CEUS real-time guided SLN-FNA, of which 2 patients refused surgical treatment, one patient performed tumor resection without SLNB and ALND, 2 patients performed unilateral mastectomy + ALND without SLNB. Finally, twenty-one patients age of 40–77 y (59.4±8.7) were included in present study, of which 15 patients were T1 and 6 patients were T2. The location of mass were 14 patients in left breast and 7 patients in right. The number of tumor were one tumor in 19 patients, 2 tumors in one patients and three tumors in one patients. According to ACR BI-RADS-US classification, 5 tumors were BI-RADS-US 4A, 5 tumors were BI-RADS-US 4B, 10 tumors were BI-RADS-US 4C, and 4 tumors were BI-RADS-US 5. Twenty tumors were invasive ductal carcinoma, 1 tumor was lobular carcinoma in situ and 3 tumors were ductal carcinoma in situ. Three tumors were divided into pathologic histology grade 1, 17 tumors were divided into grade 2 and 4 tumors were divided into grade 3. The characteristics were summarized in Table 1.
Clinical and pathological characteristics of 21 patients
Clinical and pathological characteristics of 21 patients
BI-RADS US = ultrasound Breast Imaging Reporting and Data System.
Intradermal CEUS identified 26 SLNs in all 21 patients. Among them, one SLN was identified in 18 patients, two SLNs were identified in 1 patient, and 3 SLNs were identified in 2 patients. The median CE-SLN was 1. A total of 130 SLNs were detected by SLNB, of which 1 SLN was detected in 1 patient, 3 SLNs were detected in 3 patients, 4 SLNs were detected in 2 patients and≥5 SLNs were detected in 15 patients. The median SLN detected by SLNB was 5. Compared to intradermal CEUS, SLNB detected more SLNs (p < 0.001) (Table 2).
Comparison of detections of SLN between intradermal CEUS and SLNB
Comparison of detections of SLN between intradermal CEUS and SLNB
CEUS = contrast enhanced ultrasound; SLNB = sentinel lymph node biopsy; SLN = sentinel lymph node.
All the 26 SLNs of 21 patients can be showed by CEUS mode, including 5 SLNs (19.2%) of 4 patients were difficult to distinguish in grey scale mode because of the echo was close to the surrounding tissue. Finally, all 26 SLNs of 21 patients were successfully performed FNA by dual CEUS image mode real time guiding. Cytopathology reported that cancer cells were found in 3 SLNs of 2 patients. Of the 130 SLNs in 21 patients detected by SLNB during the operation, histopathological examination reported that 8 SLNs of 5 patients were positive (Table 3). These five patients all performed ALND. Three cases didn’t find additional metastatic lymph node in the axillary specimen. The other 2 patients both had one metastatic lymph node in the removed axillary specimen. Compared to SLNB, FNA found 2 of 5 cases of SLN metastasis, the diagnosis sensitivity, specificity, PPV, NPV, FNR, FPR and YI were 40%, 100%, 100%, 84.2%, 60%, 0%and 40%, respectively.
Sentinel lymph node positive cases of CEUS guided FNA and SLNB
Sentinel lymph node positive cases of CEUS guided FNA and SLNB
CEUS = contrast enhanced ultrasound; FNA = fine needle biopsy; SLNB = sentinel lymph node biopsy.
It was reported that several factors were related to breast cancer ALNM such as large tumor size, non-special type of invasive cancer, high histological grade, high Ki-67, Her-2 positive and vascular invasion, etc. The larger the volume of breast cancer, the faster the tumor cell proliferation, the longer the tumor growth time, and the greater the possibility of ALNM in the infiltrating lymphatic vessels [27–29]. The morphology of the tumor reflected the growth pattern of the tumor. The irregular morphology was the characteristic of tumor invasive growth. Due to the rapid growth rate, tumor cells can easily invade the lymphatic vessels, resulting in ALNM [30, 31]. According to pathology, the appearance of crab feet or burr-like growth on the edge of the tumor may indicate that the tumor cells were highly invasive to surrounding tissues and lymphatic vessels. Neovascularization can provide necessary nutrients for tumor cells to maintain their growth and invasion ability. Tumor cells with strong invasion ability were easy to destroy surrounding normal tissues and invade lymphatic vessels, resulting in ALNM.
A variety of imaging methods were used to assess the status of ALN in breast cancer. The advantages of ultrasonography were convenience, non-invasiveness, and economy, but it was highly dependent on the operator and difficult to diagnose deep lymph nodes. CEUS with ultrasound contrast agent bolus injected through elbow vein can be used to observe the microcirculation of lymph nodes and evaluate whether lymph nodes of breast cancer patients were involved. The diagnostic efficacy had been improved, but it still lacked objectivity and increased additional cost [32].
MRI had the advantages of high soft tissue resolution, multi-sequence, multi-angle imaging and harmless to human body. Diffusion-weighted imaging (DWI) was a non-invasive method to detect the diffusion movement of water molecules in a living body, and it can reflect the limited movement of water molecules in the tissue to a certain extent. The area where diffusion was restricted on DWI images will appear as high signal. The low apparent diffusion coefficient (ADC) can quantify the diffusion of water molecules. ADC value and ADC ratio were used to distinguish between ALNM and non-metastatic ALN. But there was no uniform standard for the threshold of ALNM, and further research was needed [33–35]. Dynamic contrast-enhanced magnetic resonance imaging (DCE-MRI) scans while rapidly injecting a contrast agent to reflect changes in the microcirculation, perfusion, and capillary permeability of the diseased tissue. Previous studies have pointed out that DCE-MRI cannot be used as an accurate basis for diagnosing ALNM due to its low specificity, but DCE-MRI had a very high NPV and can be used to rule out ALNM [36]. In addition, DCE-MRI still had the disadvantages of long scanning time and the scanning image was affected by respiratory motion. In recent years, scholars had applied the new contrast agent ultrasmall superparamagnetic iron oxide (USPIO) to the evaluation of breast cancer ALN. Lahaye et al. found that the sensitivity and specificity reached 93%and 96%, respectively [37]. Further study was also needed.
Positron emission tomography/computed tomography(PET/CT) can also assess the status ALN of breast cancer. Fluorodeoxyglucose (FDG) intake was detected by PET/CT for diagnosis of lymph node involvement. High fluorodeoxyglucose (FDG) intake indicated the possibility of invasion of malignant cells. It was reported that this method has low sensitivity and high specificity for the diagnosis of ALNM. However, as a whole body imaging examination, PET/CT can scan the chest, abdomen, bones and other systems at the same time. It was more accurate than bone scans in detecting the presence or absence of bone metastasis. Therefore, the main significance of PET/CT in the preoperative examination of breast cancer patients was to determine whether the internal mammary lymph nodes, supraclavicular lymph nodes, parasternal lymph nodes and distant organs have metastasis [38, 39].
In the 21st century, SLNB was considered as a infusive improvement of breast surgery. It was a routine procedure to assess the status of ALN in breast cancer patients [7, 8]. Generally, blue dye and isotope were used as tracer of SLNB. Blue dye was easy to overstain the lymphatic tissue because of the small molecular weight, which lead to excessive removal of nonSLNs. The tracer commonly used in radio nuclide method was a radiopharmaceutical containing technetium. According to literature reports, the detection rate of different radiotracers was slightly different, but they were all higher than 97%[40–42]. The radio nuclide method can clearly trace the lymph vessels and lymph nodes, but the radioactivity was strong, the intraoperative positioning equipment was expensive and the operation was complicated, and the processing of surgical specimens must be strictly implemented in accordance with relevant regulations [43]. Thus, a more accurate, safe and less invasive tracer to identify SLN was needed.
Contrast enhanced ultrasound can provide more diagnosis information via enhance the tissue microvasculature by intravenous injection of contrast microbubble. It had been widely used for several years. Fischer et al. and Wiesinger et al. reported that CEUS, including perfusion imaging, was widely used in the field of spleen alterations, focal liver lesions, cystic renal lesions, testicular pathologies, assess the efficiency of thermal ablation and irreversible electroporation, and so on [44, 49]. In 2004, Goldberg et al. first reported the successful lymphatic ultrasonography in a swine melanoma model after injection ultrasonic microbubbles around the tumor [50]. The followed clinical studies involved CEUS and SLN of breast cancer patients were carried out and reported that CEUS detected SLN and the median CE-SLN was usually 1, which was significantly less than the median SLN of conventional method [23, 51]. Cui et al. revealed that compared to non-CE-SLNs, CE-SLNs were more positive of metastasis, indicating that CE-SLN may be more specific and accurate [52]. In the present study, methylene blue was used as a tracer of SLNB, and a total of 130 SLNs were detected in 21 patients (median SLN = 5), of which 8 SLNs in 5 patients were confirmed to be positive lymph nodes. In comparison, CEUS-SLN-FNA detected 26 SLNs in 21 patients (median SLN = 1, of which 3 lymph nodes in 2 patients were confirmed to be metastatic lymph nodes. Although there was no significant difference in the ratio of positive SLNs detected between these two procedure (p = 0.394), it was sufficient to explain the overstaining problem of methylene blue as a tracer, resulting in too many negative lymph nodes to be removed. In comparison, CEUS was more accurate to identify SLN.
In the literature that CEUS used to assist SLN-FNA, the role of CEUS was to identify SLN, especially in the case of lymph nodes that were not easily displayed by conventional ultrasound. Sever et al reported that 40%of the presumed SLNs were identified only on the CEUS imaging mode, and Zhong et al. reported that 31.7%of the suspected lymph nodes were considered to be suspicious SLNs only after contrast agent injection [23, 24]. In this study, five of 26 SLNs were identified only after microbubble injection. Due to the low mechanical index in contrast-enhanced ultrasound mode, it will affect the clarity of the image and may affect the observation of the needle position during FNA procedure. Therefore, it has been reported in the past that the conventional ultrasound mode was often used to guide the procedure. However, some SLNs were difficult to identify due to their deep location or the similar echoes of the surrounding tissues on conventional ultrasound. At this time, the high contrast ratio between lymphatic and surrounding tissue under the intradermal CEUS imaging mode can clearly show the lymphatic ducts and lymph nodes. The present study tried to use intradermal dual CEUS image mode to guide sentinel lymph node needle aspiration cytology biopsy in real time, which proved that this procedure was technically achievable, especially for lymph nodes which were difficult to distinguish by conventional ultrasound. Contrast-enhanced ultrasound can better display lymph nodes, and further FNA was completed under the real-time guidance of CEUS. In dual CEUS image mode, enhanced imaging can clearly show the enhanced SLN, and the gray-scale imaging can clearly show the needle. The synchronous cursor of left and right imaging was helpful to confirm whether the needle tip is in the SLN (Fig. 2). In this study, 26 lymph nodes of 21 patients were successfully implemented FNA under intradermal dual CEUS image real-time guidance. Among them, 5 SLNs of 4 patients were not clearly displayed on conventional ultrasound. If only conventional ultrasound was used for guidance, we would not be able to biopsy these lymph nodes, intradermal dual CEUS image real-time guidance helped us solve this problem.
Generally, further ALND was unnecessary according to negative SLNB results. In line with American College of Surgeons Oncology Group (ACOSOG) Z0011 criteria, further ALND also can be avoided for breast cancer patients with low-risk SLN metastasis, such as micrometastases or 1-2 macrometastases [53]. Nevertheless, in China, further treatment may not be completely consistent with the ACOSOG Z0011 criteria when a positive SLNB result was acquired. Miao et al. reported that ACOSOG Z0011 criteria was a good exportability to avoid unnecessary ALND for Chinese patients, but this criteria was not strictly enforced as national treatment guideline in China [54]. Liu et al. reported that the Western nomogram and calculator for predicting non-SLN metastasis did not perform as well as in Chinese breast cancer patients [55]. This results indicated that breast cancer patients were different between Chinese and Western populations. Additionally, in consideration of insufficient standard adjuvant treatment after surgery in suburban areas and worrying about recurrences, some Chinese surgeons and patients were more conservative to perform ALND for any SLNB positive cases [54]. Therefore, indications for ALND were less rigid in China than in Western countries.
To some extent, the trauma associated with ALND had been reduced by application of SLNB. Nevertheless, it was also an invasive procedure with non-negligible FNR [56]. As an minimally invisive diagnosis method of lymph node metastases, intradermal dual CEUS image real-time guided SLN-FNA was a potential procedure to assess ALN status preoperatively, which will reduce intraoperative SLNB need. This study found that the PPV of CEUS real-time guidance of SLN-FNA in diagnosis of SLN metastatic in breast cancer patients was 100%. FNA detected 2 positive cases, both of which were positive for SLNB. According to Chinese surgeons and patients’ conservatism of positive SLN cases, this results suggested that surgeons should directly perform ALND in FNA-positive patients. Thus, the use of CEUS real-time guidance SLN-FNA before operation as a less invasive operation in a non-anesthetic state can shorten the anesthetic time and reduce the additional surgical trauma caused by unnecessary SLNB.
The FNR of intradermal dual CEUS image real-time guided SLN-FNA cannot be ignored. Zhong et al. reported that the application of CEUS to assist sentinel lymph node FNA has high accuracy and extremely low FNR, and suggested that this method was potentially as reliable as SLNB [23]. But Sever et al. reported that the FNR was 8%, which should not be ignored [24]. In this study, the FNR was higher to 60%. Although only 1 or 2 metastatic SLNs were found in the 3 false negative patients, metastatic lymph nodes were found in the ALND specimens. Taking into account the population characteristics of Chinese patients and the conservative attitude of Chinese doctors, it was recommended that patients with negative CEUS-SLN-FNA results should take a prudent procedure for intraoperative SLNB.
This retrospective analysis has several limitations. Above all, there was no T3 stage breast cancer patients in present study. Patients with history of radiotherapy, neo-adjuvant chemotherapy, related surgery of corresponding breast or axilla were not suggested to CEUS-SLN-FNA accounting to the disturbance of the drainage of microbubble to the SLN. Thus, the efficiency of the proposed procedure may be influenced by selection bias. It might be a potential reason of the higher FNR. Otherwise, the present study was carried out just in a single center of a small sample with 21 breast cancer patients. A prospective multicenter large sample research is needed to verify our opinion.
The additional cost of CEUS-SLN-FNA before surgery cannot be ignored, because some patients still need SLNB after this procedure. However, positive patients who skipped SLNB and performed ALND directly avoided waiting for rapid freezing pathological results under anesthesia during SLNB and reduced additional trauma caused by SLNB. Moreover, this procedure is easy to operate, a well-trained team can complete the operation within 10–20 min. Of course, this requires examiners to be proficient in ultrasound, including CEUS, as well as FNA under ultrasound guidance, which limits the application and popularization of this technology to a certain extent.
In conclusion, SLN-FNA real time guided by dual CEUS imaging mode was technically feasible. SLNs that difficult to distinguish by conventional ultrasound identified and biopsied successfully by this procedure. Patient with a positive SLN-FNA should be advised to ALND without intraoperative SLNB according to Chinese surgeon and patients’ conservatism attitude. But a negative SLN-FNA did not obviate the need of conventional SLNB because of the FNR. Otherwise, prospective multicenter large sample research was needed to verify our opinion.
Funding
Beijing Municipal Administration of Hospital’s Ascent Plan, Code: DFL20180102.
Conflict of interest
None.
Ethical statement
This retrospective study was approved by the local institutional ethics committee of Beijing Friendship Hospital, Capital Medical University (Code: 2020-P2-177-01).
Footnotes
Acknowledgments
This study was supported by Beijing Municipal Administration of Hospital’s Ascent Plan (Code: DFL20180102). We express our special appreciation to Miao Wang and Xiaomeng Yu for providing cytological figures.